Neuroendocrine tumors, with an incidence in the general population of 2.5-5/100.000/year, are rare malignancies that most commonly originate in the gastrointestinal tract1–3. NETs may secrete various vasoactive substances, including serotonin, histamine, prostaglandins, or bradykinin. When these products exceed the hepatic capacity for degradation, carcinoid syndrome ensues4–6. Up to 50% of patients with carcinoid syndrome (CS) develop carcinoid heart disease (CaHD)2. Carcinoid heart disease is initially well tolerated, but it represents a major cause of morbidity and mortality2.
The disease diagnosis and management pose a significant challenge because of the heterogeneous clinical presentations and poor prognosis7. Transthoracic echocardiography is the gold standard for diagnosis1, but cardiac magnetic resonance and computed tomography may be valuable adjuncts in investigating patients with the disease2. Managing carcinoid heart disease involves a holistic approach, developed based on the expert opinion of a multidisciplinary consensus, including endocrinologists, oncologists, cardiologists, and cardiothoracic surgeons2.
We hereby present the case of a 53-year-old female patient who was admitted to the hospital for dyspnea and fatigability on a moderate effort. The patient’s history revealed premature menopause (at 39 years old), ankylosis spondylitis, uterine fibroids with total hysterectomy, osteoporosis, arterial hypertension, and small intestine neuroendocrine tumor with segmental resection and termino-terminal anastomosis. Bilateral lower extremity edema and a grade 4/6 systolic tricuspid murmur were observed in the clinical examination. Home medication included Sulfasalazine 2000 mg per day, Lanreotide 60 mg monthly, Vitamin D 2000 UI daily, Bisoprolol 5 mg daily, and Ramipril 5mg daily.
Upon admission, the blood results showed cholestasis syndrome (GGT = 87 U/L, total bilirubin = 2.15 mg/dL, direct bilirubin = 0.72 mg/dL, indirect bilirubin = 1.43 mg/dL) and a moderate elevation of N-terminal pro-brain-type natriuretic peptide (NT-proBNP) (1,577 pg/mL). The other laboratory parameters did not show any abnormalities.
The electrocardiogram (ECG) revealed sinus rhythm with a heart rate of 80 b.p.m. and minor right bundle branch block (RBBB) (Figure 1-A). Chest X-ray showed slight heart dilatation (cardiothoracic index=0.53) (Figure 1-B).
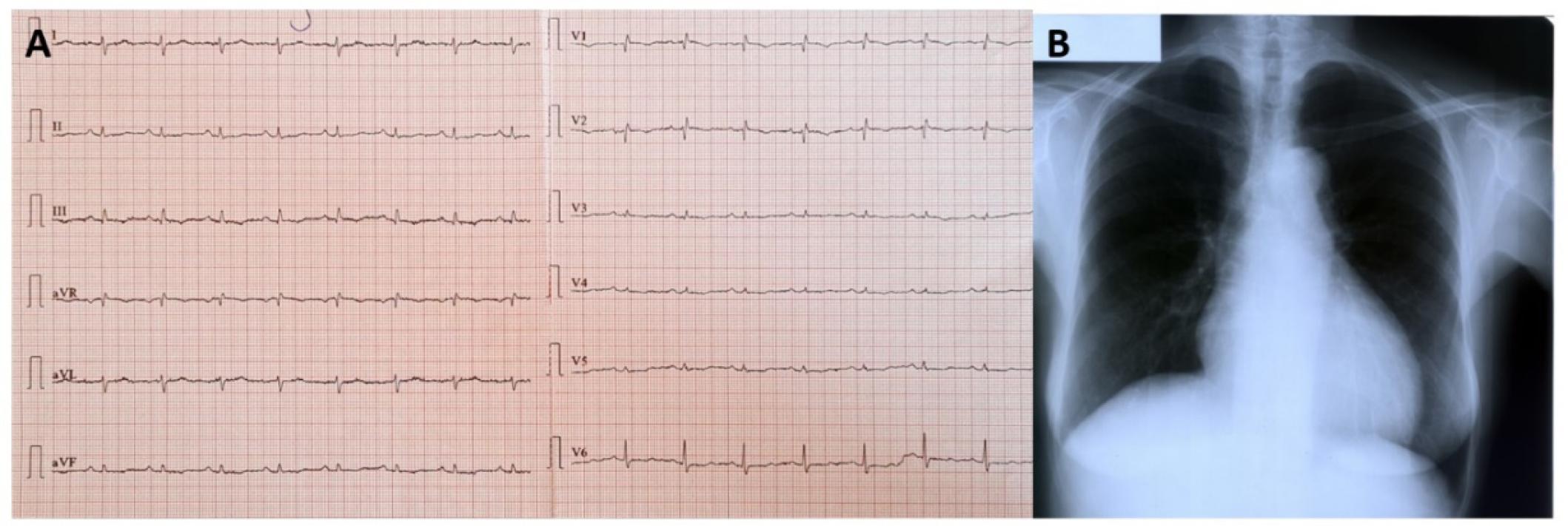
A.ECG: Sinus rhythm, 80/min, minor RBBB. B.Chest X-ray: cardiothoracic index=0,53.
Transthoracic echocardiography (TTE) remains the cornerstone for diagnosing carcinoid heart disease. In this case, we observed the characteristic thickening of the valve leaflets and the subvalvular apparatus, which are typical signs of the disease. Transthoracic echocardiography revealed normal ventricular dimensions and wall thickness, no wall motion abnormalities, preserved global systolic function, and normofunctional aortic and mitral valves (Figure 2-A, B). Also, an enlarged right ventricle (RVOT proximal diameter = 44 mm, RVOT distal diameter = 27 mm) (Figure 2-C, D) was observed, with important medioventricular trabeculation (Figure 2-E) and enlarged right atrium (RA volume = 121 mL) (Figure 2-F). The right ventricular systolic function was normal (RVFAC-right ventricle fractional area change = 46%, TAPSE-tricuspid annular plane systolic excursion = 22 mm, S’t = 16 cm/s, and right ventricular free wall longitudinal strain-RVFWLS = -19.5%) (Figure 3).
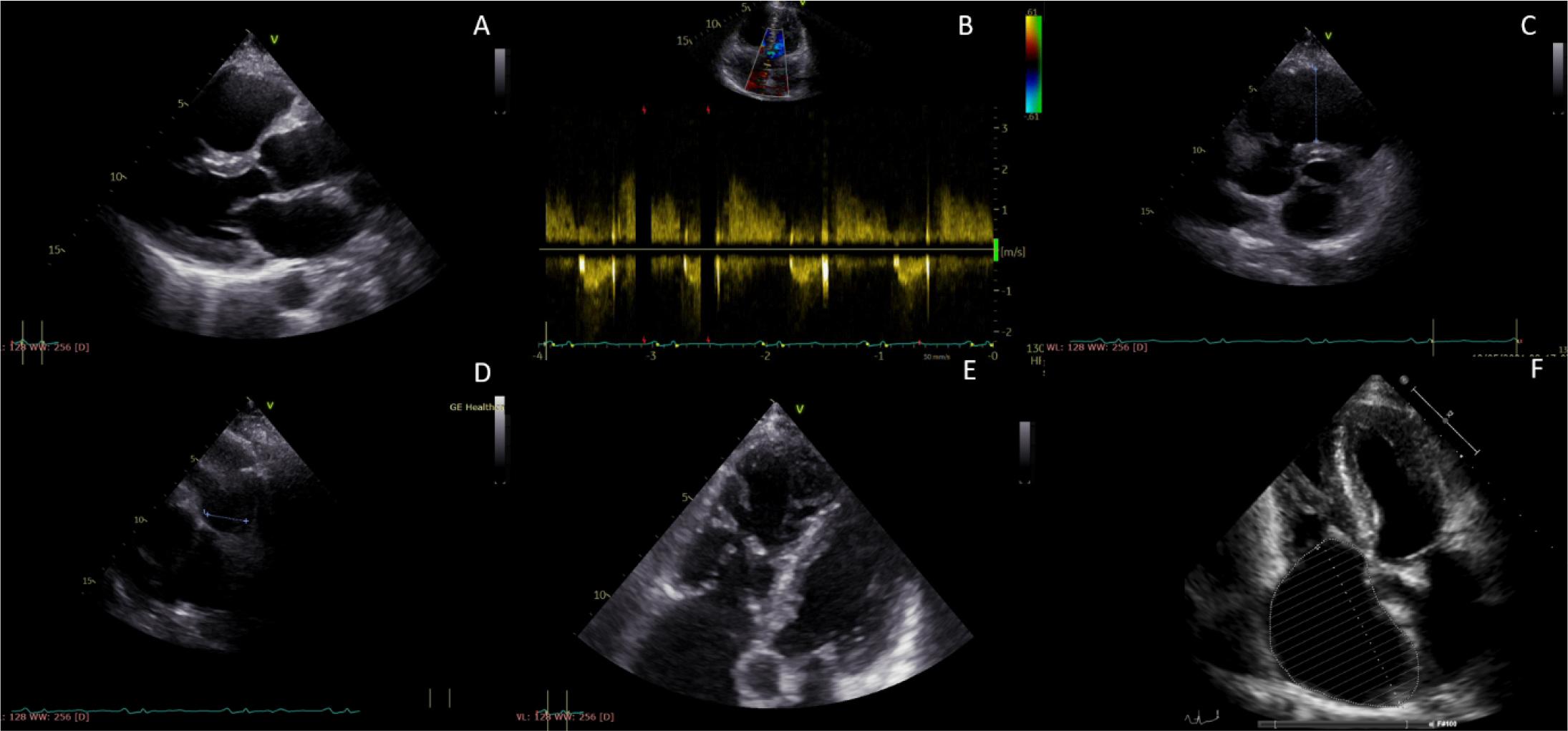
Transthoracic echocardiography. A. Left ventricle-normal dimension and wall thickness. B. Normofunctional aortic valve. C, D, F. Enlarged right cavities. E.Medioventricular trabeculation.
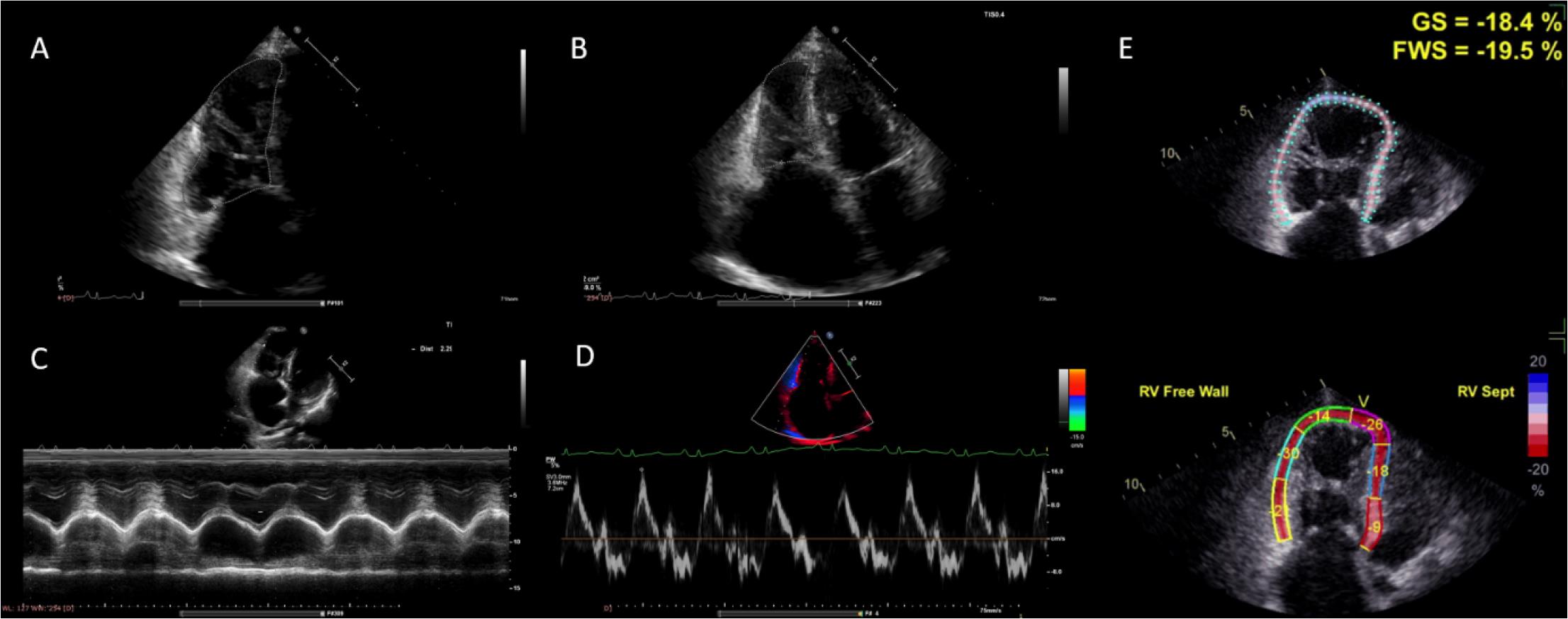
Normal right ventricular systolic function. A, B. RVFAC=46%. C. TAPSE=22 mm. D. S’t=16 cm/s. E. RVFWLS= -19,5%.
The tricuspid valve leaflets were thickened with fused shortened chordae, causing severe tricuspid regurgitation (continuous wave (CW) signal jet-dense, triangular, with early peaking contour, systolic reflux in hepatic veins) and stenosis (diastolic mean gradient = 12 mmHg). The pulmonary valve cusps were thickened, causing severe pulmonary regurgitation and moderate pulmonary stenosis with a peak pressure gradient of 38 mmHg (Figure 4).
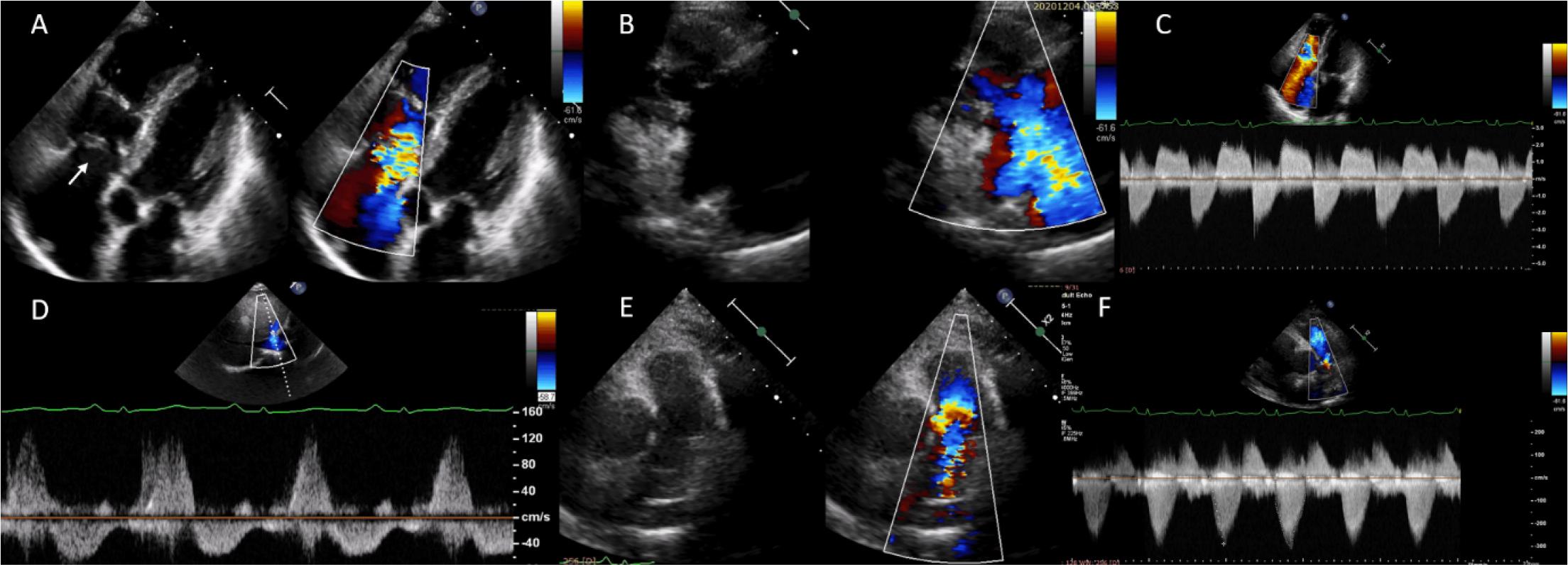
A. Thickened tricuspid valve leaflets. B. Severe tricuspid regurgitation. C. CW signal jet-dense, triangular, with early peaking contour. D. Systolic reflux in hepatic veins. E. Thickened pulmonary valve cusps, pulmonary stenosis, turbulent diastolic flow. F. Moderate pulmonary valve stenosis with a peak pressure gradient of 38 mmHg.
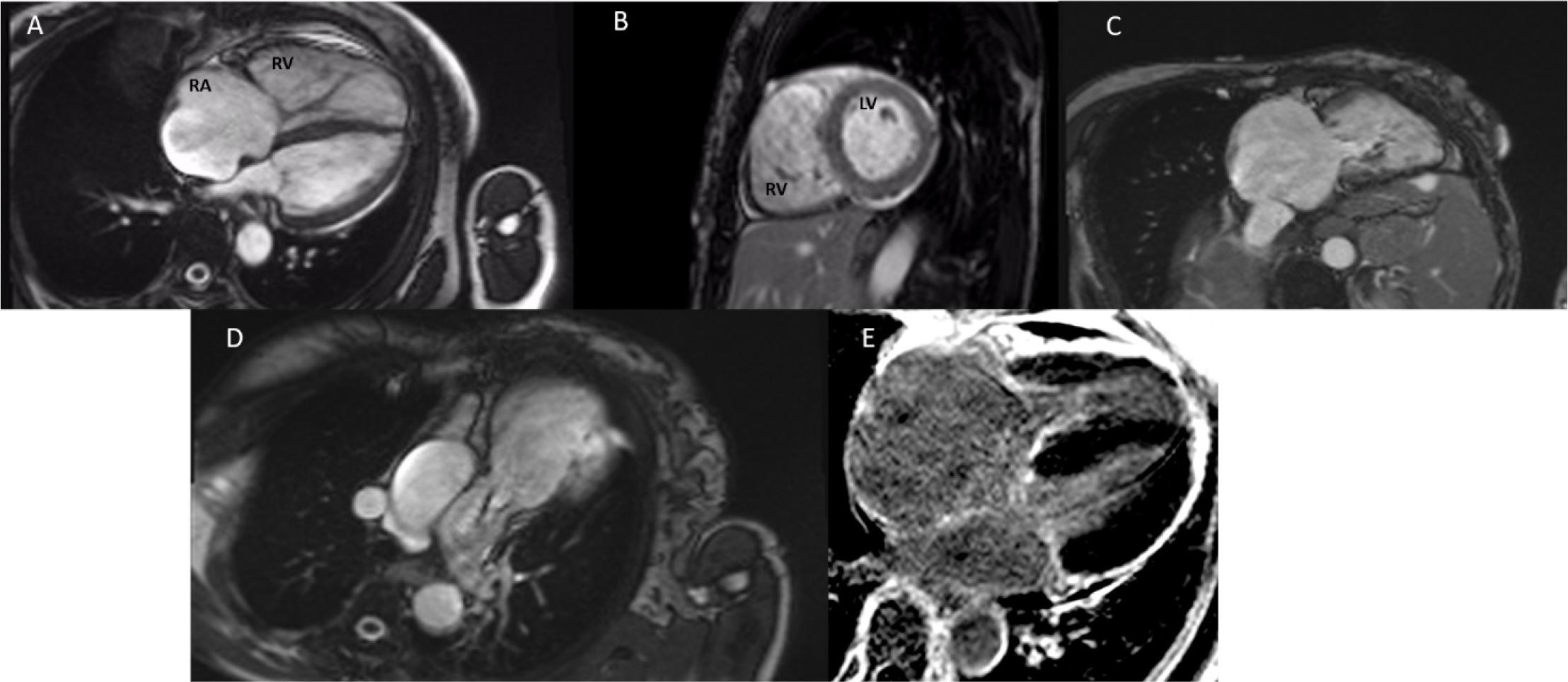
A, B, C. Enlarged right cavities, thickened tricuspid valve leaflets. D. Pulmonary regurgitation. E. No cardiac metastases.
Regarding the etiology of right heart failure, the following diagnoses were taken into consideration: pulmonary embolism, rheumatic heart disease, Ebstein disease, infective endocarditis, and right ventricular arrhythmogenic dysplasia.
Pulmonary angiography results of our patient with a negative D-dimer test and low Geneva score excluded pulmonary embolism. Right heart catheterization (RHC) was not performed in this patient, as severe tricuspid regurgitation was sufficiently confirmed by transthoracic echocardiography and cardiac magnetic resonance imaging. However, we recognize the value of RHC in differentiating between torrential and severe TR, particularly in complex cases where echocardiographic assessment may be inconclusive. The patient has no history of untreated strep throat or rheumatic fever, and the aortic and mitral valves are normofunctional. Some congenital heart defects may affect the tricuspid valve. We have considered Ebstein’s anomaly, but the tricuspid valve leaflets sit normally. The tricuspid valve may be damaged by an infection of the lining of the heart that can involve heart valves. Duke criteria were not met. Also, the Padua criteria for diagnosis of arrhythmogenic cardiomyopathy were not met8,9.
The small intestine tumor was removed, but unusually increased levels of circulating serotonin (>1,000 mg/L), urinary 5-HIAA-hydroxyindoleacetic acid (97.9 mg/24 hours), and Chromogranin A (5,390 μg/L) were observed. Abdominal computed tomography revealed hepatic metastases confirmed by biopsy and anatomopathological examination.
Cardiac magnetic resonance showed severe right atrium and right ventricle regurgitation with preserved right ventricular systolic function (RVEF = 71%), thickened and fixed tricuspid valve leaflets with severe tricuspid regurgitation, thickened pulmonary cusps with moderate stenosis and severe pulmonary regurgitation, but no cardiac metastases (Figure 4).
The patient was medicated with furosemide (40 mg/day), spironolactone (25 mg/day), ramipril (5 mg/day), and bisoprolol (5 mg/zi), and she was discharged clinically improved. After talking with the endocrinologist, the dose of Lanreotide was doubled. The indication of surgery was discussed.
CaHD is caused by thousands of vasoactive substances secreted by metastatic tumor cells in the liver, leading to white plaque deposits on the endocardium3. In 90% of cases, deposits are found in the right heart1. The aortic and mitral valves are involved in patients with patent foramen ovale or when NET is localized in the lung1. The mitral and aortic valves were evaluated in our patient and were found to be normofunctional, as confirmed by transthoracic echocardiography. Although the tricuspid and pulmonary valves are the primary sites of involvement in carcinoid heart disease, we recognize that, in certain cases, especially those involving a patent foramen ovale or lung-located neuroendocrine tumors, the aortic and mitral valves may also be affected. Our patient’s interatrial septum was intact, and the left heart was not involved. While an agitated saline study was not performed in this case, as there was no clinical indication or evidence of a patent foramen ovale or atrial septal defect based on the patient’s clinical history and transthoracic echocardiographic findings, we acknowledge that such a study may be considered in patients with a suspected right-to-left shunt.
Besides valvular involvement, specifically tricuspid valve regurgitation and pulmonary valve stenosis, other cardiovascular manifestations may be found: coronary artery involvement, arrhythmias, or direct myocardial involvment10. In our patient, transthoracic echocardiography and cardiac magnetic resonance found severe tricuspid regurgitation, moderate pulmonary stenosis, and severe pulmonary regurgitation. The pulmonic valve is a key structure in carcinoid heart disease, and its involvement is significant. In our patient, the thickening of the pulmonary valve cusps led to severe pulmonary regurgitation and moderate pulmonary stenosis. This highlights the importance of a thorough evaluation of the pulmonic valve in diagnosing and managing CaHD. One hallmark feature of carcinoid valve disease is the ‘board-like’ motion of the valve leaflets, a stiffened, restricted movement that contrasts with the normal undulating motion of healthy valves. In our case, this feature was evident in both the tricuspid and pulmonary valves, contributing significantly to the diagnosis. Coronary heart disease was excluded using computed tomography angiography. On Holter monitoring, there was no evidence of arrhythmias. CMR evaluated direct myocardial involvement. Cardiac MRI is particularly useful in cases where echocardiographic views are limited or when there is a need to assess complex right-sided valve pathologies or possible cardiac metastases. In our patient, MRI confirmed the presence of severe tricuspid and pulmonary regurgitation, as well as the absence of cardiac metastases.
The diagnosis of CaHD depends upon clinical suspicion, biomarker levels, and cardiac imaging results2. In addition to transthoracic echocardiography and cardiac magnetic resonance imaging, biomarkers such as NT-proBNP, 5-HIAA, and chromogranin A play a crucial role in diagnosing, prognosis, and monitoring carcinoid heart disease. Elevated NT-proBNP levels are associated with the severity of right heart dysfunction, while 5-HIAA and chromogranin A are instrumental in assessing the extent of tumor activity and cardiac involvement. These biomarkers provide valuable information for both diagnosing and managing patients with CaHD10.
Transthoracic echocardiography is the gold standard in diagnosing and monitoring patients with CaHD. In patients with carcinoid heart disease, transthoracic echocardiography is recommended every three or six months or when the clinical status is changing1. Cardiac magnetic resonance imaging and cardiac computed tomography may assess the heart valves’ pathology, especially of the pulmonary valve, recognize cardiac metastases, and assess the right ventricle2.
In CaHD, cardiovascular surgery is an effective treatment option for patients with severe symptoms, fatigue, or dyspnea leading to edema, ascites, or progressive asymptomatic right ventricular dysfunction2. Current literature suggests that valve surgery may improve these patients’ survival and quality of life. In our case, the patient had normal right ventricular function, with poorly controlled systemic disease (biomarkers were still markedly increased) and an increased risk of bleeding because of high-volume liver metastases, so pharmacologic management with close imaging follow-up every three months was chosen. However, in patients with progressive right heart failure or poorly controlled tumor activity, surgical treatment of the affected valves may be warranted to improve clinical outcomes.
Carcinoid heart disease is often overlooked due to its rarity, but this case highlights its distinctive features, especially on echocardiography, which can aid in prompt diagnosis and treatment. Early recognition of these features allows cardiologists to initiate timely diagnosis and management of this potentially fatal condition, and we believe this case serves as a valuable educational opportunity to raise awareness among clinicians—particularly cardiologists—of this under-recognized disease.