
Hypertrophic cardiomyopathy (HCM) is a common inherited heart disease with diverse phenotypic and genetic expressions1. Although often compatible with a normal life expectancy, some patients are at increased risk of significant complications, such as progressive heart failure, arrhythmias, and ischemia2,3. The co-existence of acquired cardiovascular diseases adds complexity to patient management. Multimodal imaging has emerged as a critical tool in this context, offering comprehensive risk assessment and aiding in the formulation of tailored therapeutic strategies4. This report emphasizes the diagnostic and therapeutic impact of advanced imaging in the management of HCM.
We present the case of a 50-year-old female, a current smoker, admitted to our clinic for mild exertional dyspnoea, progressively worsening for three months. She was diagnosed with non-obstructive HCM with preserved systolic function and second-grade diastolic dysfunction fifteen years ago.
Regarding her family history, her mother was diagnosed with HCM, and her maternal grandmother died suddenly at 40 years of age.
At admission, the patient had a regular heart rate (HR) of 80 bpm, a grade III/VI systolic murmur extending from the left parasternal to the apical regions, normal bilateral blood pressure of 135/70 mmHg, and normal O2 saturation, with no signs of systemic or pulmonary congestion or hypoperfusion. The electrocardiogram (ECG) showed a normal sinus rhythm of 60 bpm and LV hypertrophy criteria (R wave of 40 mm in aVL, Sokolov-Lyon index of 45 mm, and down-sloping ST-T abnormalities). The routine blood workup showed an elevated NT-proBNP of 8833 pg/mL and hyperuricemia. The transthoracic echocardiography (TTE) revealed LV wall hypertrophy (interventricular septum of 26 mm, posterior wall of 26 mm) with medio-ventricular obstruction, alongside an apical aneurysm and akinesis of the basal segments of the inferior and inferolateral LV walls, with moderate LV systolic dysfunction and an LVEF of 35% (Figure 1). Given the unusual segmental LV systolic dysfunction pattern and the hourglass shape, a contrast TTE was performed for more precise evaluation, confirming severe LV systolic dysfunction (Figure 2). Continuous-wave (CW) Doppler analysis of mid-LV obstruction showed an interruption of blood flow from the LV apex to the base during mid-systole (void pattern), followed by a paradoxical jet from the aneurysm in late systole-early diastole (Figure 1).
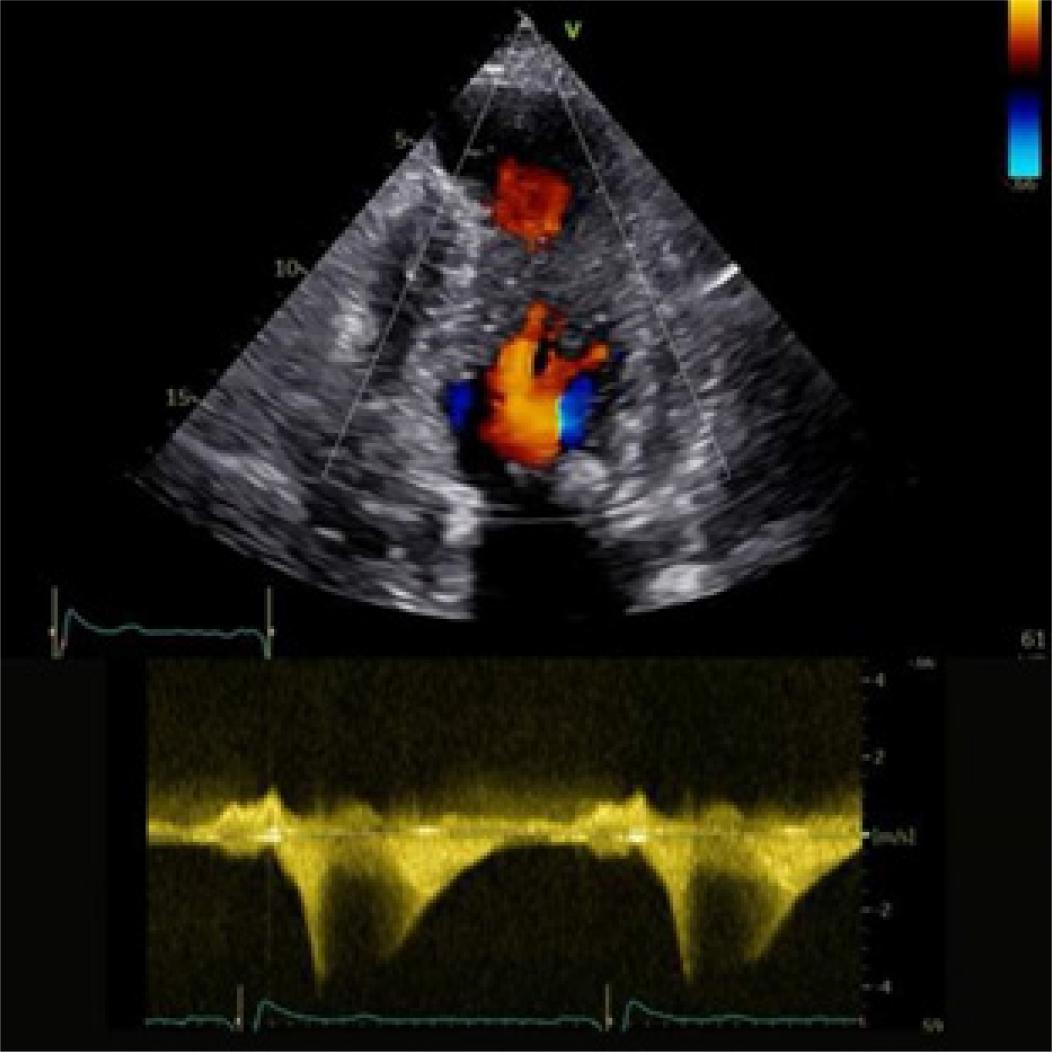
CW Doppler analysis of mid-LV obstruction showed an interruption in blood flow from the LV apex to the base during mid-systole (void pattern), followed by a late systole to early diastole paradoxical jet flowing out of the aneurysm.
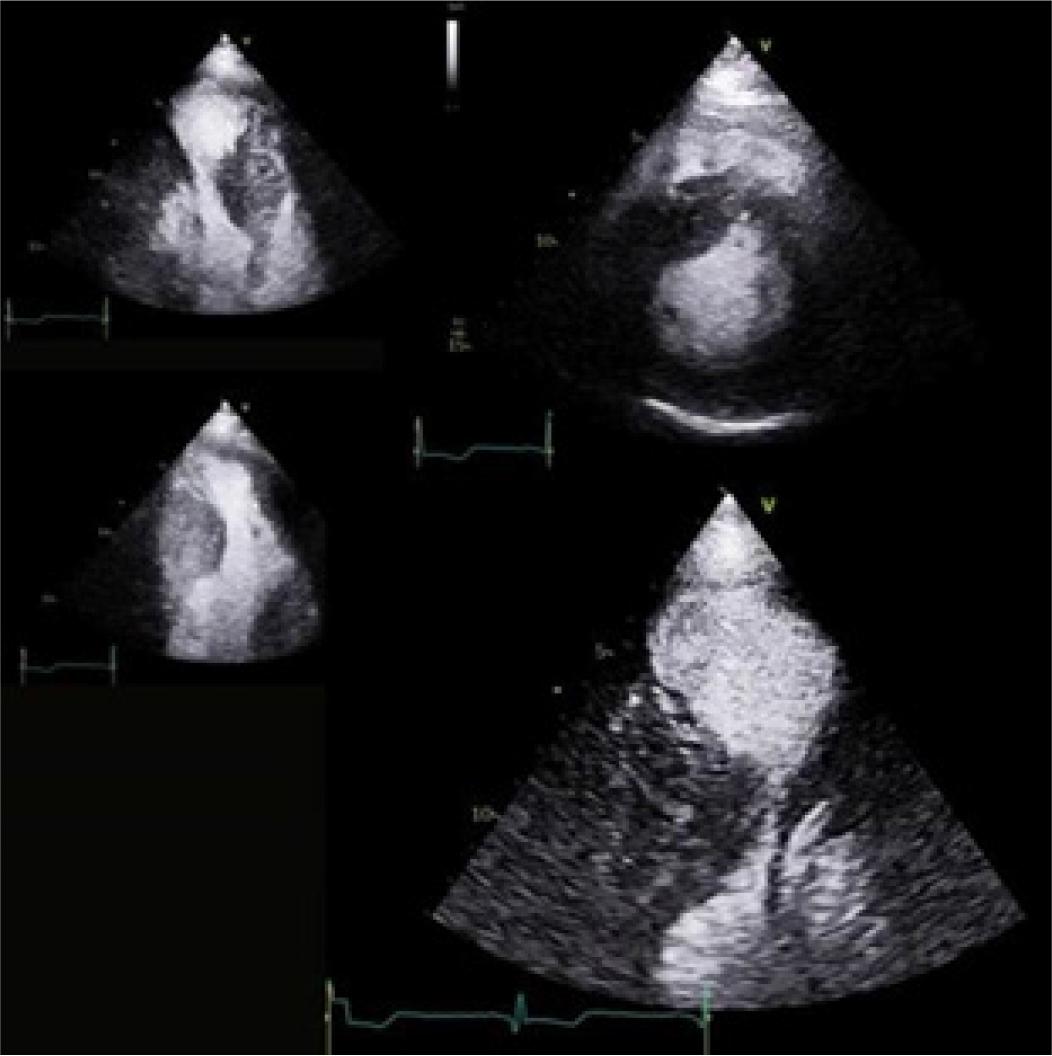
Contrast echocardiography was used to accurately assess the endocardial border and characterize the apical aneurysm, revealing moderate systolic dysfunction.
Contrast-enhanced cardiac magnetic resonance (CMR) was performed to accurately assess cardiac structure and function, and to characterize myocardial tissue4. This imaging technique confirmed HCM, with significant mid-segment hypertrophy of the interventricular septum measuring 28 mm, a large apical aneurysm (maximum diameter of 4 cm) without thrombosis, severe systolic dysfunction (LVEF of 25%), and a medio-ventricular obstruction (Figure 3). The late gadolinium enhancement (LGE) CMR sequence revealed 16% fibrosis of the LV myocardial mass, primarily in the apical aneurysm and the mid-segment of the lateral and inferolateral walls, consistent with a burnout HCM phenotype. Moreover, the CMR showed a subendocardial infarct with viability in the inferior and inferolateral basal segments (Figure 3).
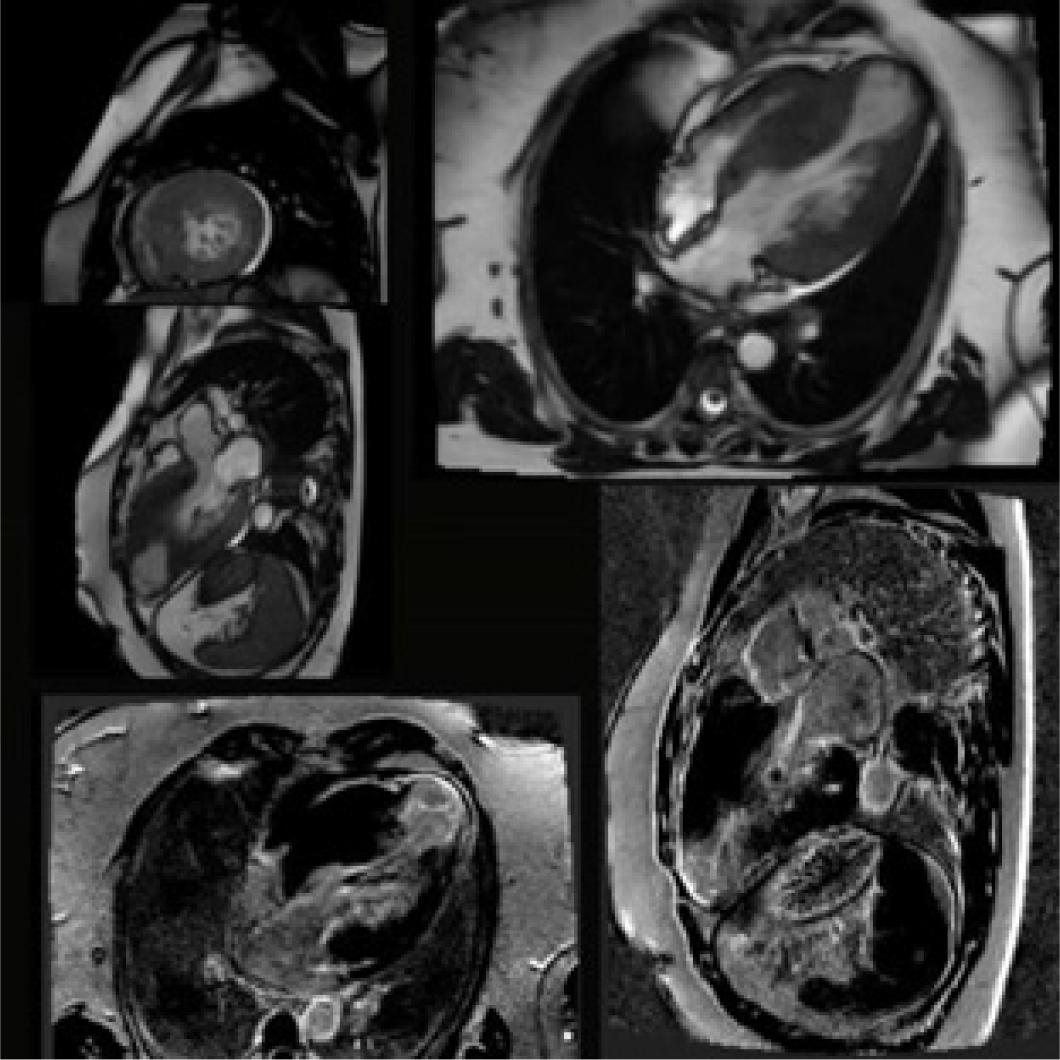
Cardiac MRI confirms medio-ventricular HCM in the burn-out stage with severe systolic dysfunction, 16% LGE of LV myocardial mass predominantly at the level of the apical aneurysm, and subendocardial fibrosis in the inferior and inferolateral walls, suggesting myocardial viability.
Given the significant myocardial viability identified on contrast-enhanced CMR, we performed coronary angiography. This revealed a significant 80% stenosis in the second segment of the right coronary artery, along with 50% stenosis in the mid-to-distal segments of the left anterior descending coronary artery (LAD). Therefore, myocardial revascularization with a drug-eluting stent was performed, with good post-interventional results (Figure 4).
Echocardiography and speckle tracking imaging showed improved regional kinetics after revascularization, but persistent severe global longitudinal dysfunction, especially at the medio-ventricular and apical levels.
Given the positive family history of HCM and SCD, along with a Class Ic indication according to the ESC Guidelines for the Management of Cardiomyopathies4, genetic testing was performed using next-generation sequencing of a panel of 174 genes potentially involved in cardiomyopathies, yielding a negative result. A negative result does not rule out the diagnosis of HCM, which is otherwise suggested by tissue characterization on CMR. Instead, it draws attention to the possibility of as-yet-unidentified abnormal variants associated with the hypertrophic phenotype. Nevertheless, despite the genetic test results, her family is advised to undergo clinical screening, and further testing with WES may be undertaken.
The medical treatment aimed to provide prognostic-targeted therapy in HF with reduced LVEF, comprising a beta-blocker (metoprolol succinate 100 mg o.d), a mineralocorticoid receptor antagonist (spironolactone 25 mg o.d), ARNIs (sacubitril/valsartan 24/26 mg b.i.d), and an SGLT2 inhibitor (dapagliflozin 10 mg o.d) (5). Additionally, dual antiplatelet therapy (aspirin 75 mg o.d and clopidogrel 75 mg o.d, daily for up to 6 months) and a high-dose statin (atorvastatin 80 mg o.d) were initiated.
While the ESC guidelines do not specifically endorse routine anticoagulation for HCM patients with apical aneurysm, the literature supports a low threshold for considering anticoagulation in this high-risk group, particularly for aneurysms ≥2 cm or in the presence of thrombus11, 12. In our case, although the apical aneurysm measures 4 cm, we opted not to initiate anticoagulation at this time, given the absence of thrombus on CMR and contrast echocardiography. We will reconsider this decision based on findings from routine periodic follow-up with ECG Holter monitoring and echocardiographic imaging.
According to the ESC HCM and Cardiomyopathy Guidelines, intracardiac defibrillator implantation is indicated as primary prophylaxis for SCD in patients with an intermediate arrhythmic risk associated with HCM of 4.28% and at least one additional risk factor: myocardial fibrosis exceeding 15% on CMR, apical aneurysm, and systolic LV dysfunction4. This intervention was delayed for three months after myocardial revascularization in our patient, given the possibility of improvement in LV systolic function5.
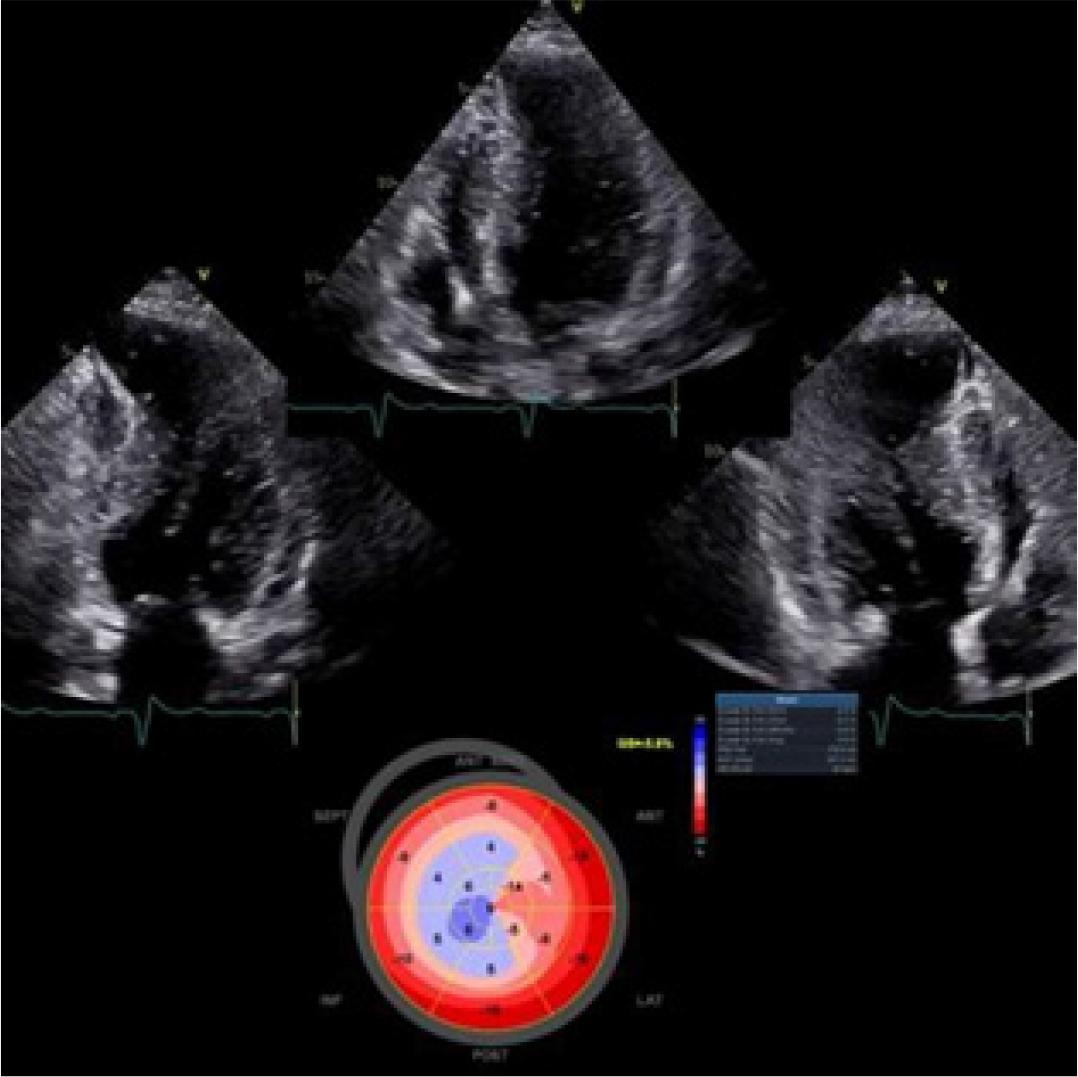
At the three-month follow-up after myocardial revascularization, the patient remained symptomatic, but NT-proBNP had decreased to 2200 pg/mL. The TTE revealed LV remodeling with an hourglass shape and persistent systolic dysfunction assessed by three-dimensional volumetry, with an EF of 36% (Figure 5). A persistent void pattern was also observed during continuous-wave (CW) Doppler interrogation of the LV, with near-complete cessation of flow for more than 50% of LV systole. Therefore, medical treatment was optimized by increasing the beta-blocker dose to reduce the medio-ventricular gradient (the resting gradient reached up to 52 mmHg). The ARNI dose could not be up-titrated due to low blood pressure, which was exacerbated by dynamic medio-ventricular obstruction.
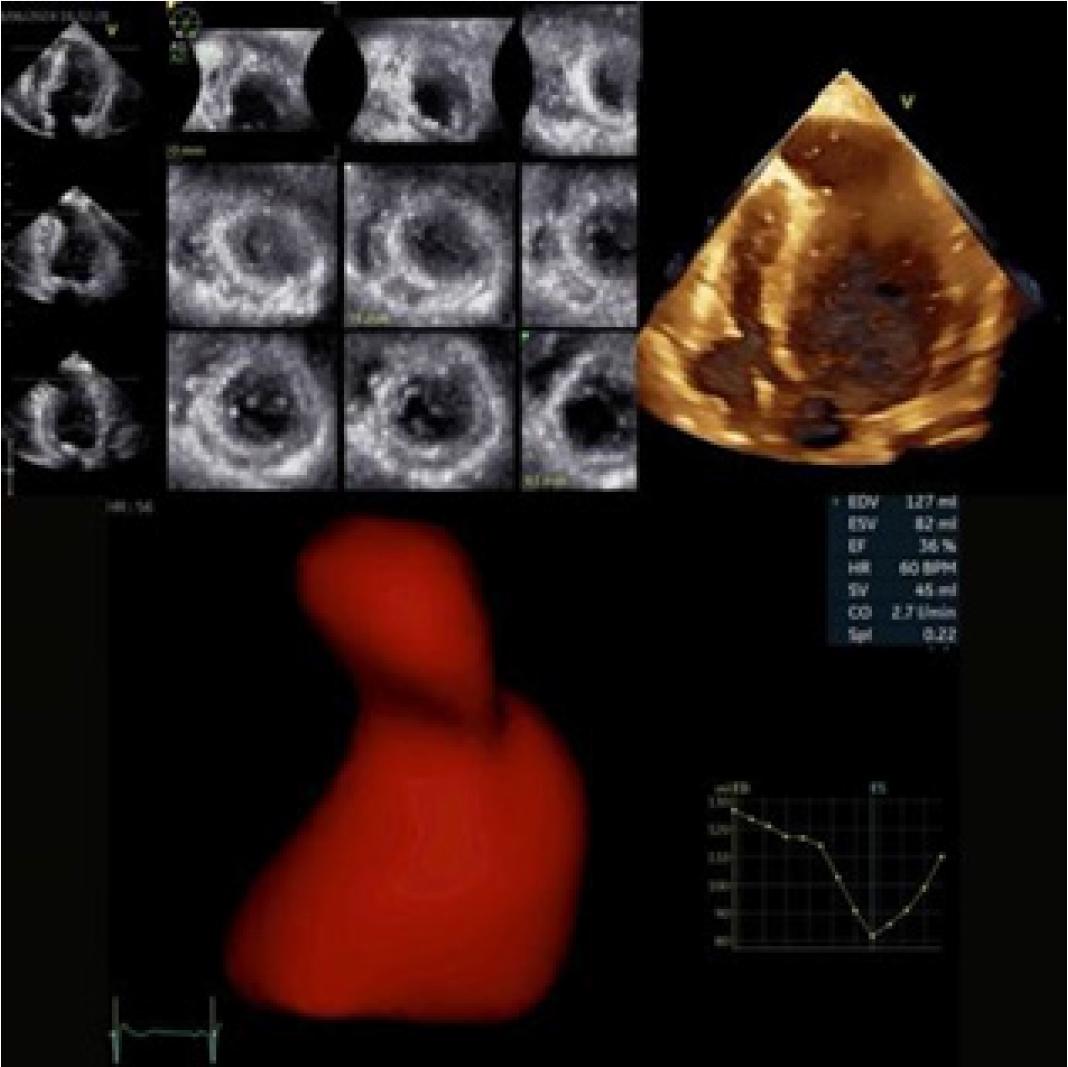
The follow-up echocardiogram highlighted a remodelled LV with an hourglass shape, moderate systolic dysfunction assessed by 3D volumetry with an EF of 36%.
While the ESC guidelines4 do not specifically endorse routine anticoagulation for HCM patients with an apical aneurysm and no atrial fibrillation, we will consider anticoagulation based on findings from routine periodic follow-up with ECG Holter monitoring and echocardiographic imaging. We opted not to initiate anticoagulation at this time, given the absence of thrombus on CMR and contrast echocardiography.
In our case, an ICD was recommended for primary prevention of sudden cardiac death per current guidelines4,5. The decision was based on both the burnout stage of HCM and persistent severe LV systolic dysfunction despite revascularization and optimization of medical treatment. As a result, the ICD was successfully implanted without complications.
Due to the unpredictable nature of HCM disease progression, periodic assessments are essential to monitor changes in clinical status and risk profiles. Ongoing follow-up and continuous treatment optimization remain crucial to improving long-term survival.
CMR combines the advantages of being non-invasive and independent of acoustic windows with its ability to characterize myocardial tissue6. Therefore, it is recommended in the 2023 ESC Guidelines for managing cardiomyopathies, with a Class IB indication for patients with HCM4. In this case, CMR with LGE sequences revealed mid-ventricular HCM with significant fibrosis, accounting for 16% of LV mass, predominantly distributed at the level of the apical aneurysm. Additionally, subendocardial myocardial fibrosis, involving less than 50% of wall thickness, was identified in the lateral and inferolateral basal segments, suggesting a possible ischemic etiology with viable myocardium in these regions. Although other investigations, such as myocardial scintigraphy, could have provided similar information about viability, their results in this case may be limited by increased mid-ventricular obstruction and arrhythmic risk associated with exertion. Moreover, identifying myocardial fibrosis and viability has significant therapeutic implications. The patient benefited from myocardial revascularization with a drug-eluting stent (DES) and subsequently received a prophylactic ICD.
Clinicians routinely face the decision of whether revascularization would be beneficial for patients with CAD and significant LV systolic dysfunction7. By directly visualizing scars and evaluating their transmural extent with LGE, CMR offers a unique advantage over other modalities as a central player in viability assessment8. It should be considered a feasible technique, especially in HCM patients.
The second aspect of this case concerns the complex mechanism of apical aneurysm remodelling. Severe mid-LV obstruction leads to cessation of mid-systolic flow, trapping blood in the apical chamber, increasing wall stress, and producing afterload mismatch and ischemia9,10. Additionally, a hemodynamically significant atherosclerotic lesion further reduces oxygen supply. Thus, this case illustrates the dual mechanism of apical aneurysm formation, involving mid-ventricular obstruction, evidenced by CW Doppler interrogation revealing a persistent void pattern, and serial non-significant mid-to-distal LAD stenosis, compounded by pre-existing microvascular ischemia, which is frequently encountered in patients with HCM. Therefore, patients with severe mid-ventricular obstructive HCM and akinetic apical aneurysms may require tailored therapeutic measures9,10. These could include progressive uptitration of beta-blockers, the addition of calcium-channel blockers, or even novel negative inotropic agents, alongside revascularization and optimized medical therapy to address atherosclerotic disease. Follow-up for thrombotic risk at this level is essential, and contrast echocardiography can be a valuable adjunct imaging tool.
HCM is a complex disease whose course can be unpredictable, progressing toward aneurysm formation and end-stage disease, with marked changes in its clinical profile and the adoption of effective, diverse management strategies. Advancements in multimodality imaging and genetic testing have reshaped its clinical picture and contributed to its progression, preventing sudden death and reversing heart failure, resulting in improved quality of life and extended longevity for many patients1. HCM has transformed into a treatable cardiovascular disease in modern times.
Multimodal imaging, particularly CMR with LGE, was pivotal in managing HCM in this case, revealing myocardial fibrosis and viability. These findings guided both revascularization and ICD placement.
Apical aneurysm resulted from both mid-ventricular obstruction and ischemia, highlighting the need for an individualized, multimodal approach—combining revascularization, medical therapy, and ICD placement.
This case demonstrates the transformative role of multimodal imaging in HCM management, providing valuable information on myocardial viability and guiding clinical decision-making. Continuous monitoring and ongoing therapy optimization remain essential to address the unpredictable nature of HCM and improve patient outcomes.