Remote Ischemic Preconditioning (RIPC) is a noninvasive technique aimed at protecting the heart and other organs from the damaging effects of lethal ischemia and reperfusion injury. This approach consists of inducing short, intermittent periods of limb ischemia and reperfusion, usually achieved by repeatedly inflating and deflating a blood-pressure cuff on one or more limbs to a suprasystolic pressure level for several cycles.[1]
When organs are subjected to repeated short-term ischemia-reperfusion cycles, they experience less damage during the final reperfusion phase than during extended periods of ischemia. This effect is particularly evident in patients undergoing coronary artery bypass grafting (CABG) combined with remote ischemic conditioning (RIC).[2] [3]
This method was initially described by Murry et al. in 1986 during a study on canine hearts[4], which revealed the heart’s ability to adapt to ischemic episodes lasting several minutes — a phenomenon referred to as ischemic preconditioning (IP). [5] [6]
Przyklenk et al. first described the phenomenon of remote ischemic preconditioning (RIPC) in humans towards the end of the 20th century.[7] In the years that followed, the concept of “remote cardioprotection” through ischemic conditioning was extended to include other tissues and organs, as well as regions further from the heart.[8] The mechanisms involved are believed to include the release of transferable humoral factors from perfused tissue, along with neuronal responses.[9]
Despite the implementation of myocardial preservation strategies, coronary artery bypass grafting (CABG) remains associated with significant complications. During CABG, blood flow to the heart and lungs is temporarily halted, leading to oxygen deprivation in these organs. This disruption disturbs the balance between oxidant and antioxidant enzymes, resulting in inefficient degradation of free oxygen radicals; altered activity of antioxidant enzymes; and the accumulation of reactive oxygen species (ROS), which ultimately triggers oxidative stress.[10] [11] [12]
Antioxidants are molecules capable of preventing the oxidation of other substances by neutralizing oxidants or reducing the generation of free oxygen radicals. The primary antioxidant systems found in vascular walls include Superoxide Dismutase (SOD), Catalase, Glutathione Peroxidase, Thioredoxin, and Peroxiredoxin.[11,12]
The protective mechanisms of RIPC are thought to involve a complex interplay of humoral and neuronal signaling pathways, with cytokines such as interleukin-1 (IL-1) and interleukin-6 (IL-6) playing pivotal roles. IL-1 and IL-6 are key pro-inflammatory cytokines released during tissue ischemia and reperfusion, contributing to the inflammatory cascade that exacerbates ischemia-reperfusion injury. By modulating these cytokines and reducing systemic inflammation, RIPC has the potential to enhance outcomes in patients undergoing CABG.[13]
Remote ischemic preconditioning (RIPC) has been shown to reduce reperfusion injury in patients undergoing cardiac surgery and improve clinical outcomes.[14]
This study aims to evaluate the impact of remote ischemic preconditioning on inflammatory markers and oxidative stress in patients with severe coronary artery disease who are undergoing CABG.
We conducted a prospective observational study, enrolling 80 consecutive adult patients (aged over 18 years) with severe coronary artery disease who were scheduled for elective CABG and had provided consent for the procedure (Figure 1).
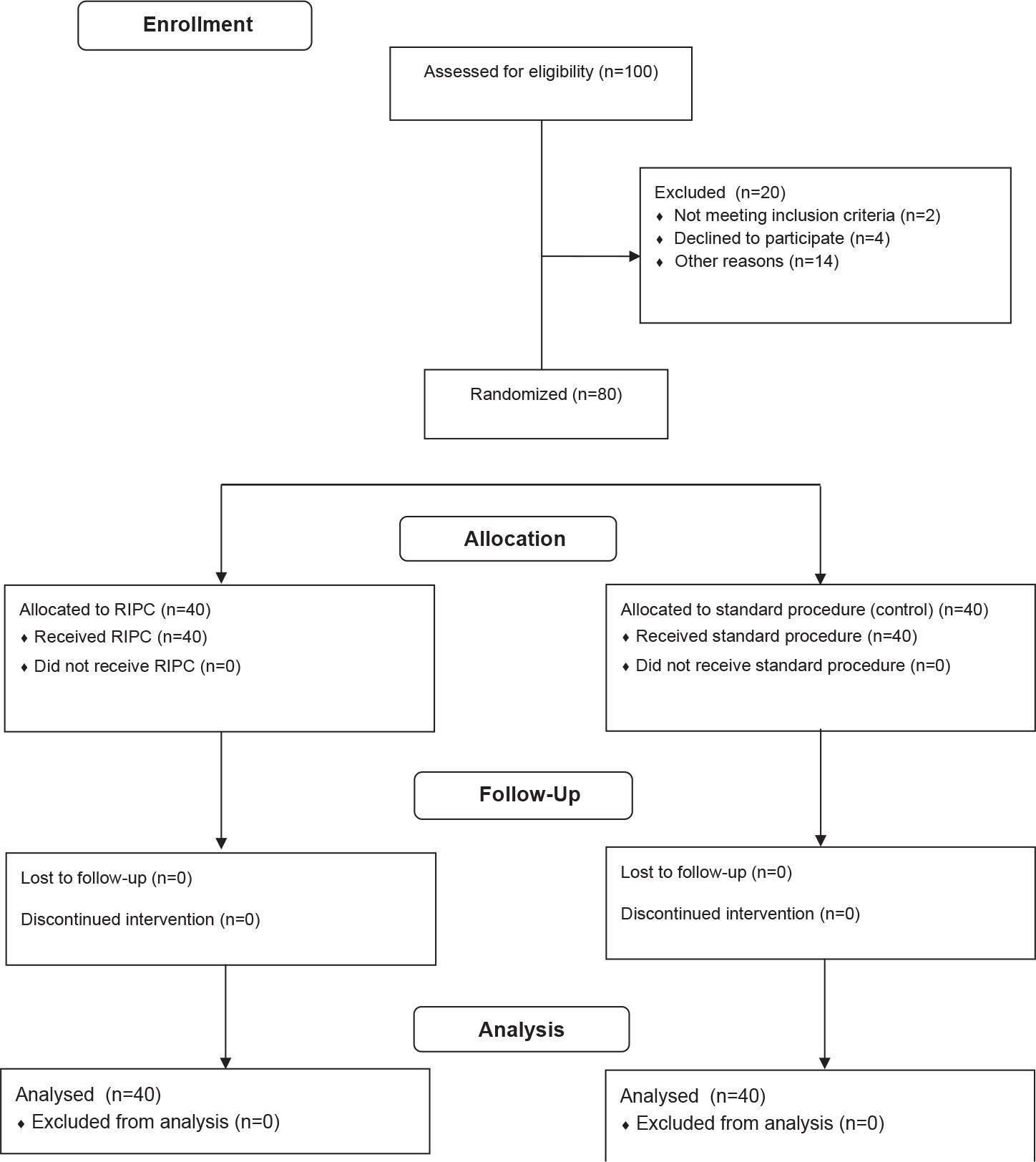
Randomization and follow-up flow chart
The inclusion criteria for this study required participants to weigh more than 50 kg, be over 18 years of age, and have provided appropriately dated and signed written informed consent prior to enrollment. Patients with a history of prior revascularization; decompensated heart failure; left ventricular ejection fraction (LVEF) below 30%; severe renal failure (grade 4 or requiring dialysis); hepatic dysfunction (Child-Pugh class B or higher); severe pulmonary disease; an indication for emergency CABG; and/or those unable or unwilling to provide informed consent were excluded from the study.
Following inclusion, patients were randomly assigned in a 1:1 ratio to either the RIPC group or the control group. All personnel involved in conducting the study were blinded to the RIPC procedure.
Between January 2020 and November 2022, the study was conducted at Clinicco Hospital in Brasov. All procedures in this study were carried out in compliance with the Helsinki Declaration for human-subject research, and the Ethics Review Board of Transilvania University of Brasov provided ethical permission.
Patients were evaluated upon admission, which included a review of their medical history and current clinical status, as well as assessments from physical examinations, echocardiography, and laboratory tests.
The severity of coronary lesions was assessed using the Syntax score, which was based on coronary angiography done in all patients roughly 2 to 4 weeks prior to the index CABG hospitalization.
Blood samples were obtained in accordance with hospital procedure and tested for blood cell counts; glycemia; renal function; hepatic function; cardiac biomarkers such as creatin-kinase MB (CK-MB); high-sensitivity troponin I (hsTnI); various inflammatory markers; and other biological parameters.
For the specific parameters in our investigation, we centrifuged the samples to separate the serum and plasma, which were subsequently labeled and stored at -80° C. We used the ELISA test to measure SOD-1, IL-1, and IL-6 levels in both preconditioned and non-preconditioned populations at three critical points: before surgery (visit 1, or V1), immediately post-operation (visit 2, or V2), and one week post-operation (visit 3, or V3).
RIPC was performed on the day of surgery, prior to the administration of anesthesia. It involved inflating a blood-pressure cuff on the upper and lower limbs to 200 mmHg for 5 minutes (ischemia stage), followed by a period of five minutes with the cuff deflated (reperfusion stage), for a total of four cycles.
Anesthesia, cardiopulmonary bypass, cardioplegia, surgical methods, and all other parts of pre- and postoperative care all followed the hospital’s established standards. All patients were given the same form of general anesthesia, which included volatile inhalation and intravenous hypnotics.
The database was developed using Microsoft Excel 2019, and the data were analyzed with JASP version 0.19.0. Categorical variables were reported as counts or absolute frequencies. To compare the mean values of two variables, we employed either Student’s t-test or the Mann-Whitney U test, depending on the normality of the distribution. A p-value of less than 0.05 was considered statistically significant. Post-hoc analyses were conducted using repeated measures ANOVA to identify differences both within and between groups.
For the power analysis, we anticipated an effect size of Cohen’s d = 0.5, indicative of a medium effect, with a significance level (alpha) of 0.05 and a desired power of 0.80. This power level was chosen to ensure an 80% likelihood of detecting a true effect if one exists, thus effectively balancing the risks of Type I (false positive) and Type II (false negative) errors.
Out of the 100 patients screened, 80 were successfully enrolled in the study, as illustrated in Figure 1. The remaining 20 patients were excluded for the following reasons: two did not meet the inclusion criterion of weighing over 50 kg; four declined participation, refusing to sign the informed consent form; and 14 were excluded for reasons detailed in the CONSORT flow chart. Specifically, two patients had severe renal impairment, two had a history of prior revascularization, four were diagnosed with decompensated heart failure, and six faced logistical challenges, such as transportation difficulties or residing at a considerable distance from the study site.
Of the 80 patients who were enrolled, 40 were randomly assigned to receive RIPC and 40 were assigned to the control group. No patients were lost to follow-up or excluded early from the trial.
The baseline characteristics of the patients in both the experimental and control groups were usually well-matched, with no statistically significant differences found, as shown in Table 1. The experimental and control groups had comparable mean ages (65.00 ± 7.57 years and 64.47 ± 8.53 years, respectively, p = 0.90). The gender distribution also differed slightly, with the experimental group having a greater proportion of males (85%) than the control group (75%); however, the difference was not statistically significant. The mean body mass index (BMI) and smoking status were also comparable between the groups.
Baseline characteristics of the patients
| Experimental group N = 40 | Control group N = 40 | p | |
|---|---|---|---|
| Age – years (mean) ± SD | 65 ± 7.57 | 64.47 ± 8.53 | 0.90 |
| Gender (male) – n, (%) | 34, (85) | 29, (72.50) | 0.08 |
| BMI – kg/m2±SD | 27.88 ± 4.26 | 29.36 ± 3.93 | 0.98 |
| Smoking – n, (%) | 9, (22.50) | 6, (15) | 0.08 |
The risk factors were generally similar between the experimental and control groups, as shown in Table 2. Dyslipidemia was present in all patients in the experimental group (100%) and 92.5% in the control group (p = 0.10). Both groups had high prevalence rates of arterial hypertension (HTN), with 97.5% in the experimental group and 92.5% in the control group (p = 0.21). Type 2 diabetes mellitus (T2DM) was detected in 40% of the experimental group and 37.5% of the control group (p = 0.36). A history of myocardial infarction (MI) was reported in 30% of the experimental group and 42.5% of the control group (p = 0.11), while stroke was reported equally in both groups at 5% (p = 0.98). Peripheral arterial disease (PAD) was slightly more common in the control group (15%) than in the experimental group (7.5%), though the difference was not statistically significant (p = 0.10).
Cardiovascular risk factors of the patients
| Experimental group N = 40 | Control group N = 40 | p | |
|---|---|---|---|
| Dyslipidemia n, (%) | 40, (100.00) | 37, (92.50) | 0.10 |
| HTN n, (%) | 39, (97.50) | 37, (92.50) | 0.21 |
| T2DM n, (%) | 16, (40.00) | 15, (37.50) | 0.36 |
| Old MI n, (%) | 12, (30.00) | 17, (42.50) | 0.11 |
| History of stroke n, (%) | 2, (5.00) | 2, (5.00) | 0.98 |
| PAD n, (%) | 4, (7.50) | 8, (15) | 0.10 |
HTN - arterial hypertension; T2DM - type 2 diabetes mellitus; MI - myocardial infarction; PAD - peripheral artery disease
Overall, the patients’ baseline characteristics and the presence of cardiovascular risk factors were well-balanced between the two groups, indicating that differences in these variables did not influence the study’s outcomes.
The operative features of the patients showed no significant variations between the experimental and control groups, implying similar surgical experiences and outcomes across both cohorts, which were unaffected by RIPC, as shown in Table 3. The SYNTAX I score, which measures the complexity of coronary artery disease, was similar in the experimental and control groups (29.58 ± 7.94 and 30.51 ± 8.59, respectively, p = 0.61). The experimental group had a similar aortic clamp time (ACT) of 65.45 ± 28.20 minutes, compared to the control group’s 76.42 ± 26.33 minutes (p = 0.97), and a CPBT of 81.20 ± 28.00 minutes, versus the control group’s 93.50 ± 28.31 minutes (p = 0.97).
Operative characteristics of the patients
| Experimental group N = 40 | Control group N = 40 | p | |
|---|---|---|---|
| SYNTAX I – n ± SD | 29.58 ± 7.94 | 30.51 ± 8.59 | 0.61 |
| ACT (min) – n ± SD | 65.45 ± 28.20 | 76.42 ± 26.33 | 0.97 |
| CPBT (min) – n ± SD | 81.20 ± 28 | 93.50 ± 28.31 | 0.97 |
| LVEF/pre (%) – n ± SD | 51.75 ± 7.97 | 48.37 ± 9.63 | 0.89 |
| LVEF/post (%) – n ± SD | 51.62 ± 7.37 | 49.37 ± 8.02 | 0.90 |
| ICU days (n) – n ± SD | 3.62 ± 0.86 | 4.10±1.59 | 0.97 |
| Hosp. days (n) - n ± SD | 10.30 ± 2.51 | 10.55 ± 3.17 | 0.98 |
ACT - aortic clamp time; CPBT - cardio-pulmonary bypass time; LVEF/pre - left ventricular ejection fraction preoperatory; LVEF/post - left ventricular ejection fraction postoperatory; ICU - intensive care unit
The experimental group had a slightly greater preoperative left ventricular ejection fraction (LVEF) (51.75 ± 7.97%) than the control group (48.37 ± 9.63%, p = 0.89), although postoperative LVEF values were comparable (51.62 ± 7.37% vs. 49.37 ± 8.02%, p = 0.90). The number of days spent in the intensive care unit (ICU) and total hospital stay were closely matched, with ICU stays averaging 3.62 ± 0.86 days in the experimental group and 4.10 ± 1.59 days in the control group (p = 0.97). Total hospital stays were 10.30 ± 2.51 days and 10.55 ± 3.17 days, respectively (p = 0.98).
The general laboratory tests revealed no statistically significant differences between the experimental and control groups across all the measured parameters, as demonstrated in Table 4 and Figure 2.
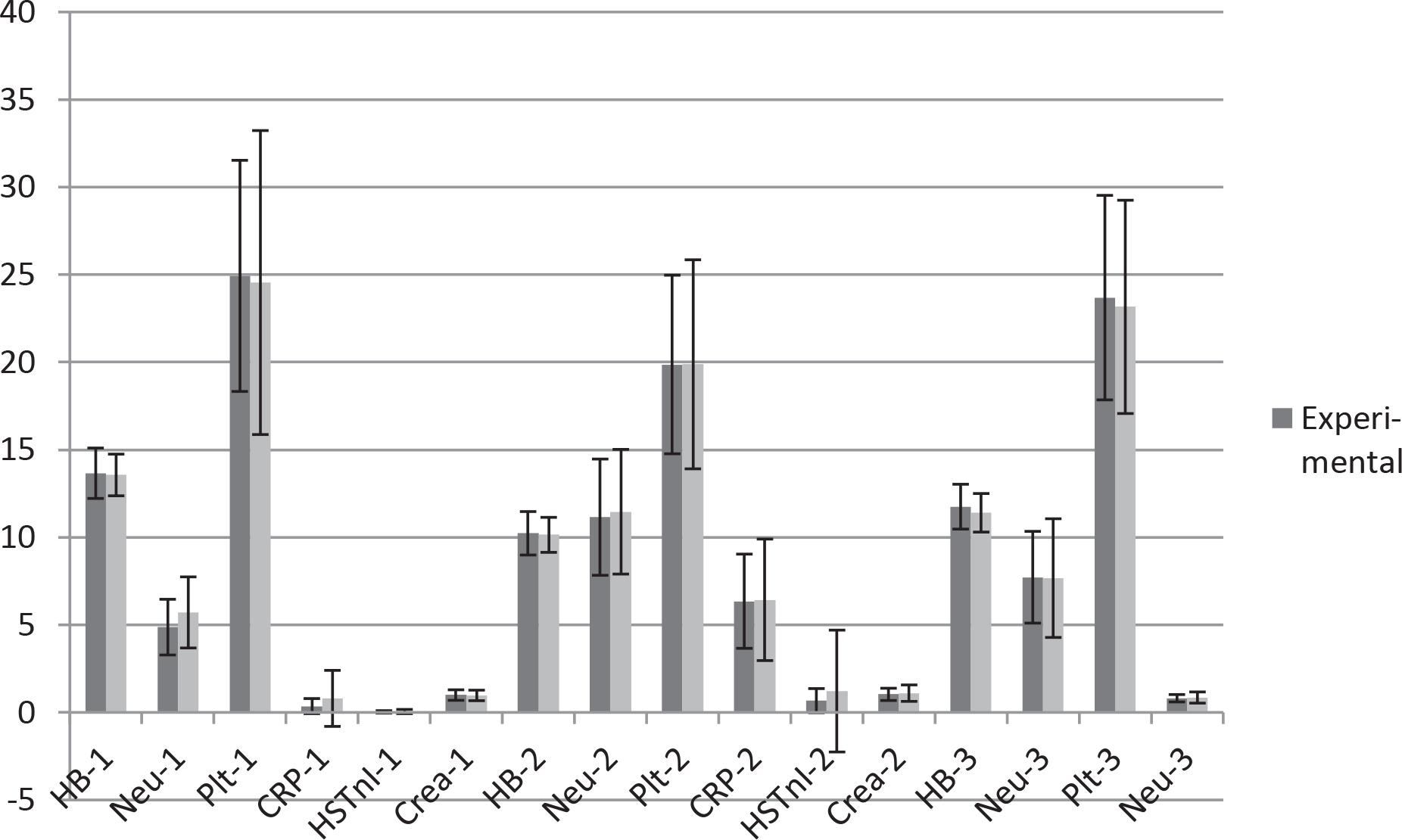
Descriptive box plots regarding general laboratory test activity.
General laboratory tests
| Experimental group N = 40 | Control group N = 40 | p | ||
|---|---|---|---|---|
| V1 | Hb - g/dl ± SD | 13.66 ± 1.44 | 13.56 ± 1.19 | 0.73 |
| Neu – u/l (103) ± SD | 4.87 ± 1.59 | 5.71 ± 2.03 | 0.44 | |
| Plt – u/l (103) ± SD | 249.35 ± 66.05 | 245.57 ± 86.80 | 0.82 | |
| CRP – mg/dl ± SD | 0.36 ± 0.43 | 0.80 ± 1.60 | 0.10 | |
| hsTnI – pg/ml ± SD | 0.03 ± 0.07 | 0.05 ± 0.12 | 0.57 | |
| Creatinine – mg/dl ± SD | 0.99 ± 0.30 | 0.97 ± 0.30 | 0.83 | |
| V2 | Hb - g/dl ± SD | 10.23 ± 1.24 | 10.14 ± 1.00 | 0.71 |
| Neu – u/l (103) ± SD | 11.15 ± 3.32 | 11.46 ± 3.56 | 0.69 | |
| Plt – u/l (103) ± SD | 198.75 ± 51.08 | 198.85 ± 59.75 | 0.99 | |
| CRP – mg/dl ± SD | 6.35 ± 2.69 | 6.43 ± 3.47 | 0.90 | |
| hsTnI – pg/ml ± SD | 0.67 ± 0.69 | 1.22 ± 3.48 | 0,33 | |
| Creatinine – mg/m l± SD | 1.03 ± 0.35 | 1.10 ± 0.47 | 0.43 | |
| V3 | Hb - g/dl ± SD | 11.75 ± 1.28 | 11.40 ± 1.10 | 0.19 |
| Neu – u/l (103) ± SD | 7.72 ± 2.62 | 7.67 ± 3.39 | 0.94 | |
| Plt – u/l (103) ± SD | 236.95 ± 58.41 | 231.62 ± 60.97 | 0.69 | |
| Creatinine – mg/ml ± SD | 0.81 ± 0.21 | 0.85 ± 0.32 | 0.45 | |
Hb - hemoglobin; CRP - C reactive protein; hsTnI – high sensitive troponin I; Neu – neutrophils; Plt - platelets
Prior to surgery, the levels of hemoglobin were comparable between the experimental group (13.66 ± 1.44 g/dL) and the control group (13.56 ± 1.19 g/dL), with a p-value of 0.73, indicating no significant difference. Similarly, CRP levels were 0.36 ± 0.43 mg/dL in the experimental group compared to 0.80 ± 1.60 mg/dL in the control group (p = 0.10). HsTnI levels were 0.03 ± 0.07 pg/mL in the experimental group versus 0.05 ± 0.12 pg/mL in the control group (p = 0.57). Additionally, serum creatinine levels were also comparable between the groups (0.99 ± 0.30 mg/dL vs. 0.97 ± 0.30 mg/dL, p = 0.83). Neutrophil counts were 4.87 ± 1.59 (×103/uL) for the experimental group and 5.71 ± 2.03 (×103/uL) for the control group (p = 0.44). Platelet counts were 249.35 ± 66.05 (×103/uL) in the experimental group, compared to 245.57 ± 86.80 (×103/uL) in the control group (p = 0.82).
Following surgery, the trends in laboratory markers remained consistent. Hemoglobin levels were 10.23 ± 1.24 g/dL in the experimental group and 10.14 ± 1.00 g/dL in the control group (p = 0.71). CRP levels increased significantly postoperatively, with values of 6.35 ± 2.69 mg/dL for the experimental group and 6.43 ± 3.47 mg/dL for the control group (p = 0.90). HsTnI levels were 0.67 ± 0.69 pg/mL in the experimental group, versus 1.22 ± 3.48 pg/mL in the control group (p = 0.33). Serum creatinine levels were 1.03 ± 0.35 mg/dL for the experimental group and 1.10 ± 0.47 mg/dL for the control group (p = 0.43). Neutrophil counts increased to 11.15 ± 3.32 (×103/uL) in the experimental group and 11.46 ± 3.56 (×103/uL) in the control group (p = 0.69). Platelet counts were 198.75 ± 51.08 (×103/uL) for the experimental group and 198.85 ± 59.75 (×103/uL) for the control group (p = 0.99).
At the follow-up visit (Visit 3), laboratory outcomes for Hb and serum creatinine were assessed. The experimental group had an Hb level of 11.75 ± 1.28 g/dL, compared to 11.40 ± 1.10 g/dL in the control group (p = 0.19). Serum creatinine levels were 0.81 ± 0.21 mg/dL for the experimental group versus 0.85 ± 0.32 mg/dL for the control group (p = 0.45). Neutrophil counts were 7.72 ± 2.62 (×103/uL) in the experimental group and 7.67 ± 3.39 (×103/uL) in the control group (p = 0.94). Platelet counts were 236.95 ± 58.41 (×103/uL) for the experimental group and 231.62 ± 60.97 (×103/uL) for the control group (p = 0.69).
Notably, during the follow-up phase (Visit 3), only Hb, neutrophil, platelet and creatinine levels were evaluated, in compliance with the hospital’s laboratory testing standard. As a result, although the data offered insightful information about these particular parameters, our post-operative analysis is limited by the lack of further laboratory marker follow-up tests, such as CRP and hsTnI.
An extensive examination of pre-operative biochemical markers conducted at the beginning of the study revealed that plasma levels of SOD-1, IL-1, and IL-6 were comparable in the experimental and control groups prior to surgery. By creating a trustworthy baseline between the two cohorts, this consistency makes sure that any disparities in the results can be attributed to variations in key markers of inflammation and oxidative stress that may have preceded the interventions.
An ANOVA analysis of the results of repeated assessments of SOD-1, IL-1, and IL-6 levels in patients undergoing coronary artery bypass grafting (CABG) with remote ischemia preconditioning (RIPC) revealed significant differences between the experimental and control groups at various time points.
SOD-1 levels in the experimental group increased considerably from V1 (1.38 ± 0.20 pg/ml) to V2 (2.99 ± 0.93 pg/ml, p < 0.001) and decreased slightly by V3 (2.20 ± 1.22 pg/ml, p < 0.01), but remained elevated compared to the baseline. In contrast, the control group’s SOD-1 levels remained reasonably steady, with no significant changes between visits, as seen in Table 5 and Figure 3.
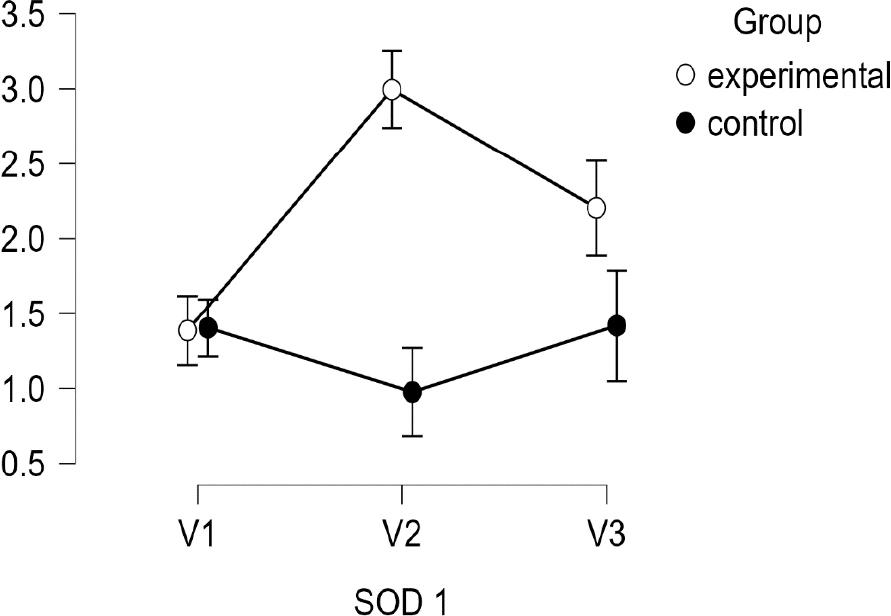
Descriptive plots regarding SOD-1.
Results of ANOVA RM for SOD-1, IL-1 and IL-6 under RIPC on patients undergoing CABG
| SOD-1 | IL-1 | IL-6 | ||||
|---|---|---|---|---|---|---|
| Experimental (n = 40) | Control (n = 40) | Experimental (n = 40) | Control (n = 40) | Experimental (n = 40) | Control (n = 40) | |
| V1 | 1.38±0.20 | 1.4±0.24 | 14.57±11.17 | 16.78 ± 13.17 | 80.59 ± 10.89 | 77.66 ± 9.43 |
| V2 | 2.99 ± 0.93*** | 0.97 ± 0.79 | 2.85 ± 2.24*** | 5.56 ± 4.90 | 16.43±9.73** | 22.83 ± 13.39 |
| V3 | 2.20 ± 1.22** | 1.41 ± 1.33 | 2.75 ± 2.06*** | 6.54 ± 5.10 | 2.75 ± 2.06*** | 6.54 ± 5.10 |
Note. Post hoc comparisons (Holm correction): between (experimental vs. control) * p < 0.05,
p < 0.01,
p < 0.001.
Note 2. SOD-1, IL-1 and IL-6 values measured in pg/ml.
The levels of IL-1 were measured at three time points in both the experimental and control groups, as summarized in Table 5 and Figure 4. At baseline, IL-1 levels were comparable between the groups, with the experimental group showing a mean of 14.57 ± 11.17 pg/ml and the control group, 16.78 ± 13.17 pg/ml. However, a significant reduction in IL-1 levels was observed in the experimental group over the course of the study. By the second time point, the experimental group’s IL-1 levels had decreased to 2.85 ± 2.24 pg/ml, compared to 5.56 ± 4.90 pg/ml in the control group, a difference that was statistically significant (p < 0.001). At the final time point, the experimental group had maintained lower IL-1 levels (2.75 ± 2.06 pg/ml), whereas the control group’s IL-1 levels higher in comparison, at 6.54 ± 5.10 pg/ml, further reinforcing the significant difference (p < 0.001) between the two groups.
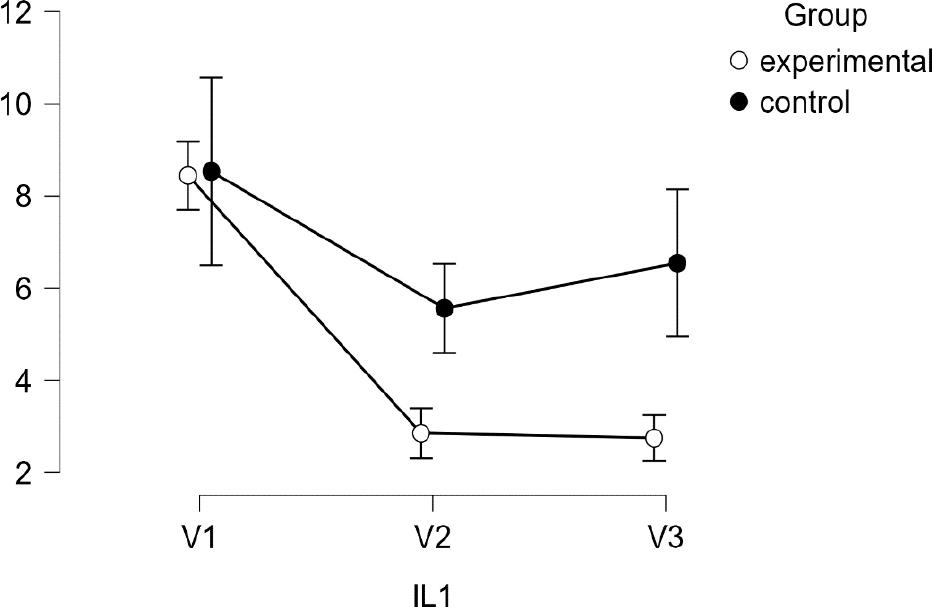
Descriptive plots regarding IL-1 activity.
Interleukin-6 (IL-6) levels were also measured at three time points in both the experimental (n = 40) and control (n = 40) groups. At baseline, IL-6 levels were comparable between the experimental group (80.59 ± 10.89 pg/ml) and the control group (77.66 ± 9.43 pg/ml), with no significant difference observed. Following the intervention, IL-6 levels significantly decreased in both groups. However, the experimental group showed a markedly greater reduction in IL-6 levels, which dropped to 16.43 ± 9.73 pg/ml, compared to 22.83 ± 13.39 pg/ml in the control group (p < 0.01).
By the final measurement, IL-6 levels in the experimental group had further decreased, to 2.75 ± 2.06 pg/ml – significantly lower than the control group, which recorded levels of 6.54 ± 5.10 pg/ml (p < 0.001), indicating a more pronounced anti-inflammatory effect in the experimental group, as demonstrated in Table 5 and Figure 5.
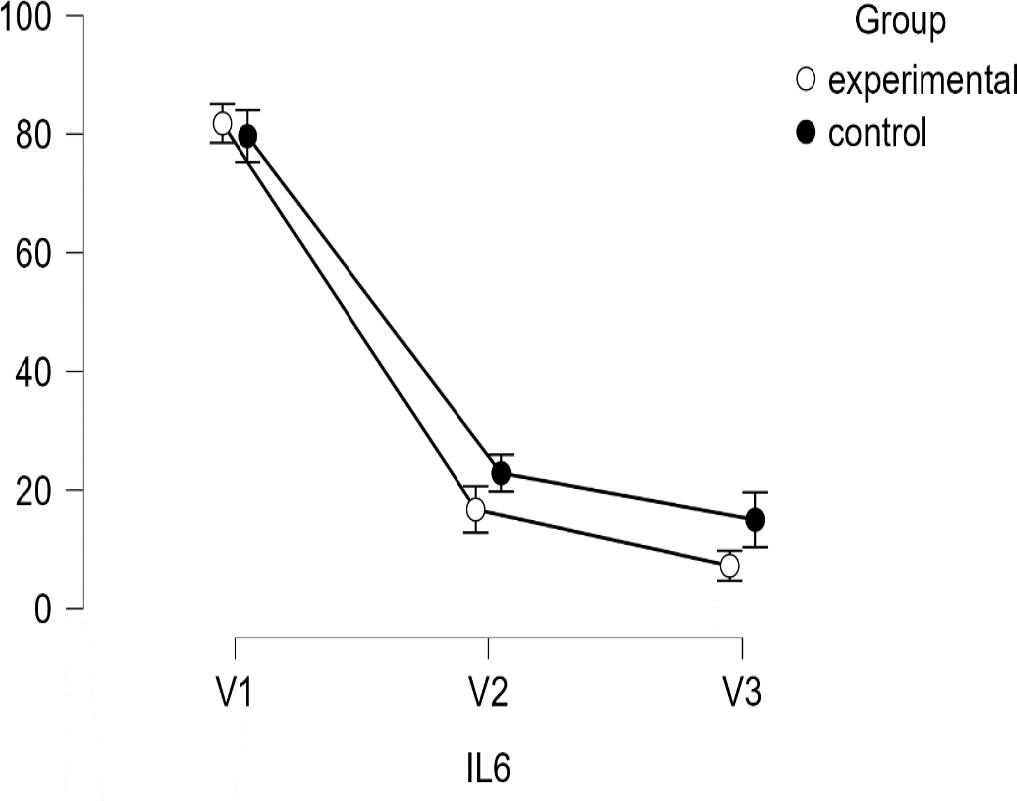
Descriptive plots regarding IL-6.
SOD-1, IL-1, and IL-6 levels were compared between the experimental (n = 40) and control (n = 40) groups at three time points. At baseline (V1), there were no significant differences between groups for SOD-1, IL-1, or IL-6.
By V2, the experimental group showed significant improvements: SOD-1 increased to 2.99 ± 0.93 pg/ml, compared to 0.97 ± 0.79 pg/ml in the control group (p < 0.001); IL-1 decreased to 2.85 ± 2.24 pg/ml vs. 5.56 ± 4.90 pg/ml (p < 0.001) in the control group; and IL-6 dropped to 16.43 ± 9.73 pg/ml vs. 22.83 ± 13.39 pg/ml (p < 0.01) in the control group.
At V3, these trends continued, with the experimental group maintaining higher SOD-1 (2.20 ± 1.22 pg/ml vs. 1.41 ± 1.33 pg/ml, p < 0.01 in the control), and lower IL-1 and IL-6 levels (both p < 0.001), suggesting a stronger anti-inflammatory and antioxidant response in the experimental group.
Our study’s findings indicate that RIPC may influence oxidative stress and inflammatory responses in a manner that varies between groups, potentially explaining the differences observed in biomarker levels over time. These results align with prior research on the protective effects of RIPC. Additionally, while certain cardiovascular risk factors were assessed, their impact was not found to be statistically significant, suggesting they did not contribute meaningfully to the observed outcomes.
Interleukin-1 (IL-1) is a pivotal mediator of the inflammatory response triggered by ischemic injury, playing a significant role in cardiovascular disease, particularly during coronary artery bypass grafting (CABG). Elevated IL-1 levels have been associated with poor outcomes in CABG patients, as IL-1 drives the production of additional pro-inflammatory cytokines and exacerbates tissue damage by recruiting immune cells to the injury site.[15] Consequently, terventions aimed at reducing IL-1 levels may enhance clinical outcomes by attenuating excessive inflammation and minimizing myocardial injury during surgery.
In our study, remote ischemic preconditioning (RIPC) significantly reduced IL-1 levels in the experimental group compared to the control group. IL-1 levels in the experimental group declined from 14.57 ± 11.17 pg/ml at baseline to 2.75 ± 2.06 pg/ml at the final measurement, while the control group exhibited higher IL-1 levels (6.54 ± 5.10 pg/ml) at the same time point. These results support the growing evidence that RIPC mitigates systemic inflammation by regulating cytokine expression.[16] Consistent with prior research, our findings demonstrate that RIPC reduces the release of pro-inflammatory cytokines like IL-1, thereby dampening inflammation and protecting cardiac tissue from ischemia-reperfusion injury.[17]
Elevated IL-1 levels are linked to poorer outcomes in ischemic heart disease, making the reduction observed in our experimental group particularly significant. This finding underscores the potential of RIPC to alleviate perioperative inflammation and enhance long-term cardiac function. Previous research has shown that patients with lower postoperative IL-1 levels experience reduced myocardial injury and faster recovery.[18] Our results build on this evidence, suggesting that the anti-inflammatory properties of RIPC, as demonstrated by the decreased IL-1 levels, may be instrumental in improving CABG outcomes.
Interleukin-6 (IL-6), a pro-inflammatory cytokine, is a key mediator in the body’s response to tissue injury, particularly in cardiovascular conditions such as coronary artery disease. Elevated IL-6 levels have been linked to poorer outcomes in patients undergoing coronary artery bypass grafting (CABG), as IL-6 contributes to heightened inflammation, myocardial injury, and adverse cardiac remodeling. [19] Our study demonstrated that remote ischemic preconditioning (RIPC) significantly lowered IL-6 levels in CABG patients, highlighting a potential mechanism by which RIPC exerts its cardioprotective effects through the modulation of inflammatory pathways.
The significant reduction in IL-6 levels in the experimental group compared to the control group (p < 0.001) supports the hypothesis that RIPC mitigates systemic inflammation by suppressing cytokine production. Previous research has emphasized the role of IL-6 in ischemia-reperfusion injury, where elevated IL-6 levels amplify myocardial damage and lead to poorer clinical outcomes.[20] Our results are consistent with other studies reporting decreased IL-6 levels following RIPC, reinforcing the anti-inflammatory advantages of this intervention.[21]
IL-6 is also linked to the onset of heart failure and adverse cardiovascular events following surgery.[22] By markedly reducing IL-6 levels, RIPC may help lower the risk of postoperative complications and enhance long-term outcomes for patients undergoing CABG. This decrease in IL-6 may also mitigate the systemic inflammatory response syndrome (SIRS) that is frequently observed after cardiopulmonary bypass, which is a recognized driver of postoperative morbidity.[23]
SOD-1 is an essential antioxidant enzyme that catalyzes the conversion of superoxide radicals into hydrogen peroxide, safeguarding cells from oxidative damage.[12] The upregulation of SOD-1 observed in our study aligns with the established mechanisms of RIPC, which is thought to strengthen the body’s endogenous antioxidant defense system.
Previous research has highlighted RIPC’s ability to elevate antioxidant enzyme levels, though specific investigations into SOD-1 have been relatively limited. Similar findings have been reported for other antioxidant enzymes; for example, studies by Heusch et al. and Shimizu et al. demonstrated increased antioxidant levels and reduced oxidative stress in RIPC-treated patients, indicating that RIPC broadly enhances the antioxidant defense system.[9] [24] The significant increase in SOD-1 levels observed in our study adds to this body of evidence, suggesting that RIPC specifically boosts the activity of this vital enzyme, potentially contributing to its cardioprotective effects during CABG.
Our study’s findings are consistent with prior research exploring the role of remote ischemic preconditioning (RIPC) in regulating oxidative stress and inflammatory markers, including SOD-1, IL-1, and IL-6. Numerous studies have highlighted the cardioprotective benefits of RIPC during coronary artery bypass grafting (CABG), demonstrating its ability to reduce inflammatory cytokines and enhance antioxidant defenses. Notably, RIPC has been shown to elevate SOD-1 levels, thereby mitigating oxidative damage associated with ischemia-reperfusion injury, a finding that aligns with our observation of increased SOD-1 levels in the experimental group following the intervention.[25]
Similarly, RIPC has been shown to reduce IL-1 and IL-6 levels, underlining its involvement in mitigating the systemic inflammatory response induced by heart surgery. Our findings, which showed considerably lower IL-1 and IL-6 levels in the experimental group, are consistent with previous observations that RIPC lowers pro-inflammatory cytokine production, hence minimizing myocardial damage and enhancing cardioprotection.[25]
These findings support the idea that RIPC provides cardioprotection through a multifaceted mechanism that includes both the suppression of harmful oxidative processes and the augmentation of protective antioxidant defenses. This dual regulation may be especially advantageous in the context of CABG, where oxidative stress and inflammation are widespread and lead to complications following surgery.
As demonstrated in this research, the methodologies used to evaluate IL-1, IL-6, and SOD-1 in RIPC investigations rely mostly on ELISA, which has a high sensitivity and specificity for detecting these biomarkers in biological fluids. Western blotting and activity assays are also valuable, particularly for tissue-specific studies and functional assessments.[26] The methodology employed depends on the study’s focus, such as measuring protein levels or analyzing enzyme activity.
The prevalence of dyslipidemia in the experimental group (100%) and the control group (92.5%) aligns with existing evidence highlighting the ubiquity of dyslipidemia in CABG patients.[27] Dyslipidemia has been recognized as a key modifiable risk factor contributing to atherosclerosis and cardiovascular disease (CVD). Hypertension (HTN) also exhibited high prevalence in both groups, with rates of 97.5% in the experimental group and 92.5% in the control group. These findings are consistent with prior studies reporting HTN to be a common comorbidity in CABG patients.[28]
Although RIPC did not demonstrate significant differences in dyslipidemia or HTN prevalence, previous studies have suggested that RIPC might confer endothelial protective effects by reducing oxidative stress and inflammation.[9] However, translating such biochemical benefits into measurable clinical changes in cardiovascular risk factors may require longer observation periods and larger sample sizes.
Type 2 diabetes mellitus (T2DM) was observed in 40% of the experimental group and 37.5% of the control group, paralleling findings of high diabetes prevalence in CABG populations.[29] T2DM is a critical determinant of CVD risk due to its contribution to microvascular and macrovascular complications, which may explain its prevalence in both groups.
Prior myocardial infarction (MI) was more frequent in the control group (42.5%) than in the experimental group (30%), though this difference was not statistically significant. Similarly, stroke and peripheral artery disease (PAD) showed comparable prevalence in both groups, with PAD observed in 7.5% of the experimental group and 15% of the control group. This trend is consistent with studies indicating a strong association between PAD, prior cardiovascular events, and CABG candidacy.[30]
While this study did not identify significant differences in cardiovascular risk factors between the groups, RIPC may influence systemic pathways involved in cardiovascular health. For instance, RIPC has been shown to improve myocardial ischemia tolerance and reduce reperfusion injury.[31] However, its impact on long-term cardiovascular risk factor modification remains inconclusive and warrants further investigation.
Our findings contribute to the growing body of evidence that RIPC might modulate oxidative stress and inflammatory pathways, potentially delivering cardioprotective benefits during surgical procedures like CABG. This has important clinical implications, suggesting that RIPC could be a viable therapy for improving outcomes in CABG patients by targeting specific molecular pathways involved in oxidative stress and inflammation. Future studies should attempt to replicate these findings in bigger, multi-center trials, as well as delve deeper into the molecular basis of RIPC’s effects on IL-1, IL-6, and SOD1. Furthermore, more study is needed to determine whether RIPC might be used as an adjuvant therapy to pharmaceutical interventions that target oxidative stress in CABG patients.
This study has several limitations that should be considered. First, the sample size was relatively small, which may limit the generalizability of the findings, as demonstrated in Table 6.
Post-hoc Power Analysis
| Power | Without RIPC | With RIPC | Cohen’s |δ| | α | |
|---|---|---|---|---|---|
| 0.598 | 40 | 40 | 0.500 | 0.050 | |
| Power by Effect Size | |||||
| True effect size | Power to detect | Description | |||
| 0 < |δ| ≤ 0.444 | ≤ 50% | Likely to miss | |||
| 0.444 < |δ| ≤ 0.634 | 50% – 80% | Good chance of missing | |||
| 0.634 < |δ| ≤ 0.816 | 80% – 95% | Probably will detect | |||
| |δ| ≥ 0.816 | ≥ 95% | Almost surely will detect | |||
Note: RIPC – remote ischemic preconditioning
The post-hoc power analysis outlined in Table 6 emphasizes a key limitation previously noted in this study. With a sample size of 40 participants per group, the statistical power achieved was 0.598, which is below the commonly-accepted threshold of 0.80. This indicates a moderate risk of committing a Type II error. The effect size analysis further highlights this issue, showing that the study was adequately powered (≥ 95%) only for detecting large effect sizes (|δ|≥ 0.816). For medium effect sizes (0.634 < |δ| ≤ 0.816), the power ranged between 80% and 95%, reflecting a reasonable probability of identifying differences, albeit with some risk of underestimation. However, for small effect sizes (|δ| ≤ 0.634), the power declined sharply, indicating a considerable likelihood of failing to detect significant effects. This limitation suggests that the study, at this size, may lack sufficient sensitivity to identify smaller, yet potentially clinically meaningful, differences between groups.
Moreover, the study was conducted at a single center, which may have introduced selection bias. The limited duration of the follow-up period precluded the evaluation of the long-term effects of remote ischemic preconditioning (RIPC) on IL-1, IL-6, and SOD-1 levels following coronary artery bypass grafting (CABG). Additionally, although significant changes in these biomarkers were observed, the precise mechanisms by which RIPC modulates IL-1, IL-6, and SOD-1 remain insufficiently understood, necessitating further investigation.
This study shows that remote ischemic preconditioning (RIPC) can reduce oxidative stress and inflammation in patients undergoing CABG by significantly lowering IL-1 and IL-6 levels while increasing SOD-1 levels. These changes suggest that RIPC helps improve the body’s antioxidative defenses and reduces inflammatory processes linked to cardiovascular risk factors. As a result, RIPC may be an effective strategy for enhancing cardioprotection and improving outcomes in these patients.