
Distal radius fracture (DRF) is the most frequent injury of the upper limb [1–4]. This fracture often occurs in the group of women over 65 years of age suffering from low-energy injuries and for young men suffering from high-energy injuries, which are often associated with sports activities, high-altitude falls or traffic accidents [3,5,6]. Due to the large number of fracture types, many classifications have been used, introducing the division according to specific criteria, which allows determination of correct treatment and possible complications. Because of a good healing potential of these type of fractures, as well as, rare occurrence of nonunion or formation of pseudoarthrosis, patients are usually treated conservatively [7,11]. Comminuted fractures, interarticular fractures, fractures after unsuccessful reposition or with secondary fracture displacement require surgical treatment. The most common methods of surgical treatment are: close reduction and internal fixation (CRIF), open reduction and internal fixation (ORIF) or external stabilization [4,7,8]. Żyluk and Janowski [9] found that DRF treated conservatively leads to displacement in load 30-50% of cases, which is why the tendency to use ORIF technique prevails today among unstable fractures [4].
Anyone who sustains an upper limb fracture will experience a period where they have difficulty participating in personal, occupational and sporting activities that may extend to 12 months beyond the time of fracture [10,11]. The degree of difficulty may be related to the type of fracture, length and position of immobilization or any complications such as CRPS. Problems during treatment are most often associated with pain and swelling [12]. Pain consequently makes it difficult to perform everyday activities, which many patients did not have previously had difficulties with [12]. Research by Ydreborg et al. [13] showed that despite regaining the range of mobility (ROM) and grip strength in 12 months, pain during rest and activity was still a problem.
Immobilization of one of the limbs prevents bimanual use of upper limbs, which leads to problems with performing basic activities of daily living (ADL), such as bathing, dressing, undressing and self-catering. In addition, problems with the upper limb can cause dependence of patients on other people. Immobilization of the limb also limits the mobility, which together with the weakening of muscle strength results in graphomotor problems as well as manipulative problems.
Distal radius fractures also occur in people at working age, which can significantly impede the performance of paid work during the rehabilitation period [14,15]. Valdes et al. [16] points out that pain has a significant impact on the performance of paid work among the DRF, which is an area for an occupational therapist who prepares the patient to return to work.
Considering that the upper limbs form the foundation for performing basic (ADL) and instrumental ADL (IADL), the occurrence of a fracture leads to some limitations in the performance of activities and functional independence [17]. A study by Vergar et al. [17] showed that for about 23-24% of people after breaking, the limitations persist after 6 months from the injury. Limitations of limb activity during exercise may be caused by a decrease in ROM, pain, swelling or weakness in muscle strength [13]. During the fracture injuries there are also possibilities of soft tissue damages, which is why later patients often present more physical and functional restrictions [18].
Occupational therapy (OT) is a crucial component in the process of comprehensive rehabilitation [15,19–21]. Occupational therapist cooperates with the patient after a fracture in the field of medical, social and vocational rehabilitation [20]. Occupational therapy through the therapeutic use of everyday activities is to ensure participation in various roles performed at home, work, school or in the community. The fundamental aim of therapeutic intervention is to support the beneficiary in order to provide him/her with the opportunity to participate in activities that are crucial, needed by the patient in everyday functioning or show willingness to perform them [19].
Although DRF is one of the most common fractures, current scientific research does not indicate a standardized, comprehensive rehabilitation program, which aims to optimize the functioning level of various patients. Current research carried out on the subject of a therapy program for people after breaking the DRF does not give univocal evidence about the superiority of any of the methods over others.
Taking into consideration the uncertainty about the role of exercise in the rehabilitation process after upper limb fracture, the aim of this review was to assess the efficacy of OT in the treatment of patients after DRF.
Due to the low availability of studies comparing occupational therapy with other forms of treatment, it was decided to include a review comparing physiotherapy [22–24] to the scope of occupational therapy. According to the definition of the International Classification of Functioning, Disability and Health (ICF), rehabilitation including both physiotherapy and OT includes comprehensive activities, among others, in the field of physiological impairments [25]. Occupational therapist during the first contact with the patient usually begins with reducing swelling, stiffness and increasing the ranges of motion and muscle strength, which was weakened by immobilization of the limb [15,22,26,27]. Working on these elements is necessary to regain hand lost functions. Occupational therapist at later stages of rehabilitation may advise the patient to perform activities of other departments e.g. ergotherapy or art therapy. The occupational therapist’s forms of work do not differ from the physiotherapist’s forms of work with the patient, especially after breaking over physiological impairments (e.g. ROM, swelling, strength of grip) [25].
In order to find clinical controlled trials used in the review, we conducted an electronic search without language restrictions using EBSCO and Pubmed. The following search terms were used: (occupational therapy AND distal radius fracture) or (rehabilitation AND distal radius fracture). Search results have been limited by the date of publication: January 2008 – December 2018. The electronic search was supplemented by a hand search of reference lists of relevant studies and reviews. Citation tracking and list checks of the included studies was performed also in previously used articles.
The reviewer examined study titles and abstracts to determinate if they satisfied the eligibility criteria (table 1). If there were any doubts about the suitability of a trial for review, its full text has been analyzed. Other researches were analyzed according to included criteria (fig. 1.). Finally, 10 trials were extracted for systematic review.
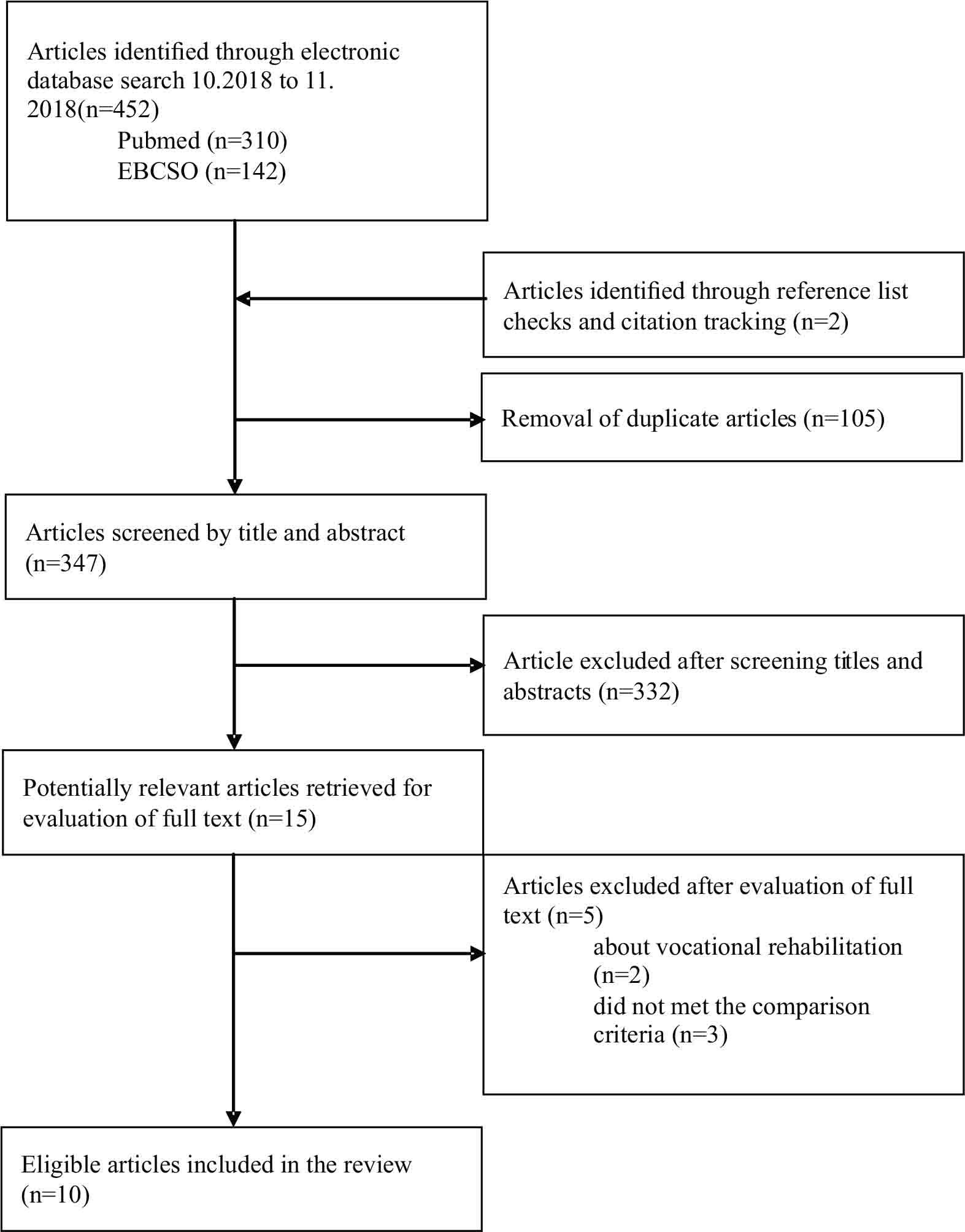
Flow of studies through the review
Inclusion criteria scientific research to review
| Design of the study |
|
| Participants |
|
| Intervention |
|
| Comparisons intervention |
|
The data extracted from eligible trials were: trial design, age, gender, inclusion criteria participants, description of the intervention, results measure and constraints research (exclusion criteria).
Ten studies comparising 490 participants who had sustained distal radius fracture. Over 71% participants of this study were female.
Seven trials evaluated the effect of therapy provided by an allied health professional that included supervised exercise plus home exercise program compared with home exercise program alone. Four of these seven assessed programs were led by an occupational therapist [15,28–30], two of them by a physiotherapist [16,22] and one by a hand therapist [24]. The remaining three trials evaluated the impact of exercise/advice following upper limb fracture by prescription of exercise only to the intervention group [23,31,32].
Six trials included patients during fracture immobilization period (first 5 weeks after fracture) [15,16,22,24,29,30]. In three trials the intervention began after immobilization (approximately 6 weeks after fracture) [23,28,32]. One trial did not contain information about the timing of intervention after the fracture [31]. Summary of included studies is presented in table 2).
Summary of included trials
| Trial | Design | Participants | Intervention | Result measure | Trial limitations |
|---|---|---|---|---|---|
| Bruder et al. (2016) [47] | RCT | EXP(n=19) | EXP – HEP (AROM, stretching and strengthening exercise wrist and forearm) and advice. The advice program included on movement, swelling, pain management, skincare, sleep and relaxation strategies, return to work (three consultation with PT in weeks 1,3,5 after removal of cast). | Primary endpoint: QuickDASH | Exclusion criteria: age >21 years, history of a pre-existing inflammatory joint condition, signs/symptoms CRPS, previous wrist fracture, bilateral wrist fractures, unable to understand written/spoken English, deficiency provide informed consent to participate Weak statistical power |
| Filipova et al. (2015) [38] | RCT | EXP(n= 30) | EXP – received to the same PT as control group and OT program – additional 9 session x 30 minutes (3 times in weeks). The OT strengthening program included different exercises for the hand, wrist, and forearm using functional samples movements CON – received PT (20 minutes galvanic baths and 30 minutes of individual kinesitherapy) 9 session for 3 weeks. The PT program included strengthening and gripping exercises | AROM, grip strength, DASH | Exclusion criteria: bilateral fracture, prior trauma of the wrist, malignant conditions and symptomatic osteoarthritis of wrist and hand, age > 30 years. |
| Kay et al. (2008) [43] | RTC | EXP(n=28) | EXP- standardized advice on fracture protection, swelling control, skin care and everyday activities, and one session of instruction to perform HEP (AROM exercises, soft tissue stretches, isometric stabilizing wrist, strengthening and grip exercises). The average duration of therapy is 13h. | Primary endpoint: wrist extension | Exclusion criteria: unwilling/unable to participate; unable to understand written/spoken English; bilateral wrist fractures; previous wrist fracture; concurrent ipsilateral limb injury, pre -existing inflammatory joint condition; managed with internal/external fixation. |
| Krischak et al. (2009) [39] | RTC | EXP(n= 23) | EXP (B) – supervised exercises program and HEP, advice and other interventions at PT. Received a prescription for a total of 12 sessions (20-30 minutes each), over a 6-week period. Patients were free to choose their own therapist, who were free to choose the type of therapy based on their own evaluation. | PRWE, grip strength, wrist ROM | Exclusion criteria: age>18 years, unwilling to participate, lacked the cognitive capacity, lacked self-sufficiency in managing the requirements of daily life, psychiatric illness, bone disease responsible for the treated fracture (i.e. bone metastasis, osteolysis), previous fracture near the wrist, inflammatory joint disease (i.e. rheumatoid arthritis) or reflex sympathetic dystrophy |
| Kuo et al. (2013) [45] | RCT | n=22 | EXP –exercises program supervised by OT and HEP. Group received 3 sessions (45 minutes) each per week until the external fixator was removed 6 weeks after fracture. After removing fixators, groups received regular rehabilitation programs (the same as Con group). | SF-36, grip and pinch strength, finger AROM, MAM-36, radiographic evaluation (volar tilt, radial inclination and radial height shorting) Measurement time: 1,3,6,12 weeks after surgery | Weak statistical power |
| Mitsukane et al. (2015) [46] | RCT | EXP(n=14) | EXP – received supervised wrist exercise (repeated 30 repetitive wrist extensions with maximal isometric 3 second hold and maximal extension than 3 second rest) and standard OT program. 30 repetitions were performed within 6 min (series of 10 repetitions/minute then minute rest). | Grip strength, pain (VAS), isometric strength of the wrist extension Measurement time: before and after 10 minutes exercises or relax | Exclusion criteria: bilateral fracture of upper limb Weak statistical power Lack of long-term outcome |
| Öken et al. (2011) [44] | CT | EXP(n=37) | EXP – each day for 3 weeks received rehabilitation in the hospital ward (passive ROM and wrist stretching exercises) under the supervision of a hand specialist. They were advised to do each exercise at home hourly, during the remaining part of the day. | ROM, grip strength - pinch gauge, grip strength, oedema Measurement time: before treatment and after 3 weeks rehabilitation | Exclusion criteria: age<18 years, previous fracture of the injured and/or non-affected hand, any systemic disorder (e.g. diabetes mellitus, infections, etc.), complication (e.g. CRPS, arthritis, etc.) |
| Sen et al. (2014) [34] | CT | EXP(n=15) | EXP – received detailed instructions, demonstration HEP, which were in a specially prepared exercise booklet. Each session has been taken for 30 minutes and twice in a day (30 session). CON – received in OT, supervised by therapist over 6-week period for 30 sessions (1 hour). Therapists based on their own evaluation (reduce pain/swelling, isometric, passive and active exercises, PNF Technique, exercises against light resistance) | Test MMDT, pain (VAS), ROM, grip muscle Measurement time: before and after intervention | Weak statistical power Lack of long-term follow-up results |
| Souer et al. (2011) [40] | RCT | n= 94 | EXP – exercises program supervised by OT (motion and strengthen the hand). The content, frequency and duration of the rehabilitation program were at the discretion of the therapist. | Wrist ROM, grip strength, DASH, pain (10 gradual scale), radiographic evaluation, CES-D, PCS, PASS Measurement time: 3 and 6 months after surgery | Exclusion criteria: age>18 years, other injury, DRF treated with alternative or ancillary fixation, patience not planning to return for follow-up care, relying on others for basic functioning |
| Valdes et al. (2015) [48] | RTC | EXP(n=26) | EXP – exercised program supervised by HT and HEP (passive and active exercises ROM, mobilization, retrograde and scar massage, stretching, sensorimotor activities, prehension training, functional performance activities). 2 times a week for 30 minutes to an hour (16 visits) CON – received the same standard pictorial HEP | Primary endpoint: PRWE [measurement time - 6 months] | Exclusion criteria: conservatively treatment or other method of stabilization, age >18 years, unable to understand written/spoken English |
(AROM – active range of motion; CES-D – Center for Epidemiologic Studies-Depression; CON – control group; CRPS – complex regional pain syndrom; CT – controlled trial; CTS – carpal tunnel syndrome; DASH - Disabilities of the Arm, Shoulder and Hand; DRF – distal radius fracture; EXP – experimental group; HEP – home exercise; HT – hand therapist; F – female; M – male; MMDT – Minnesota Manual Dexterity Test; OT – occupational therapist; PASS – Pain Anxiety Symptoms Scale; PCS – Pain Catastrophizing Scale; PRWE - Patient-Rated Wrist Evaluation; PT – physiotherapist; QuickDASH – short DASH; RCT – randomized, controlled trial; ROM – range of motion; SF-36 – short form 36, VAS – Visual Analogue Scale)
Research by Kay et al. [23] indicated that a single consultation with a qualified physiotherapist covering a programme of advice and exercise brought significant benefits in terms of activity, pain reduction and increased satisfaction with the improvement process in comparison to the control group that did not receive any sort of intervention (natural health restoring process). Kay et al. [23] believe that these results are of clinical significance. However, no significant differences were found between groups in terms of the primary result - wrist extension nor secondary results for other ranges of movement and gripping force [23].
No significant difference was found between results of individual patients after distal radius fracture, who performed a six-minute exercise programme of wrist extension and the group where no intervention was conducted. The group performing the exercise experienced grip force increase, however it did not result in pain alleviation therein. Mitsukane et al. [31] found that pain did not correlate with grip strength increase.
There is no proof that adding exercise to the advice programme has a positive impact on decreasing the limitations and handicaps of DRF patients. One study found no difference in upper limb activity between patient groups, which received a programme of exercise and advice and those that received only advice during three consultations with a physiotherapist on the subject of basic activities connected with the QuickDASH assessment at week 7 and week 24. Also, no differences were found in secondary results that included the scope of mobility, grip strength and pain [32].
Research by Filipova et al. [28] proved that combination therapy, i.e. OT and physiotherapy in conjunction, is more effective in decreasing the limitations after distal radius fracture. It was proven that introducing occupational therapy between week 8 and week 16 after the fracture to the rehabilitation process has indeed significantly improved the grip strength for up to a month from completing the 3-week exercise programme. However, no differences were found in the scope of activity, measured with the DASH Questionnaire [28].
One study indicated that OT was comparable or slightly worse from independent exercises after surgical treatment of unstable DRF [29]. Two studies showed greater effectiveness of a home exercise programme over a rehabilitation programme [15, 22]. Patients following a house exercise programme achieved a significantly greater improvement in grip strength and scope of wrist extension and bending [22]. Evidence from one of the tests showed that introduction of the exercise process supervised by an occupational therapist during immobilisation after a DRF significantly improved the dexterity of the thumb and other fingers. Research conducted by Kuo et al. [30] did not show additional benefits in the scope of arm strength and finger dexterity as well as functional results during immobilisation or another time after removing the stabiliser.
In tests conducted by Öken et al. [24], a group of patients participating in rehabilitation conducted by a qualified therapist achieved a significant improvement of ROM results (wrist bending and extension, forearm supination) as well as hand grip and pincer grip strength, and a significant reduction of swelling, whereas the group participating in the home exercise programme achieved a significant improvement in wrist bending and radioulnar deviation.
Research conducted by Valdes et al. [16] indicated a lack of significant differences between the groups in the final PRWE, scope of active wrist and forearm motion, pain, and grip strength. However, both groups experienced an improvement of all the measures [16]. Summary of results is presented in table 3.
Summary of results
| Trial | Effectiveness |
|---|---|
| Bruder et al. (2016) | 0 |
| Filipova et al. (2015) | + |
| Kay et al. (2008) | + |
| Krischak et al. (2009) | - |
| Kuo et al. (2013) | 0 |
| Mitsukane et al. (2015) | 0 |
| Öken et al. (2011) | + |
| Sen et al. (2014) | - |
| Souer et al. (2011) | 0 |
| Valdes et al. (2015) | 0 |
+ the study reported strong evidence that therapy was effective
0 the study did no report significant difference
- the study reported that therapy was less effective than home exercises program or other programs
Analysis of published controlled trials did not yield clear evidence to show the benefits of occupational therapy instead of or in addition to other forms of patient rehabilitation after a distal radius fracture. In their research, Oken et al. [24] proved that home exercise programme after a DRF is less efficient then supervised rehabilitation. Nielsen et al. [28] recognised the efficacy of OT, if it is conducted within a year from the injury. Sen et al. [15] and Souer et al. [29] showed that occupational therapy is comparatively effective to patients exercising on their own in improving hand ability. Filipova et al. [28] showed that a combination of occupational therapy and physical therapy in the rehabilitation process benefit patients’ recovery. Kuo et al. [30] did not show any additional benefits of introducing OT for DRF patients. It was shown that patients without complications benefit equally from the advice programme and home exercises, as well as from therapy supervised by a therapist [16].
Besides individual therapeutic interventions adapted to the patient’s needs, a therapist may participate in creating and implementing home exercise programmes, as well as to conduct individual consultations for patients with fractures. Exercise programmes and consultations are aimed at speeding up the recovery process and maximising the achieved results. Sen [15] emphasises that during the consultations, the patient should be informed on the details of the exercise programme and receive an explanation that the treatment may be successful only if the patient performs it in accordance with the therapist’s instructions and emphasise that the basis for achieving therapy goals is confidence in the treatment.
Filipova et al. [28] claim that patient education and training is also of crucial importance and differentiate between the areas of work of occupational therapists and physiotherapists. The former mainly educates the patient in the scope of performing functional tasks and defined daily activities, and the latter, in movement scope exercises [24]. Due to the age bracket of patients suffering from distal radius fractures most often (the elderly), it would seem that obtaining the maximum scope of movement is a secondary goal to enabling self-reliance and a return to normal day-to-day functioning. By working with the patient on function, the occupational therapist also makes use of exercises to increase ROM necessary to perform functional tasks.
In addition to working on movement disorders, the occupational therapist also influences how the patients perceive their own disability, which will allow for an optimal reflection of recovery. Research done by Kay et al. [23] showcased that 13 persons from the control group (46%) who received no rehabilitation provided information about concerns in connection with lack of advice or guidelines provided during recovery. In comparison to the experimental group, 20 participants (71%) indicated a beneficial effect of advice and exercise provided by the physiotherapist [15]. Research may also indicate that the results of the experimental group were also influenced by psychological factors such as reduction of fear and anxiety connected with using the broken limb. Occupational therapy conducted in the form of consultations after a DRF allows for an explanation of all the possibilities and limitations in using the limb in day-to-day activities.
A distal radius fracture oftentimes results in complications, and the criteria for disorders are not always possible to determine and eliminate. In case of complications, the most important thing is an early diagnosis that enables appropriate action to be taken. Kay et al. [23] indicate that diagnosing many complications would be overlooked or delayed if not for the test protocol provided by the therapist.
Research by Valdes et al. [16] indicated that the most common complication after a fracture is CSPS / complex regional pain syndrome/, however, patients with soft tissue damage, swelling, or concomitant diseases also require increased supervision during treatment in order to maximise their results. Filipova et al. [28] suggest that adding an intervention to occupational therapy is recommended for persons with significantly decreased grip strength after cast removal. Research by Valdes [16] and MacDerimd [24] confirms that patients with complications benefit from clinical therapy. Kay et al. [23] indicate that persons after DRF should routinely be directed to a therapist in order to receive a set of exercises and enable early detection of complications.
Occupational therapy for patients with DRF may be conducted in the form of advice, consultations, or a supervised therapeutic process. Nielsen and [33] emphasise that in Denmark, DRF patients are directed to an occupational therapist by a surgeon, for a single consultation or a prolonged rehabilitation, depending on their needs. Case-Smith [25] acknowledged that “arm rehabilitation includes both outpatient services and a recommended home exercise programme” (Case-Smith J., 2003). The attached occupational therapy efficacy assessment confirms this thesis.
Analysis of the literature failed to indicate clear evidence for occupational therapy efficacy in the rehabilitation period of patients with DRFs. However, research demonstrated a necessity to introduce an intervention conducted by an occupational therapist with patients in danger of complications or those who already suffer from such complications.
The analysis emphasised the importance of the moment of occupational therapy introduction in relation to the time of injury. Aydog et al. [15] determined that patients should undergo rehabilitation shortly after treatment in order to improve the function of the arm, elbow and radiocarpal joints, as it will prevent complications. Efficacy analysis indicated a variance in timing of occupational therapy inclusion in the patient rehabilitation process. Six researchers suggested that this form of therapy should be included during the immobilisation period, and three postulated that it should be included after cast removal.
All of the presented research has weak statistical capacity, which hinders translating the results into the general population of DRF patients. An additional factor hindering result translation to the entire group of patients are the exclusion criteria. Without a doubt, subsequent research should include persons with bilateral wrist fractures, persons who suffered from previous DRFs of the same limb, persons with concomitant diseases and complications.
Analysis of literature on the effectiveness of OT during rehabilitation of patients with distal radius fractures indicates that this topic is rarely the object of scientific research. Considering how significant they are for the patients’ health and quality of life, further research is required. It should include a larger sample, consider an earlier introduction of an occupational therapy intervention in the recovery process, and perform long term measurements.
Analysis of literature on occupational therapy with DRF patients indicated no research on using detailed methods of working with the patient. A review of literature indicated a lack of protocols from the conducted therapeutic programmes in conducted tests that would compare the efficacy of methods for recovering the functions from before the injury. In case of DRF treatment, no standardised treatment rehabilitation programme exists, therefore it seems warranted to publish protocols on the conducted activities in order to determine the most efficient activities.
The inclusion of occupational therapy to the rehabilitation process (advice, consultations, exercises or supervised therapy process) leads to better results in patients after DRF. There is no clear evidence showing the benefits of occupational therapy performed instead of or in addition to other forms of patient rehabilitation after DRF.