
A recommendation system utilizes patient profiles and analyzed data to generate tailored recommendations. Recommendations such as changes in lifestyle that can improve sleep quality, such as better hygiene practices, managing stress, eating healthily, exercising regularly, and avoiding certain substances (such as alcohol or tobacco) are sometimes recommended.
The system can provide sleep exercises recommendations to improve one’s sleep environment, set a sleep schedule, train relaxation techniques, and other strategies to improve sleep. Recommendation systems can encourage consistent use of prescribed treatments and interventions by monitoring patient compliance and providing reminders and feedback. Feedback and interaction between system and patients can The recommender system continuously learns from new data and patient feedback, refining its algorithms and recommendations to adapt to individual patient needs and preferences. This iterative process ensures that the system remains up-to-date and relevant.
Another popular way to deal with sleep apnea (SA) is to diagnose this disease at an early stage with machine-learning (ML) and deep-learning (DL) methods. Signals recorded from suspected patients’ body like electrocardiogram (ECG), SpO2, and EEG are analyzed through these techniques to make predictions about the severity of the disease. Figure 1 shows a detailed workflow for SA diagnosis at sleep centers.
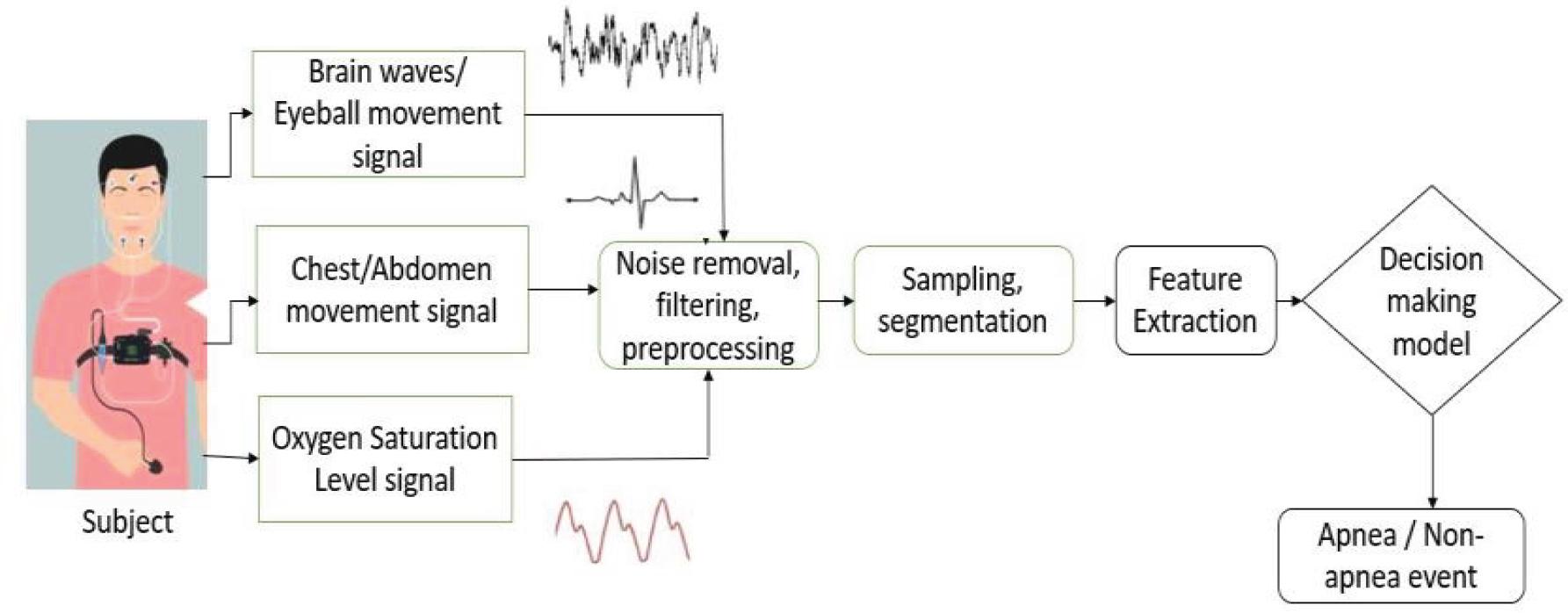
Workflow of sleep apnea diagnosis process
This review article discusses various approaches to diagnose sleep apnea and their advantages and drawbacks. This article also compares the effectiveness of ML or DL algorithms in terms of accuracy, precision, and recall. At the end, we propose a recommender system for SA patients.
We have explored databases such as PubMed and IEEE-Xplore to find the interaction between the health and biological sciences literature with the computer science and engineering literature. Google Scholar and NCBI were also used to manually screen papers from various journals and conferences based on title and abstract; see Table 1. In this review article, we have included/excluded articles based on some criteria; those are shown in Table 2.
Database search and selection criteria
| Electronic database |
|
| Inclusion criteria |
|
| Exclusion criteria |
|
Search strategy
| Population | Studies using physiological data to build sleep apnea classi^ication algorithms |
| Comparison | Different models and their utility for clinical intervention |
| Outcome | Ability to detect or predict sleep apnea, sleep arousals, respiratory events during sleep |
| Study type | Quantitative study |
| Keywords | Sleep apnea, recommender system, polysomnography, machine learning, artificial intelligence |
The available literature suggests that the occurrence of SA and factors that contribute to obstructive sleep apnea (OSA) in India are increasing urbanization, a stressful life, and lifestyle changes. India is expected to face an obesity epidemic, which is highly associated with OSA [1]. OSA is the most common breathing disorder worldwide. While obesity remains a major cause of OSA in Asians, factors like age, body mass index (BMI), smoking, and alcohol consumption may contribute more to OSA development; see Figure 1 for types, causes, and consequences of SA. Research highlights the need for public awareness, early diagnosis, and effective treatment to tackle SA [2].
The following research articles show that SA is highly prevalent in India and in other parts of the world. The data set “Sleep-Cohort-Study by Wisconsin” discusses the occurrence of sleep-disordered breathing (SDB) for two distinct time frames in the US: 1988–1994 and 2007–2010. The findings reveal a significant increase in the prevalence of moderateto-severe SA over the past two decades. The relative increases in various subgroups (by age) range from 14 percent to 55 percent [3]. A decade ago, Suri pioneered work on sleep medicine in India, which led to the establishment of multiple sleep centers across the country. The article underscores the need for educational initiatives, local production of affordable sleep analysis tools, and integrating sleep medicine into medical education. The article advocates collaborations with premier engineering institutes like IITMadras for developing cost-effective equipment’s for SA diagnosis [4].
Types of SA: The existing literature suggests three categories of SA: OSA, central sleep apnea (CSA), and mixed/complex sleep apnea; see Figure 2 for more details. Of these, OSA) is most prevalent. Individuals with OSA commonly experience repeated instances of pharyngeal airway narrowing or collapse during sleep, as highlighted by Campana et al. [5].
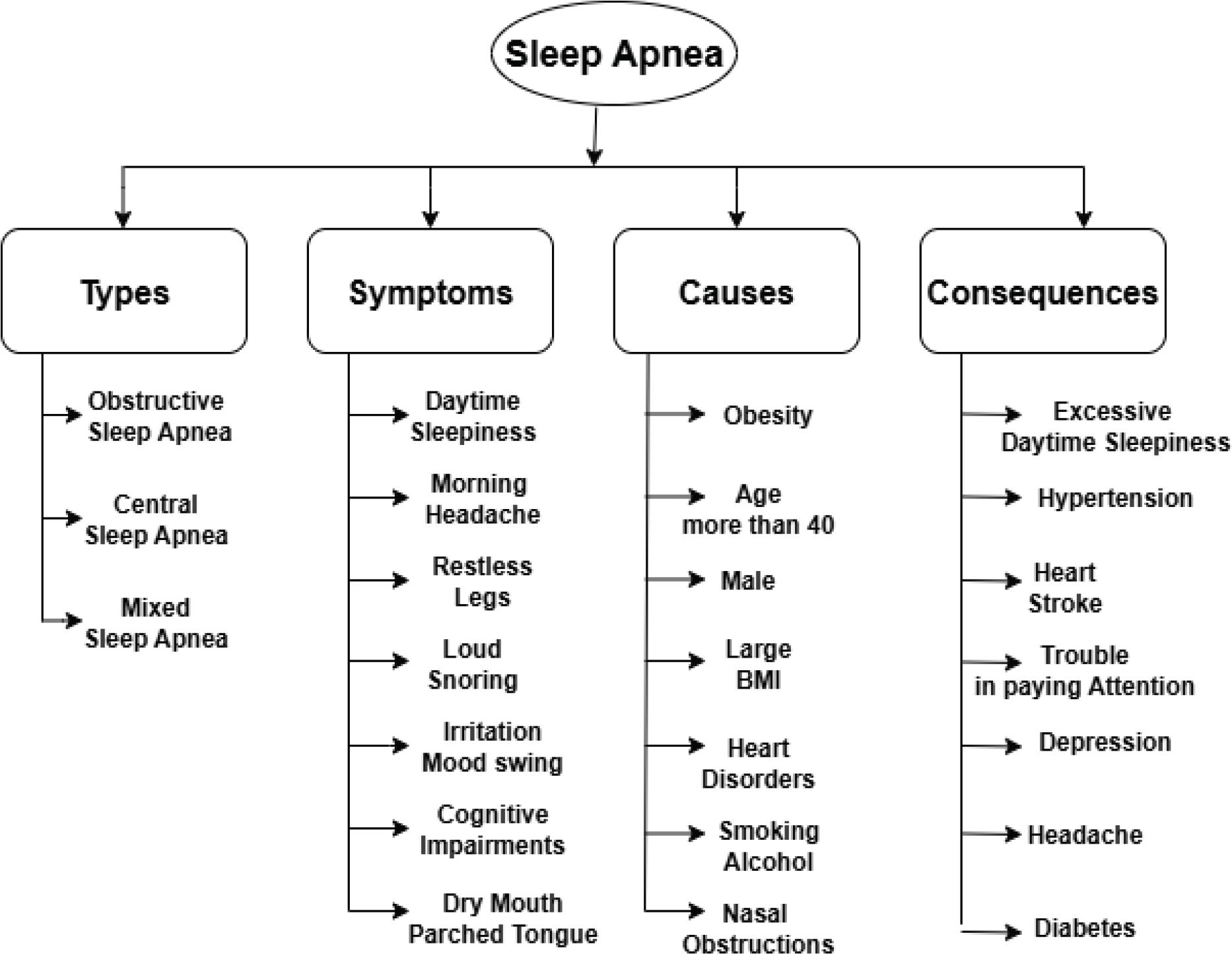
SA symptoms, causes, and consequences
OSA is characterized by repeated collapse of the upper airway during sleep, leading to disrupted sleep, hypoxemia, and increased risk of conditions like hypertension and cardiovascular disease (CVD). Figure 3 shows a comparison between various breathing patterns associated with breathing disorders. With a global prevalence of 2 percent to 10 percent, risk factors include age, gender, obesity, genetics, craniofacial anomalies, smoking, and alcohol consumption. Identifiable symptoms include loud snoring, observed apneas, and daytime sleepiness [6].
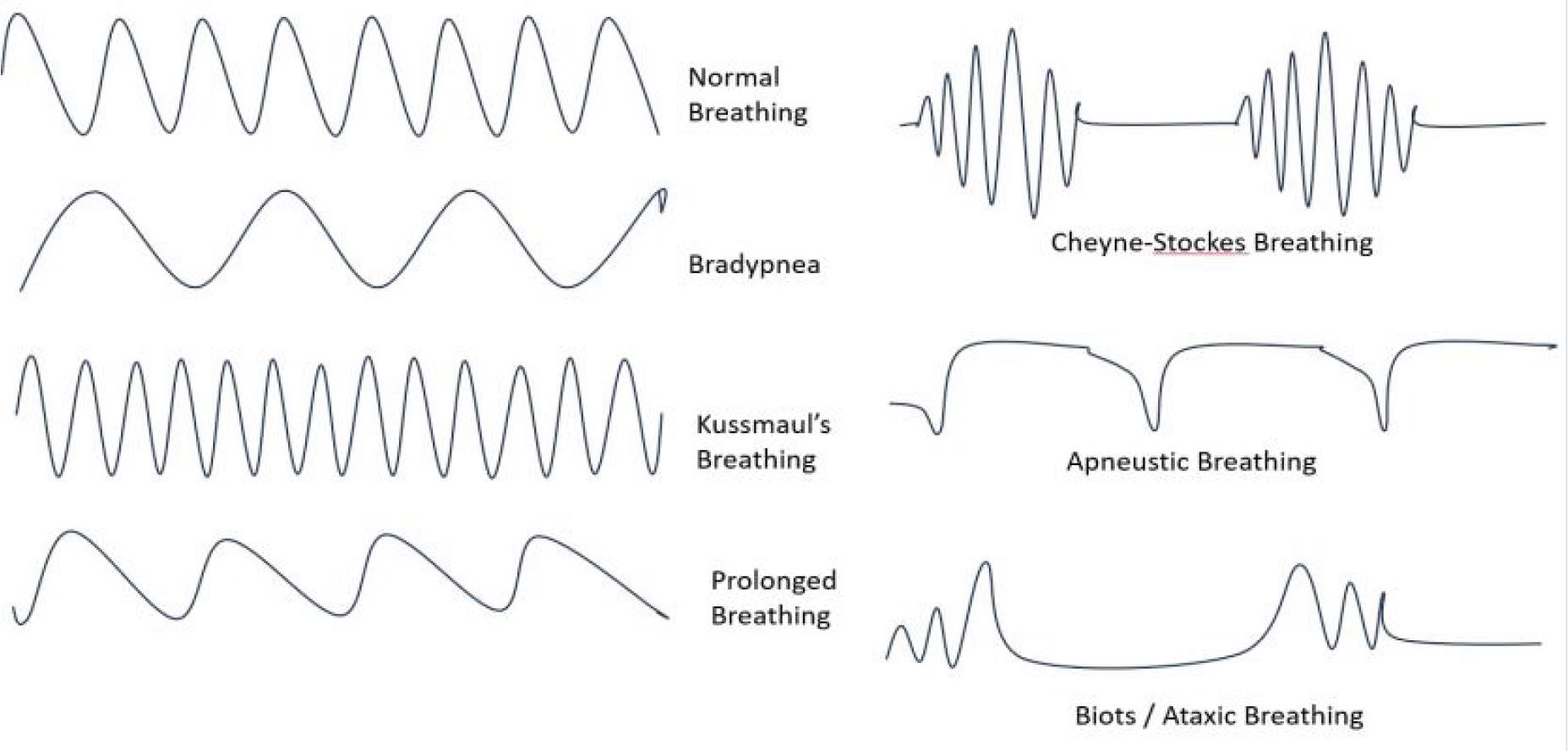
Breathing patterns
Sleep-Disordered-Breathing (SDB) Recognized as a significant health issue in young children, SDB has estimated prevalence rates of 1 percent to 4 percent, with contributing factors being a narrow airway and reduced neuromuscular tone. Children with conditions like Down syndrome are at higher risk. SDB symptoms include snoring, frequent arousal, enuresis, and hyperactivity, and if untreated, it can lead to learning challenges, stunted growth, and increased risks of hypertension and cardiovascular problems [7].
Since SA is sleep-related disorder, knowledge of sleep stages is important because it has been observed through the literature that SA occurs when a patient goes into deep sleep. There are two main types of sleep stages: the first one is nonrapid eye movement (NREM) sleep and the second one is rapid eye movement (REM) sleep.
NREM is subdivided into stages N1, N2, and N3. The characteristics of REM sleep are rapid eye movements, muscle atonia, and desynchronized brain activity [8].
Risk Factors of OSA: Obesity: The literature analyzed here suggests that patients with high BMI value is very likely to develop SA. Kandala et al. [9] investigated OSA in 30 participants with snoring history and a high Epworth sleepiness scale scores. Based on BMI, 23 patients were diagnosed with OSA (AHI > 5); out of these, 13 were obese and 10 were nonobese. Obese individuals exhibited lower mean oxygen saturation levels (SpO2) and experienced reduced total sleep time, sleep efficiency, N3 stage, and REM stage compared to nonobese patients. The same thing is highlighted by Reddy et al. [10]; they have assessed OSA occurrence and contributing factors in an urban Indian population aged 30 to 65, estimating a 9.3 percent population prevalence for OSA and 2.8 percent for OSA syndrome. Male gender, high BMI, and abdominal obesity were associated with OSA, with obesity found to be a major risk factor; they noted associations with hypertension, while the least significant risk factors were smoking and drinking. Their study also highlighted the fact that OSA is a common condition that causes interrupted breathing during sleep, affects various age groups (prevalence: 2 percent to 14 percent), and leads to fragmented sleep and daytime sleepiness. Linked health issues include hypertension and heart disease, with predictive features like snoring and obesity. Diagnosis involves polysomnography (PSG), and the primary treatment is the continuous positive airway pressure (CPAP) machine, with bariatric surgery considered for obese patients.
If SA is left untreated, its consequences can be fatal. Some of the following articles discuss links between SA and other diseases. According to Gurubhagavatula et al. [11], OSA can cause daytime sleepiness and cognitive impairments, affecting vigilance, memory, concentration, and executive function, thus increasing the risk of accidents and diminishing overall quality of life. Treatment of OSA has demonstrated improvements in these areas. Researchers like Martin et al. [12] highlight the impact of OSA during pregnancy, linking it to adverse outcomes such as preeclampsia and gestational diabetes. Fatima et al. [13] emphasize that OSA is prevalent, affecting about 20 percent of US adults, with a higher incidence in obese individuals and males. Home studies reveal that 7.5 percent of middle-aged Indian men have OSA. The connection between OSA and CVD is of interest due to their potential mechanisms, but the impact of OSA treatment on cardiovascular risk remains uncertain.
Many researchers discuss SA and kidney diseases. Anker et al. [14] highlight the common occurrence of SDB in CVD and its impact on outcomes. It discusses the two main SDB types, diagnostic considerations using PSG or portable devices, and effective treatments like CPAP for OSA. The optimal treatment for CSA in heart failure is uncertain, with emerging therapies like phrenic nerve stimulation under exploration. Targa et al. [15], in their study, explored the link between OSA events and their impact on sleep patterns, Alzheimer markers, and cognitive decline in 116 patients (median age: 76, AHI: 25.9). Obstructive apneas were related to sleep disruptions, while hypopneas were linked to increased arousal, and both mixed and central apneas affected sleep structure. At the 12-month follow-up, hypopneas were the most significant predictor of greater cognitive deterioration, and OSA was connected with raised neurofilament light levels. Mavanur et al. [16] showed that SDB is common in advanced chronic kidney disease (CKD), affecting over 50 percent. It leads to upper airway blockage during sleep, causing physiological reactions and increased cardiovascular risks. Treatments like renal transplantation and specialized dialysis methods show promise in reducing SDB severity in CKD patients.
For diagnosis of SA, sleep experts usually monitor ECG [17–21], EEG [22], SpO2 [23], snoring sound, and various other body parameters of the patient. Sharma et al. [24] emphasized that due to lack of awareness about OSA in India, the Ministry of Health and Family Welfare established INdian initiative on Obstructive sleep apnoea (INOSA) guidelines. These guidelines recommend a sleep assessment, particularly for individuals showing symptoms like snoring and daytime sleepiness or those who were considered high-risk cases. PSG is the standard diagnostic method, and positive airway pressure (PAP) therapy is the primary treatment, with oral appliances and bariatric surgery considered for specific cases.
In line with this, Huttunen et al. [25] showed that, by utilizing polysomnographic data from 877 participants, this model enhances the assessment of SA by taking into account each individual sleep stage. Using pulse oximetry data, it improves the accuracy of distinguishing between apnea and hypopnea, and its ability to estimate AHI during REM and NREM sleep makes it valuable for OSA screening and treatment. Korkalainen et al. [26] proposed an effective DL-based automatic sleep stage classification method that shows reliable results for subjects with varying degrees of OSA. This approach, especially when single or frontal EEG channels are used, is a cost-effective and accurate alternative to OSA diagnosis.
Many research articles underline the application of ECG signals for SA diagnosis. Pombo et al. [18] investigated the use of classifiers to identify episodes of SA from minute-to-minute ECG signals. ECG-derived respiration (EDR), heart rate variability (HRV) are the characteristics used in a study to examine the accuracy and performance of various classifiers. The highest accuracy attained was 82.12 percent, accompanied by 88.41 percent sensitivity and 72.29 percent specificity.
Table 3 shows variety of data used by researchers across the world to address research questions concerning SA classification. The data components encompass subject demographics, data sets of ECG signal data, EEG signals, and SpO2 related to SA. Data sets were also obtained through various kinds of wearable sensors like smart watches, pulse oximeters, SA rings, smart body sensors, and nasal cannulas.
Subject demographics
| Author | Data Sample Size (N) | Male (M) | Female (F) | Age Range/Mean Age | Time Frame | Type of Data |
|---|---|---|---|---|---|---|
| Peppard et al. [3] | 1520 | – | – | 37–85 | 2000–2015 | PSG |
| Han et al. [27] | 4014 | 2841 | 1173 | 53 | 2014–2021 | PSG, ESS questionnaire |
| Shi et al. [28] | 1493 | 1269 | 224 | – | 2019–2021 | PSG |
| Targa et al. [15] | 116 | 52 | 64 | 72–80 | 2015–2019 | PSG |
| Zarei et al. [29] | 25 | 21 | 04 | 28–68 | 2011 | PSG |
| Huttunen et al. [25] | 877 | 480 | 396 | 44–65 | 2015–2017 | PSG |
| Pombo et al. [18] | 70 | 57 | 13 | 27–63 | ECG |
A large volume of literature is available that shows how the CPAP machine is effective in SA treatment. CPAP is the first choice of medical experts. Some of the following literature highlighted the use of CPAP. Jané [30] highlighted that standard treatment involves CPAP therapy; their research focuses on adaptive pressure algorithms and emerging trends aimed at enhancing patient engagement through mobile apps and web platforms such m-Health and Tele-Health. Similarly, authors like Senavongse et al. [31] discuss the affordability issue of CPAP machines for treating OSA and present a study designing a functional prototype. The prototype, demonstrating accurate measurements and potential improvements, shows promise for clinical trials in addressing OSA and snoring. Amrulloh et al. [32] presented an on-demand CPAP (OCPAP) controller as an alternative SA treatment, adapting air pressure based on respiratory needs for enhanced comfort and upper airway muscle training. Developed with LabView, the model demonstrated promising results in performance tests, offering potential for a low-cost treatment option, particularly in Indonesia, to reduce dependence on traditional CPAP systems.
Some authors have discussed advances in the CPAP machine and their use in SA treatment. Boisteanu et al. [33] compared automatic CPAP (APAP) to a fixedpressure CPAP in moderate to severe OSA patients; the study suggests that APAP is as effective, offering a slightly lower effective pressure. Intelligent CPAPs with remote-monitoring capabilities can reduce costs and doctor visits, making them a potential choice for long-term treatment. Penzel et al. [34] investigated how OSA affects cardiovascular and respiratory regulation during different sleep stages, focusing on patients with OSA and normal blood pressure, OSA and hypertension, and normal controls.
Researchers have discussed other popular treatment options as well, such as the mandibular advancement device (MAD). Daga et al. [35] assessed sleep quality before and after using an MAD and participating in yoga. While the MAD group showed immediate improvements with compliance issues, the yoga group demonstrated sustained benefits over the long term, indicating the effectiveness of yoga and pranayama practices in long-term management of OSA.
The literature available on SA suggests the use of advanced technological options such as adaptive servo-ventilation (ASV) for CSA treatment. Aurora et al. [36], according to a recent systematic analysis, showed that ASV enhanced left ventricular ejection fraction (LVEF) and normalized the apnea-hypopnea index (AHI) in patients with CSA associated with congestive heart failure. Webster et al. [37] proposed a novel SA treatment device comprising a mask, hose, and CO2 chamber, that automatically adjusts rebreathed air to reduce apneas without PAP, offering a potentially more effective and comfortable treatment for the over 25 million Americans affected by SA.
In conclusion, the available literature suggests that there are continuous improvements going on to make CPAP, MAD, ASV, and SA monitoring devices better and more patient-friendly. There is future research scope in this field to incorporate artificial intelligence (AI) and advanced ML and DL algorithms to make these devices intelligent, with automated pressure settings.
Treatment options for SA
| Author | Treatment | Observations | Improvements |
|---|---|---|---|
| Boisteano, et al. 2009 [33] | fixed CPAP, ACPAP | ACPAP effectively lowers pressure. It is a long-term treatment option. | Intelligent CPAP with remote monitoring can reduce frequent doctor visits, reducing overall cost. |
| Penzel et al. 2011 [34] | CPAP | OSA affects cardiovascular, respiratory regulation during sleep | CPAP affects cardiovascular coupling during deep sleep; baroreflex sensitivity response varies across sleep stages. |
| Jané, 2014 [30] | CPAP, adaptive pressure algorithm, M-Health, Tele-Health | OSA disrupts airflow during sleep; SpO2is also reduced. | Standard treatment option is CPAP, advanced CPAP with adaptive pressure settings. |
| Aurora et al. 2016 [36] | ASV for CSA patients | Cardiac mortality rate is high for LVEF >= 45%, moderate-severe CSA. | ASV suggested for patients with LVEF >45% and mild-moderate CSA. |
| Senavongse et al. 2017 [31] | A low-cost functional prototype is designed. | Modern CPAP machine is not affordable to everyone nowadays. | The functional prototype demonstrates accurate measurements and improves OSA, snoring treatment. |
| Webster et al. 2018 [37] | Novel SA treatment device consisting of mask, hose pipe, CO2 chamber. | Device automatically adjusts rebreathed air to reduce apneas. | No need for CPAP |
| Amrulloh et al. 2019 [32] | OCPAP controller developed using LabView software | OCPAP adapts air pressure based on respiratory needs | Low-cost treatment option that reduces dependency on CPAP. |
| Daga et al. 2021 [35] | MAD and yoga exercise | Sleep quality is assessed before and after MAD surgery. | MAD group showed immediate improvements while the yoga group showed sustained improvements over a long time period. |
Physiotherapy treatments like yoga, asanas, and oral exercise have proven effective in SA treatment; see Table 5 for noninvasive treatment options for SA. Kumar et al. [38] studied individuals suffering with mild-to-moderate SA and snoring; they recommended physiotherapy with different yoga postures. A three-month yoga program demonstrated positive impacts on breathing patterns, oropharyngeal musculature, and respiratory concerns, providing symptomatic relief for the 23 participants. Bankar et al. [39] showed that in comparison to the control group, the yoga group scored higher on quality-of-life components and had a minimized Pittsburgh Sleep Quality Index (PSQI) sleep quality value. Yoga participants reported fewer sleep disturbances, shorter sleep latency, reduced reliance on sleep medications, and better subjective sleep quality and habitual sleep efficiency scores. Regular yoga practice appeared to positively influence sleep quality and overall wellbeing in the elderly. Researchers have emphasized regularly doing yoga, asanas, and exercises can help overcome illnesses like SA; see Table 5 for a comparative study. Khalsa et al. [40] compared Kundalini yoga to sleep hygiene for insomnia; both interventions improved sleep, but yoga showed larger effects, suggesting that self-care yoga interventions can provide lasting improvements in sleep quality beyond traditional approaches.
Physiotherapy treatment for SA
| Author | Sample Size | Treatment | Improvements |
|---|---|---|---|
| Kumar, 2019 [38] | 23 | Yoga program for 3 months for mild-to-moderate SA and snoring issues | Positive impact on breathing pattern, oropharyngeal musculature, respiratory concerns. |
| Bankar, 2013 [39] | 2 groups | Two groups of SA patients formed; control group and yoga group | Yoga group scored higher quality of life PSQI value, reduced sleep disturbances, shorter sleep latency. |
| Khalsa, 2021 [40] | 2 groups | Two groups of insomnia patients formed: Kundalini yoga and sleep hygiene | Kundalini yoga group showed improved sleep quality |
| Kanchibhotla, 2021 [41] | 473 | Sudarshan Kriya yoga and breathing exercise | Positive impact on sleep quality. Improvement varied among patients based on age, gender, yoga practice frequency. |
| Kwiatkowska, 2008 [42] | – | Fuzzy logic-based treatment method to classify physical activities performed by OSA patients based on IPAQ | Improves monitoring of effectiveness of CPAP treatment, physical activities performed. |
| Khobarkar, 2022 [43] | – | Abhyanga Utsadana, Basti, oral medication with bitter herbs | Improvement shown in blood sugar level, BMI, waist-to-hip ratio, categories of BSQI. |
Kanchibhotla et al. [41] studied Sudarshan Kriya Yoga (SKY), a breathing exercise, involving 473 participants; they found that regular SKY practice positively impacted sleep quality, with the extent of improvement varying based on age, gender, and practice frequency; they emphasized a positive correlation between daily SKY practice and substantial enhancements in sleep quality.
Many researchers have explored the use of homeopathic medicine for SA treatment, as shown by authors like Broadway et al. [42]. They proposed a fuzzy logic method based on the International Physical Activity Questionnaire (IPAQ) to classify physical activities performed by patients of OSA; the method improved precision over traditional assessments and allowed for better monitoring of changes in physical activity and the effectiveness of CPAP treatment in respiratory clinics. Nakanekar et al. [43] proposed treatment methods, including Abhyanga, Utsadan, oral medications, and Basti, with a focus on bitter herbs; there were positive effects on respiratory patterns during sleep. Blood sugar level, weight, belly size, BMI, waistto-hip ratio, and categories on the Berlin Snoring Questionnaire all improved when Basti was used.
An ample amount of literature is available on the application of ML in SA diagnosis; see Table 6 for a comparative study. Han et al. [27], in their study, evaluated ML techniques for OSAS severity assessment using demographic and questionnaire data from 313 patients. For classification, random forest and support vector machine (SVM) models performed best, yielding the highest accuracy of 44.7 percent, with misclassification observed in only 5.7 percent of cases. Linear regression and the SVM model performed well in predicting the AHI, with regression models achieving a minimum RMSE = 22.17. Similarly, Alvarez et al. [44] used regression and SVM techniques, discovering that in terms of forecasting the AHI, the dual-channel technique performed better than individual oximetry and airflow, showcasing high complementary value, and significantly improving accuracy for efficient at-home screening of OSA.
ML algorithms for SA diagnosis
| Author | Bio signal | ML Algorithm | Performance | Type of Classification | ||
|---|---|---|---|---|---|---|
| Accuracy (%) | Sensitivity | Specificity | ||||
| Sharma et al., 2023 [49] | EEG | K-NN, ensemble bagged trees (EbagT) | 92.85 | – | – | detection |
| Mencar et al., 2020 [50] | Questionnaire based data | SVM, RF, LR | 44.7 | – | – | prediction |
| Álvarez et al., 2020 [44] | SpO2, BP, HR | LR, SVM | 81.3 Kappa coefficient = 0.71 | – | – | AHI prediction |
| Shi et al., 2022 [28] | BP, SpO2 | GBM, XGBOOST | 88.5 | 0.713 | 0.873 | prediction, hypertension |
| Kristiensen et al., 2018 [51] | ECG | RF, KNN, SVM, ANN | 87.47 | – | – | classification |
| Pombo et al., 2020 [18] | ECG | SVM, LR | 82.12 | 0.8814 | 0.7229 | classification |
| Schrader et al., 2000 [52] | ECG, HRV | LDA | 88.31 | – | – | classification |
| Lin et al., 2006 [53] | ECG | DWT, ANN | – | 0.6964 | 0.4444 | classification |
| Xie & Minn, 2012 [54] | SpO2, ECG | KNN | 84.80 | – | – | prediction and classification |
Researchers have found that ML algorithms, along with body parameters like SpO2, can be used for SA diagnosis. Shi et al. [28], in their study involving 1493 OSA patients and 27 variables, including hyper tension, learned that ML algorithms, and particularly, the gradient-boosting machine (GBM), to be the most reliable in predicting hypertension associated with OSA (AUC = 0.873, accuracy = 0.885, sensitivity = 0.713). The identified key variables, including age, minimum arterial oxygen saturation, BMI, and percentage of time with SaO2 < 90 percent, led to the development of an online tool for clinicians [28]. Researchers like Liu et al. [45] emphasize the importance of detecting non-apnea-related arousals during sleep for assessing sleep quality. The proposed algorithm trained and tested on PSG data utilizing convolutional neural networks (CNNs) and a random-forest module, achieved an Area Under the Precision-Recall Curve (AUPRC) of 0.552.While effective, the method may have limitations for certain patients.
Authors have discussed the use of ML for judging/monitoring treatment provided to SA patients. Mitri et al. [46] discussed the use of CPAP, applying air pressure for conditions like SA and preterm infants, with a focus on anomaly detection aided by ML using the Numenta Anomaly Benchmark (NAB) and Hierarchical Temporal Memory (HTM). An experiment using infant breathing patterns demonstrated effective anomaly prediction, emphasizing the potential of HTM in anomaly detection, though its immaturity limits progress, suggesting the need for future work to solidify its competitiveness in ML research. Fallamnn et al. [47] comprehensively reviewed technological advancements in sleep monitoring, addressing sleep behavior characterization, assessment methodologies, monitoring techniques, and analysis methods within personalized smart health care, emphasizing the potential for data-driven techniques to bridge the gap between clinic-based and home-based sleep assessments. Rao [48] explored wearable sensors for respiratory and pulse monitoring, emphasizing technologies like heart rate monitoring, GPS, GSM, IoT, and infrared-based breath sensors, aiming to enable selfmonitoring of health parameters and improve health care technology through ML techniques and an innovative system leveraging IoT and GSM platforms.
The accuracy of ML methods applied for SA diagnosis can be improved by considering combination of signals instead of individual signals; ECG-SpO2 [54], ECG-nasal pressure, SpO2-EEG [44], ECG-EEG, ECGchest-abdomen signal combinations can be tried. Limitations with standalone ML algorithms include the lack of feature extraction/optimal feature selection ability; hence, hybrid combinations ML models with optimization algorithms should be tested [e.g., particle swarm optimization (PSO), genetic algorithms (GAs), blue whale (BLO), and gray wolf (GWO)]. In order to enhance performance measures of ML approaches, researchers have tried hybrid approaches like CNNLSTM, PSO-SVM, and HRV-LDA [52].
DL has shown very promising results in diagnosis and processing of signals received from SA-suspected patients. Feature extraction and optimal feature selection were the key points of DL algorithms like CNNs and recurrent neural networks (RNNs). We have presented a comparative study of various DL methods applied in SA prediction; see Table 7. Sun et al. [55] presented a classification of sleep stages, a two-stage neural network strategy that uses an RNN for temporal input processing and feature learning, along with a pretraining procedure to address sample imbalance. Tests on sleep databases demonstrate superior performance compared to advanced methods, achieving significant F1 scores and Kappa coefficients.
DL algorithms for SA diagnosis
| Author | Bio signal | DL Algorithm | Performance | Type of Classification | ||
|---|---|---|---|---|---|---|
| Accuracy (%) | Sensitivity | Specificity | ||||
| Huttunen, 2023 [25] | SpO2, PR, ECG | CNN, RG | – | – | – | detection |
| Sharma et al., 2022 [49] | SpO2, PR | CNN | 93.4% | – | – | detection |
| Strumpf et al., 2023 [56] | SpO2, HR | ANN | 91% | 0.83 | 0.76 | multiclass classification |
| Hemrajani et al., 2023 [57] | ECG | RNN, LSTM, GRU. | 89.5% RNN; 90% LSTM; 90.5% GRU | – | – | classification |
| Korkalainen et al., 2021 [26] | EEG, SpO2 | CNN, RNN | hazard ratio = 1.14 (p = 0.39) for mild OSA | hazard ratio = 1.59 (p < 0.01) for moderate OSA | hazard ratio = 4.13 (p < 0.01) for severe OSA | estimation |
| Liu et al., 2020 [45] | EEG, SpO2 | CNN, RF | AUROC = 0.95 | AUPRC = 0.552 | – | detection |
| Mitri et al., 2017 [46] | Nasal pressure, CPAP pressure readings | HTM, NAB | – | – | – | anomaly detection |
| Sun et al., 2019 [55] | EEG | RNN | – | – | – | binary classification |
| Yung et al., 2020 [58] | ECG | 1D-CNN | 89% | – | – | detection |
| Zarei et al., 2021 [29] | ECG | CNN-LSTM | 97.21% | 94.41 % | 98.94% | detection |
Abbreviations: GRU, gated recurrent unit; PR, pulse rate.
Researchers like Kristiansen et al. [51] have investigated the use of data mining methods, such as decision trees, random forests, SVMs, K-nearest neighbor (KNN), and artificial neural networks to examine physiological signals for the purpose of detecting OSA, utilizing data sets from the MIT-BIH and Apnea-ECG databases [51]. Other authors like Yang et al. [58] utilized a 1D-CNN model on onechannel EEG data with sleep-stage annotations, demonstrating higher accuracy for intrapatient insomnia identification, particularly leveraging REM and SWS epochs, compared to baseline methods, while finding no significant differences in interpatient identification.
Many researchers stressed the use of ensembled ML/DL algorithms as Kwon et al. [59] have; they presented a novel method using IR-UWB radar and DL algorithms for real-time apnea-hypopnea identification in SA and hypopnea syndrome, achieving high performance with a strong association between estimated and reference AHIs. Zarei et al. [29] introduced an automated approach utilizing ECG signals and a combination of CNNs with LSTM networks for SA detection, achieving impressive results with higher sensitivity (94.41 percent), specificity (98.94 percent), and accuracy (97.21 percent) on Apneic and UCDDB data sets. The LSTM-CNN model outperforms traditional methods, providing accurate per-segment and per-recording classifications, thereby enhancing SA diagnosis for physicians.
Researchers have also presented the use of pretrained neural networks in SA diagnosis. Hemrajani et al. [57] presented MobileNet-V1, LSTM, and GRU networks for identifying single-lead ECG signals in undiagnosed OSA cases, achieving accuracy rates of 89.5 percent, 90 percent, and 90.29 percent on authentic cases. Sharma et al. [49] work presented an automated technique that uses pulse-oximeterrecorded SpO2 and PR data to identify episodes of SA. For epoch-based apnea detection, the DL model obtained a test performance of 90.4 percent area under the ROC curve and a 58.9 percent area under the precision-recall curve after being trained on a heterogeneous cohort of patients.
The IoT, along with health-monitoring devices, has a very wide scope in the field of health care monitoring. Kwon et al. [60] introduced a portable athome solution that uses wearable electronics with embedded ML and wireless sleep sensors to solve the problem of undetected sleep disorders. Clinical testing demonstrates a comparable performance to PSG in capturing brain, eye, and muscle signals. The wearable system accurately identifies OSA with 88.5 percent precision. Steblin et al. [61] introduced an IoT-based solution to improve the treatment of OSA. To assist patients with OSA and provide feedback to lung specialists, the suggested technology transmits patient data to the cloud for analysis.
Many researchers have tried to emphasize the important role of the IoT and ML/DL combinations in SA diagnosis. Abdel-Basit et al. [62] explored the challenges in detecting and treating OSA and highlighted the potential of AI-driven IoT technologies for remote patient monitoring, providing an overview of developments from 2016 to 2019 in big data, cloud computing, ML, smart devices, and fog computing.
Recommender systems (RSs) give recommendations based on user profile. Here, in the case of SA treatment recommendations, authors have proposed various approaches of RSs in collaboration with ML/DL algorithms; see Table 8. Nanehkaran et al. [63] introduced a medical recommendation system utilizing IoT devices, employing KNN classification for disease identification and collaborative filtering for treatment recommendation. The approach shows high precision in diagnosing chronic diseases and recommending treatments, surpassing previous methods. Other authors, like Casal-Guisande et al. [64], presented an intelligent system for diagnosing OSA. The system combines patient health data and symptom information to generate risk indicators for OSA. The early testing of the system showed promise, but further clinical validation and improvements are needed before it can be widely used in hospitals.
Recommender System for SA
| Author | Disease Prediction | Recommender System | ML/DL Algorithm | Data Set Used |
|---|---|---|---|---|
| Nanehkaran, 2022 [63] | Chronic Disease | collaborative filtering | K-NN classifier | PhysioNet data repository |
| Raza et al. 2023 [65] | SA | two-stage recommender system; precision = 89%, macro-average F1 score = 84% | – | MIMIC data set |
| Kaneriya et al. [68] | SA | Markov decision-based recommender system | Hidden Markov Model | – |
| Pinon et al., 2023 [66] | – | federated learning recommender system | – | historical disease-drug interactions and drug data |
| del Rio et al., 2023 [67] | Chronic Disease | – | restricted Boltzmann machine | wearable sensors connected on patient’s body |
| Casal-Guisande et al., 2023 [64] | OSA | personalized recommendation | ML classifier with fuzzy expert system | data set with 4400 patients from the Álvaro Cunqueiro Hospital (Vigo, Galicia, Spain) |
| Torres-Ruiz et al., 2023 [69] | COVID-19 | collaborative filtering | – | – |
| Chinyere et al., 2023 [70] | Hospital Recommendation | collaborative filtering | – | data collected through mobile/web application |
We have analyzed research articles on the application of RS in the health care domain utilizing electronic health records (EHRs). Raza et al. [65] introduced a two-stage recommender system for clinical decisionmaking with the help of EHRs. The first stage retrieves candidate items based on patient records using a deep neural network and a language model. The second stage ranks and recommends relevant items considering patient history and context. Pinion et al. [66] proposed a federated learning architecture for health recommender systems (HRSs) in precision medicine, addressing privacy concerns and enabling a real federated HRS without compromising confidentiality. In this research, they evaluated an HRS developed for the TeNDER-project, which provides personalized recommendations based on monitoring device data. The notifications covered various aspects of daily life.
However, other authors, like del Rio et al. [67], have proposed a recommendation system that suggests a healthy lifestyle schedule to mitigate SA severity. A probabilistic Markov model (PMM) guides activities based on patient time allocation, aiming to reduce apnea cycles and improve sleep patterns. The system uses a hidden Markov model for condition-directed recommendations, focusing on flexibility and user preferences.
Figure 4 shows a proposed HRS. It involves processes like feature engineering and selection, initial stages of HRSs we need to identify, and relevant features (e.g., SpO2, blood pressure, sleep habits, patient demographics such as age, gender, BMI, and neck circumference. Data should be preprocessed (i.e., cleaned and normalized) before feeding into an ML/DL algorithm. Before algorithm selection, we need to investigate various ML algorithms. HRSs may require DL techniques (CNNs and RNNs) for better prediction results. There is a need to optimize hyperparameters (learning rate, regularization). Ensemble methods can be used by combining predictions from multiple models. Performance evaluation metrics such as accuracy and recall can be considered, and cross-validation methods like k-fold cross-validation can be used to improve HRS performance. Domainspecific knowledge, such as collaboration with sleep medicine specialists, is essential. Understanding clinical implications is also very important.
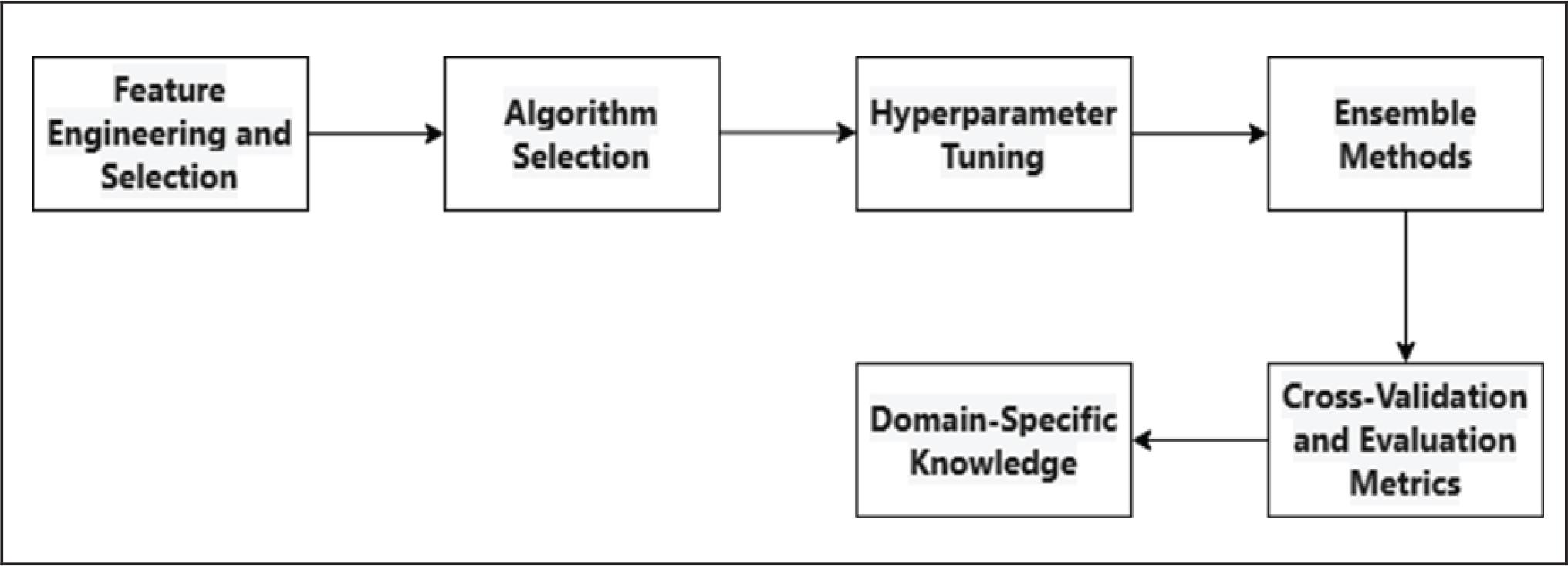
Workflow for an HRS for SA
To demonstrate its efficiency and effectiveness in the health care industry, the study [71] presents a Healthcare Monitoring System (HMS) that combines IoT and ML technologies. It does this by using wearable sensors for real-time monitoring and a medical decision support system for the detection and analysis of health issues.
Researchers across the world have explored the field of AI for SA diagnosis and the role of AI in assisting in SA treatment. In line with this, Kaneria et al. [68] developed an automated DL method called DOSED to detect sleep-breathing events in PSG recordings, which are used to diagnose OSA. The performance of the method was compared to the precision of human sleep experts in diagnosing the severity of OSA and detecting individual breathing events. Furthermore, Thorey et al. [72] reviewed publications from 1999 to 2022 to explore AI’s role in improving OSA treatment. AI can predict treatment outcomes, evaluate current treatment effectiveness, and enhance understanding of OSA mechanisms. Strumpf et al. [56] have designed Belun-Ring and tested its performance, involving 84 participants and comparing the Belun-Ring results with in-lab PSG. They found that the Belun Ring with BSP2 algorithms accurately detected OSA, classified its severity, and classified sleep stages.
SA detection using ML and DL approaches is strongly reliant on high-quality data. Researchers face numerous issues linked to data availability, privacy, and secrecy. Here are the main issues:
- 1)
Obtaining labeled SA data is challenging owing to the specialized nature of the study and the necessity for expert comments.
- 2)
Researchers frequently use publicly available data sets to construct and test their models. These databases are critical to developing SA research.
- 3)
Data privacy and confidentiality. Sleep-related information, including physiological signals (electroencephalography, electrocardiography, and breathing patterns), is sensitive and personal. Maintaining patient privacy and adhering to ethical rules are critical. Researchers must keep data anonymous and secure.
- 4)
National Sleep Research Repository (NSRR). The NSRR is an excellent resource for SA researchers. It hosts a variety of sleep problem data sets, including SA. Researchers can examine many sorts of data, including PSG recordings, actigraphy data, and clinical information.
Table 9 contains information about specific data sets important for SA research.
Various Data sets available for SA
| Data Set | Sample Size | Types of Signals | Time Range | Male | Female |
|---|---|---|---|---|---|
| UCDDB data set/St. Vincent University Hospital, Dublin [73] | 25 | 3-channel ECG | 6 months | 21 | 4 |
| Wisconsin Sleep Cohort [74,75] | 1545 | PSG, multiple sleep latency test | 1989–1993 | 1000 | 545 |
| STAGES -Stanford Technology Analytics and Genomics in Sleep [75] | 1500 | PSG | – | – | – |
| Apnea-ECG database [76] | 70 | ECG | 7–10 h | ||
| MIT-BIH [73] | 18 | PSG | 80 h | – | – |
| Sleep Heart Health Study (SHHS) [75,77] | 6441 | PSG | 1995–1998 | – | – |
SA is a sleep-related disorder that has severe consequences if not treated on time. To detect SA at an early stage, ML and DL methods are crucial. These methods can be applied to signals collected from a patient. Signals such as ECG, EEG, and SpO2 are very useful in diagnosis, but the availability of such realtime data is big hurdle that needs to be addressed. There is a lot of scope for future research in the direction of optimal feature selection from these signals and the testing of ensemble ML/DL techniques to elevate prediction accuracies. An HRS can recommend some lifestyle changes, treatment recommendations, or a doctor or hospital recommendation to patients suffering from SA. These technologies help to diagnose and effectively treat patients with SA. In parallel, SA patients can do regular oropharyngeal exercise, yoga, and pranayama which have proved to be long-term, effective, and noninvasive treatments.