
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disorder, which is characterized by persistent respiratory symptoms and airflow limitations due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases [1]. Dyspnea and cough are the initial common symptoms that reduce physical activity, load-carrying ability, and quality of life.
COPD is a chronic disease that involves high-priced treatment and management [2], 45–75% of which may be associated with exacerbation [3]. Modern COPD therapy is aimed at the reduction of the severity of symptoms, prevention of the development of relapses of exacerbation, maintenance of the optimal functioning of the respiratory system, and improving the quality of life [1].
One of the most critical deterrents to successful COPD treatment is a patient’s low adherence to therapy, which is primarily due to the low subjective evaluation of medical care outcomes and, as a result, false conclusions on the efficiency of treatment. Other reasons for low motivation to adhere to the prescribed treatment are low patient’s awareness of disease patterns, the lack of understanding of the need for long, often lifelong, therapy, the lack of knowledge on the prognosis in case of failure to receive treatment, the mechanisms of action of the prescribed medicine, the differences between the background and symptomatic therapy, as well as the fear of the occurrence of side effects, dependence on medications, high cost of treatment, patient’s unwillingness to materially change his/her lifestyle (for example, quit smoking) [4]. In other words, treatment, rehabilitation, living a healthy lifestyle, and following recommendations for self-management require a patient’s high motivation and self-organization.
It has been demonstrated that strategies for comprehensive pulmonary rehabilitation are beneficial in solving the abovementioned issues.
The following definition of pulmonary rehabilitation was defined in a joint official statement by the American Thoracic Society (ATS) and the European Respiratory Society (ERS) for the year 2013: “… a comprehensive intervention based on a thorough patient assessment followed by subject-tailored therapies that include, but are not limited to, exercise training, education, and behavior change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors” [5].
The advantages of pulmonary rehabilitation of individuals with COPD has been clearly demonstrated in the literature and need no further confirmation [6]. However, the search for optimal educational programs, ways of implementation and evaluation of their effectiveness, the introduction of strategies for the formation of knowledge, skills, and competencies, as well as the development of patient’s self-management are still critical and relevant.
The purpose of our study is to analyze and find effective strategies that could be implemented to enhance the effectiveness of the educational component in the rehabilitation of patients with COPD.
The search has been conducted on a resource of the National Center for Biotechnology Information, in the USA (PubMed). To identify all the descriptors needed for a comprehensive search, we consulted Medical Subject Headings (MeSH). The keyword combination was “COPD,” “Chronic obstructive pulmonary disease,” “Pulmonary Disease Chronic Obstructive,” “Organization and administration,” “Prevention and control,” “Rehabilitation,” “Therapy,” “Education,” “Educational,” “Knowledge,” “Informatisation” with selective Boolean operators “AND” and “OR.”
The following are the criteria for publication selection: studies pertaining solely to patients with COPD (1), papers published within the past five years (April 2014 – April 2019) (2), availability of the full text in English (3), the studies related to the level of awareness and familiarity among patients with the primary disease (COPD) (4), publications concerned with the importance, specific content of educational programs, their ways of implementation, and effectiveness (5), papers were related to self-management of patients with COPD.
Exclusionary criteria: protocols with incomplete clinical studies (a comment, an editorial, case report, clinical trial, a letter, a protocol) (1), papers related to the training of the staff involved in treatment/rehabilitation of patients with COPD and further evaluation of their level of awareness (2) or to other respiratory system diseases or if a patient was simultaneously diagnosed with COPD and other illness (3), publications on planning and implementation of activities related to medical treatment (4).
In order to ensure the accuracy of the review, both authors have independently developed a summary of the included studies. The exactness of these studies has been checked using a checklist with five questions: is this a detailed description of the participants? (1); is this an accurate description of educational programs, their ways of implementation? (2); is this a proper summary of the educational program? (3); is this a detailed description of outcomes? (4); is this a logical summary of the research methodology? (5).
Co-authors analyzed the articles by the checklist, edited the summary, and improved its accuracy. The results have been discussed, agreed, and used for the creation of tables.
All the search results are relevant as of April 2019.
Figure 1 illustrates the 3-phase screening approach and the number of articles included at each stage. From the initial database searches, 2487 unique papers were identified, 895 were retrieved for full-text evaluation, 39 of those were included for further data extraction. Publications selected for analysis based on the main content have been grouped into five categories; most articles have been focused on the self-management strategy. Among them, there are influence of the level of awareness on various aspects of health and life – 6 publications (1), education on specific issues related to COPD – 5 publications (2), provision of educational services and assessing their effectiveness – 3 publications (3), content and implementation of the educational component within the integrated pulmonary rehabilitation – 7 publications (4), self-management strategies – 18 publications (5).
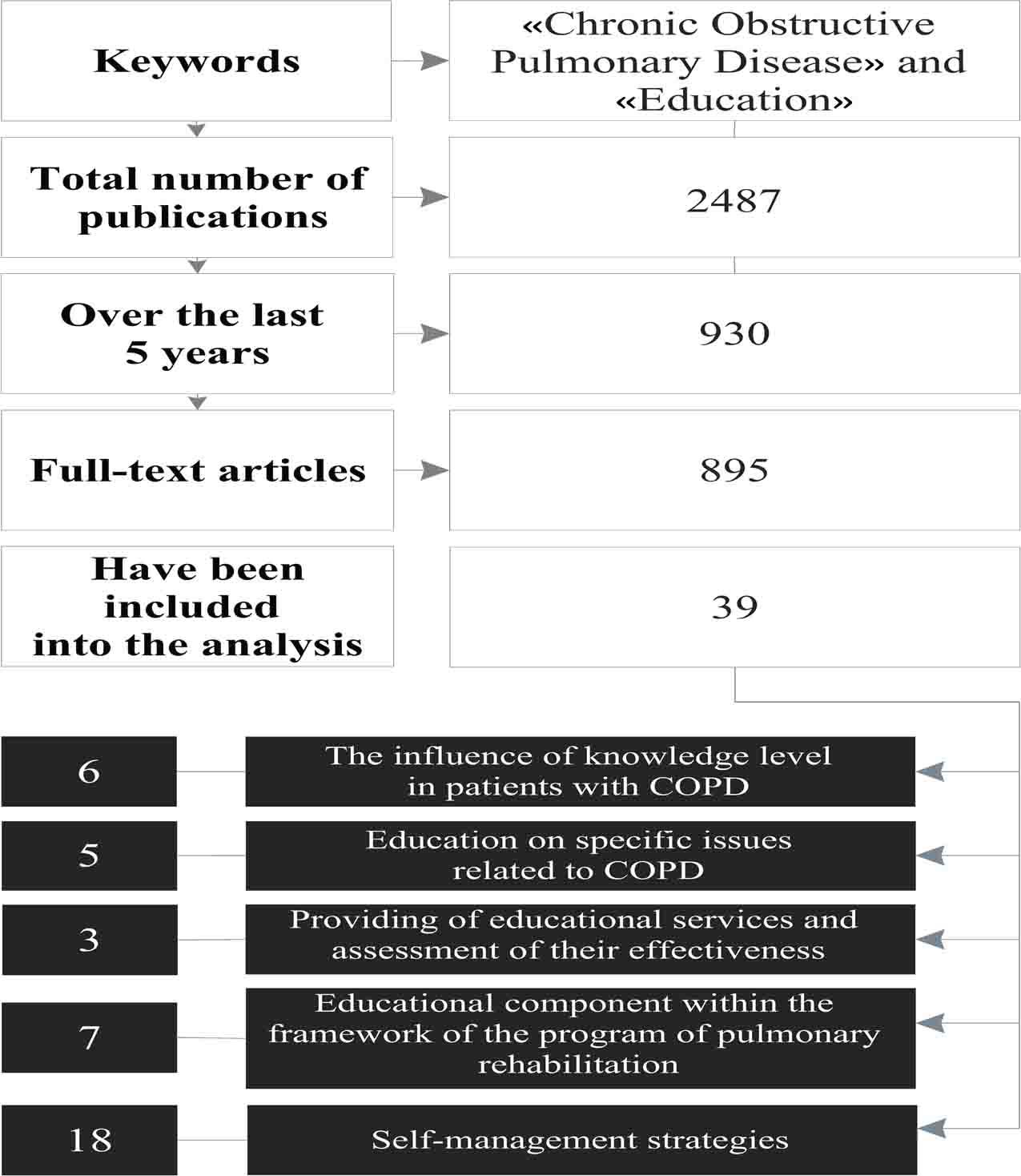
The phases of screening approach and the number of articles included at each stage
The division of articles into separate groups was, in some cases, conditional since the study could have been conducted in two or more areas. In this case, the publication has been attributed to the selected group considering the main objective of the study.
For the successful treatment and improvement of the quality of life of patients with COPD it is essential to have a high level of specialized knowledge about this disease, especially about the way disease affects the well-being and various aspects of life (Table 1). The ability of patients with COPD to independently influence the course of the disease, while maintaining their well-being at a relatively stable level depends on the level of disease awareness. The level of awareness of patients with COPD of the nature, course, and effects of the disease affects various aspects of life. In particular, there is a strong positive correlation between the level of awareness of patients with COPD and the level of their self-management [7].
Analysis of articles devoted to the impact of knowledge level on various aspects of health and life
| No. | Authors, year, country | Type of research / goal of research | Number of participants ansd sex; age (years old) | Research methods | The content of the educational program or research results |
|---|---|---|---|---|---|
| 1 | Hua Yang et al., 2019, China [7] | Observation/Determination of the relationship between the knowledge level on the disease and the level of self-management | 246♂ + 100♀; 44–86 | COPD-Q and CSMS questionnaires | It was found that the knowledge level on COPD correlates with the level of self-management behavior. |
| 2 | Abdulsalim S. et al., 2018, India [9] | Randomized controlled clinical study/Evaluating the effectiveness of the pharmacist’s clinical intervention on the patient’s commitment to treatment | 194♂ + 12♀; 61.1. (8.4)*–60.6 (7.9) | MAQ questionnaire | Consultation sessions (15–20 min) and information leaflets on the following essential indications: adhere to medical therapy, measure out in doses and take medication on time, need to quit smoking, do exercises, use inhalers properly and detect illness rapidly |
| 3 | Collinsworth A.W. et al., 2018, USA [8] | Prospective randomized pilot study/Evaluate the feasibility of the developed educational program | 128♂ + 180♀;44–86; 70.9 (12.5)– 70.0 (11.9) | Patient Activation Measure and CAT questionnaires | An educational program is aimed at obtaining basic knowledge about COPD and participation in the planning of self-management activities (15–30 min) and planned telephone conversations. Participation in planning in collaboration with patients provided a common choice of patient’s most significant on their opinion strategies for preserving health and preventing exacerbations. |
| 4 | Schüz N. et al., 2015, Australia [11] | Randomized controlled study/Studying the effect of anxiety and depression in patients on the effectiveness of a rehabilitation program | 182; ND, >45 | Questionnaires by HADS, Partners in Health Scale; axonometry | 16 conversations over the phone for 12 months. The topics of conversations concerned 5 components of self-management. |
| 5 | Zhang Q. et al., 2014, China [10] | Cross-sectional study/Study the knowledge of COPD as a risk factor for anxiety and/or depression in patients with COPD, links between levels of knowledge, functionality, and quality of life | 327♂ + 32♀; 65.64 (7.60) | Dyspnea scale mMRC; HADS, CAT, BCKQ; 6MWD questionnaires | A higher score has been correlated by HADS with a lower COPD level. Critical issues of COPD that are a risk factor for anxiety and/or depression in patients with COPD are epidemiology, and infection |
| 6 | Nakken N. et al., 2017, Netherlands [12] | Cross-sectional study / Comparing the knowledge level of illness in patients and their guardians | 194** 102♂ + 92♀; 66.0 (8.7) | The questionnaire with 34 statements, formulated by a multidisciplinary group of pulmonary rehabilitation | Patients and their guardians have limited knowledge of COPD and overall health status. Patients should be educated with their guardians, which will be useful in terms of improving management strategies, strengthening relationships, and organizing behavioral changes. |
Notes: COPD-Q – Chronic Obstructive Pulmonary Disease knowledge Questionnaire, CSMS – COPD Self-Management Scale, MAQ – Morisky, Green and Levine Medication Adherence Questionnaire, HADS – Hospital Anxiety and Depression Scale, mMRC – Modified Medical Research Council, CAT – COPD Assessment Test, BCKQ – Bristol COPD Knowledge Questionnaire, 6MWD – six-minute walk distance. ND – sex was not determined in the study.
– M (SD).
– the study involves patients and their guardians; the age and gender is given for patients with COPD.
One of the goals of educational programs in the field of rehabilitation is to improve the person’s adherence to therapy. Patients with COPD chose to develop such skills that will contribute to the formation and development of self-management, as well as the correction of a lifestyle (leaving off smoking) [8]. These and other educational topics have been provided within the educational program, which had been planned for each patient. Thanks to the abovementioned approach and educational program the duration from the beginning of the program until the first exacerbation was longer and had a positive impact on the health condition of the subjects, however, in general, it did not decrease the total number of hospitalizations.
Better adherence to medication therapy can be achieved by involving pharmacists in providing consultations for patients with COPD [9]. Such an approach reduces the number of intents of improper consumption of pharmaceuticals.
The level of awareness of the disease is a risk factor for the development of anxiety and depression in patients with COPD , a decrease in the quality of life, and an increase of dyspnea [10]. The level of a patient’s anxiety and depression before the educational program significantly determines its effectiveness. In particular, there has been found the positive effect of educational program on self-management on the level of awareness and the change in physical activity of patients with a low level of anxiety and depression [11]. At the same time, a higher level of anxiety and depression was associated with a lower level of physical activity after completing the educational program.
To overcome/stabilize the disease both patients with COPD and their guardians shall have the appropriate level of awareness. [12]. In general, the researchers have not found any significant differences between the level of awareness of the patients and their representatives. Moreover, the responses of patients who had previously participated in the program of pulmonary rehabilitation, persons with better cognitive function, younger patients, and patients with a higher level of education, as well as patients with previously diagnosed COPD appeared to be more accurate.
The syllabus for COPD patients includes a wide range of topics. Some of them are theoretical, while others are combined with practical skills. Among the selected publications there are studies devoted to the significance and peculiarities of studying particular educational topics, mainly the use of inhalation devices, the correct use of which is an essential basis for the effective treatment of COPD patients (Table 2). The studies confirmed a high rate of inappropriate use of inhalers among COPD patients (40–100%) [13–15], even after specialized training or long-term (on average 9 years) usage of the device.
The results of selected educational issues related to COPD
| No. | Authors, year, country | Type of research/aim of research | Number of participants and sex; age (years old) | Research methods | Description of educational methodology |
|---|---|---|---|---|---|
| 1 | Windisch W. et al., 2018, Germany [13] | Randomized controlled trial/Compare the effectiveness of learning with the use of web video with individual instructions for the correct inhalation technique | 74♂ + 78♀; 66.6 (7.7)*–68.2 (9.1) | Checklists of the correct inhalation technique (https://www.atemwegsliga.de) | Individual instructions provided by the doctor. Web videos provided by Deutsche Atemwegsliga demonstrating proper inhalation techniques |
| 2 | Purohit A.N. et al., 2017, India [15] | Prospective, continuous, interventional, comparative study/Evaluate the impact of such training activities as a demonstration of a researcher’s technique and information sheets on the use of a metered-dose inhalers (MDI) | 65, ND; 49.47 (1.95)–44.70 (2.19) | WHO Guidebook | Demonstration of the technique of using the inhaler, cards with a graphic representation of the correct technique of using an inhalation device |
| 3 | Beatty C.R. et al., 2017, USA [14] | Prospective experimental study/To investigate the influence of the level of medical literacy on inhalation technique | 120, ND; 18–89 | Medical literacy questionnaire – REALM-SF. Checklist for a correct use of an inhaler | Specially designed handout material that takes into account the specific types of inhalers and the level of medical literacy, a standard handout that is used in hospitals |
| 4 | Takaku Y. et al., 2017, Japan [17] | Prospective study/Evaluate the number of instructions needed to minimize mistakes when using inhalers of different types | 74♂ + 7♀; 72 (7) | Checklists for assessing the correct use of the inhaler | Repetitive testing of practical skills, evaluation of the effectiveness of the acquired knowledge (2-5 times with intervals from 2 weeks up to 1 month until the maximum possible positive result is achieved), instructions |
| 5 | Bouwmeester C. et al., 2015, USA [16] | Observation/Assess the patient’s ability to demonstrate and maintain appropriate methods of administering inhaled medication after training provided by a pharmacist | 36, ND; 81 (10.05) | Hickey’s Pharmacies Inhaler Technique assessment | Training session with a pharmacist on the use of an inhaler, evaluation of its performance |
Notes: MDI – Metered Dose Inhaler, REALM-SF – Short Form of Rapid Assessment of Adult Literacy in Medicine.
– M (SD).
ND – sex was not determined in the study.
Among the methods of the proposed work with patients, specialists have suggested as follows: specially developed handout material [14], which considers the level of awareness of a patient (including a very low one) of the disease, video lectures, demonstration of the use of inhaler techniques, direct instructions given by pharmacists, etc. [16]. Individual methods of work appeared to be the most successful ones (practical training sessions with medical specialists, and individual instructions), but video demonstration has also appeared to be effective. Even one training session with a pharmacist can significantly improve the quality of use of inhalation devices and save the result of training for 4–6 weeks [16]. However, evaluating the number of training sessions required to minimize mistakes in the use of inhalations, Takaku Y. et al. found that many specialists (pharmacists) misplaced steps and failed to demonstrate to their patients appropriate techniques of using the inhaler [17]. In order to achieve the maximum positive effect and to develop the skills of using one model of the inhaler, a patient needs at least three sessions of instructions. However, some patients may continue wrong inhalations even after repeated instructions that sometimes depend on physical constraints and the inability to use the device properly [17]. In such cases, it is recommended that the device is changed to an easier one.
Provision and effectiveness of educational services for people with COPD
| No | Authors, year | Type of research / goal of research | Number of participants and sex; age (years old)/subject of study | Research methods | Organization of educational services or research findings |
|---|---|---|---|---|---|
| 1 | Ward S., Sewell L., Singh S., 2018, UK [20] | Comparative follow-up study/Evaluate the quality of providing educational services in the form of a DVD presentation | 64♂ + 59♀; 68.00 (10.04)*–71.26 (10.19) | BCKQ questionnaire | Conducted by: members of a multidisciplinary team (pulmonologist, occupational therapist, nurse of respiratory medicine, physical therapist, psychologist, dietician, and pharmacist). |
| 2 | Bhattacharyya P. et al., 2018, India [19] | Clinical study/Evaluate the effectiveness of self-study and intensive one-session training under the guidance of specialists based on a simple training program for patients | 62♂ + 28♀; 62 (9)–71.26 (10.19) | CAT | As part of one-day training camp. Themes: information on COPD and the importance of smoking cessation, pharmaceutical information, the correct use of inhaled medicines, the importance of treatment for COPD-related diseases, proper and appropriate food and hygienic interventions (including bronchial hygiene), general exercises and exercises with particular emphasis on walking and breathing |
| 3. | Stellefson M. et al., 2014 [21] | Heuristic evaluation/Analyze the content of video materials related to COPD and located on YouTube | 223 video materials | 3 experts who have experience in web design and health technology have estimated the functionality of the prototype of the COPDFlix Social Resource Center | The following main recommendations were given for eliminating barriers in using the website: use a simpler language for potential website users, include website map and highlight active hyperlinked items |
Notes: BCKQ – Bristol COPD Knowledge Questionnaire; CAT – COPD Assessment Test.
– M (SD).
A face-to-face meeting at least once a week for 6–8 weeks and simultaneous provision of printed educational materials are the classical approach towards the implementation of the educational component [18]. It requires territorial accessibility of institutions that provide such services for patients, relevant professionals, the patient’s ability to attend training sessions and financial support. Accordingly, in order for patients with COPD to get more specialized education and to reduce the economic burden, alternative educational ways are being sought. An intensive, one-sessional training within a one-day training camp, which has a statistically proven efficiency, may be an economically sound resolution. [19].
Educational services may also be provided both in the form of lectures and using digital media (in particular, DVDs) [20]. A comparison of these two forms of training showed no significant differences in the awareness of patients who used these techniques. An increase in viewing online medical information among adults with chronic diseases, as well as the possibility of usage of information and communications technologies, increases patient’s access to learning. YouTube™ (www.youtube.com), one of the most popular social websites, is often used to exchange some educational materials for patients with chronic diseases. Assessing the content and quality of 223 video tutorials on YouTube, it has been revealed that about half of the videos cover the topic of “Drug Management” (50.7%), while “Leaving off Smoking” has been highlighted in 17.9% of the analyzed videos, “Physical activity” – 17.5%, “Everyday affairs” – 16.6%, “Infection control” – 11.7%, “Respiratory training” only 9.8%, “Nutrition” and “Stress management/energy saving” – less than 5% of the videos [21]. The promotion of educational materials on YouTube has great potential; however, the quality and the content of analyzed and available videos were quite low, and their total number is small if compared with the amount of video material related to other chronic diseases.
Education is one of the compulsory components of pulmonary rehabilitation programs [22–23], and most of them have training sessions for patients with COPD . Researches strive to find the most relevant topics, duration, number of sessions, and ways of providing educational material (Table 4).
Publications devoted to the educational component within the framework of a pulmonary rehabilitation program
| No. | Authors, year, country* | Type of research/goal of research | Number of participants and sex; age (years old)/subjects for study | Number of participants / Research methods | Content and organization of the educational component or research findings |
|---|---|---|---|---|---|
| 1 | Gardener A. C. et al., 2018 [25] | A systematic review of literature/Determine the full range of needs for the support of patients with COPD | 31 articles | The review was conducted in accordance with the PRISMA recommendations, publications from January 1996 to February 2016 were considered | a complex set of areas of necessary support for patients with COPD has been identified according to the patients’ views |
| 2 | Chaplin E. et al., 2017, UK [29] | Randomized controlled trial/Evaluate whether web-based pulmonary rehabilitation programs can be an alternative to conventional programs | 103 participants: 71♂ + 32♀; 66.1 (8.1)**–66.4 (10.1) | Physical performance has been assessed (ISWT and ESWT), chronic respiratory self-esteem from (CRQ-SR), anxiety and depression scale (HADS), evaluation of COPD manifestations (CAT), PR Adapted self-efficacy index (PRAISE), evaluation of COPD knowledge (BCKQ), quality of life(EQ-5D-5L), patient cost questionnaire | Duration of the program of pulmonary rehabilitation 6–8 weeks. |
| 3 | Garvey C. et al., 2018 [30] | Review/Describe the options for a home-based pulmonary rehabilitation program | Electronic databases MEDLINE, CINAHL, EMBASE, AMED, PubMed, Cochrane, PEDro | The search strategy applied in MEDLINE was adapted for other databases | The need for personalized, affordable, and effective pulmonary rehabilitation at COPD will stimulate the development of devices, platforms, and programs in order to meet these essential needs and gaps in treatment. |
| 4 | Wilson A.M. et al., 2015, UK [24] | Randomized controlled trial/Rate the support program after the completion of pulmonary rehabilitation | 148 participants: 91♂ + 57♀; 67.3 (15.1)–69.3 (8.9) | CRQ questionnaire, clinical test ESWT, EQ5D questionnaires, HADS, a diary of physical activity | The support program consisted of one session lasting 2 hours, held every 3 months, including 1 year of learning and 1 year of training |
| 5 | Kiongera G.M., Houde S.C., 2015, UK [27] | Clinical study/Evaluate the effectiveness of the in-patient program for pulmonary rehabilitation for patients with COPD in an institution of long-term care | 23 participants: 11♂ + 12♀; 68–72. | Physical performance (6MWD), dyspnea rate (Borg scale CR10), quality of life (SGRQ), satisfaction survey form | The 6–8 weeks program, which consisted of 24 series of activities. |
| 6 | Desveaux L. et al., 2015 [26] | Systematic review/To describe the international experience of providing pulmonary rehabilitation, and to compare its structure and indicators in different countries | 7 studies | The review was conducted in accordance with PRISMA recommendations, publications published before September 2013 were considered | The current availability of PR programs service less than 1.2% of individuals living with COPD across seven countries with wealthy economies |
| 7 | Marques A. et al., 2015, Portugal [28] | Randomized controlled trial/Study the effects of a family program of pulmonary rehabilitation on COPD management | 42 couples (a person with COPD and a family member): 28♂*** + 14♀; 65.9 (13.4)–68.8 (7.3) | Functional balance (“Get up and go” test), estimation of shin extensor’s force, quality of life (SGRQ) | Duration of the program of pulmonary rehabilitation – 12 weeks. The program consisted of training, psychological support, and education, conducted in primary care centers. Family members attended sessions of psychological support and training along with patients with COPD |
Notes: ISWT – Incremental Shuttle Walking Test; ESWT – Endurance Shuttle Walk Test; CRQ-SR – self-reported Chronic Respiratory Questionnaire; HADS – Hospital Anxiety and Depression Scale; CAT – COPD Assessment Test, PRAISE – The Pulmonary Rehabilitation Adapted Index of Self-Efficacy; BCKQ – Bristol COPD Knowledge Questionnaire; EQ-5D-5L – 5-level EuroQol 5-dimensional questionnaire; CRQ – Chronic Respiratory Disease Questionnaire; SGRQ – St. George’s Respiratory Questionnaire; 6MWD – six-minute walk distance.
– if the subject of study is articles, the information about country was not given;
– M (SD);
– information about participants with COPD.
The positive effect of pulmonary rehabilitation programs decreases in the course of time, making it important to find out ways for maintaining the achieved results. One of such approaches has been studied by Wilson A. M. et al. [24], who proposed a support program for patients with COPD , who had already completed pulmonary rehabilitation. Unfortunately, this program has appeared to be ineffective for maintaining or improving the quality of life and ability to withstand the physical load, reducing the level of anxiety and depression, as well as positive effects on dyspnea and daily physical activity achieved after the completion of the pulmonary rehabilitation program. Half of the time of the support program has been devoted to the educational component. Three-hour training sessions (in the 3d, 6th, and 9th month) were devoted to the following topics:
Healthy eating, the importance of physical training, prevention of exacerbations, and action plan in case of any of them, leaving off smoking.
Overcoming dyspnea, consideration of different workout strategies, breaking barriers on the way to physical activity.
Psychological issues that arise during the development of chronic disease, their possible solutions, mastering of relaxation techniques, and assistance for those who care for patients with COPD .
On the basis of a systematic review of publication from January 1996 to February 2016, Gardener A. C. et al. identified 13 areas that are important for patients with COPD and in which they require additional support [25].
In general, the practice of providing pulmonary rehabilitation in different countries involves specific educational programs [26]. Basically, there are about 38 educational topics for patients with COPD, and “Medicines” and “Relaxation” are considered in most cases.
There are pulmonary rehabilitation programs that include the provision of educational sessions for inpatients at long-stay institutions twice per week for six weeks [27], being held by pulmonologists, physical therapists and occupational therapist.
The family-based program of pulmonary rehabilitation had the same positive effects as usual ones focused on the ability to withstand the physical load, increase the strength of quadriceps, and functional balance [28]. It is suggested to attract family members to educational events and psychological support events. It is recommended to use didactic methods (discussion, role-playing games, homework, and brainstorming) during weekly training held by a multidisciplinary team consisting of a physical therapist, a gerontologist, a psychologist, a nurse, and a doctor. Such a version of the program is of great benefit to the family and helps its members to have a better insight into the disease and better control COPD while improving family relations.
A comparison of the usual pulmonary rehabilitation program with a web-based program revealed that 38% of the subjects prefer a web-version [29], 23.5% said they required a usual program, while others did not have preferences or refused rehabilitation at all. Assessment before the start of a web-based program was carried out in order to select educational material by the topics with low level of awareness. These studies have shown that interactive web-based programs can be an acceptable alternative to the usual pulmonary rehabilitation programs.
Possibilities and methods for organizing pulmonary rehabilitation in a remote mode are of interest to patients, healthcare personnel, and researchers. Garvey C. et al. [30] attempted to systematize data and analyze options for home-based pulmonary rehabilitation programs. Special attention is paid to the educational component of home-based pulmonary rehabilitation programs, which focuses primarily on improving the level of self-management. Based on the official statement of the American Thoracic Society and the European Respiratory Society, the following main educational topics on self-management are recommended [30]:
Systemic anatomy and physiology of the lungs.
Pathophysiology of chronic respiratory diseases.
Communication with a doctor.
Interpretation of medical screening.
Breathing techniques.
Airway clearance techniques (ACTs).
The role and justification for the need of treatment, in particular, oxygen therapy.
Effective use of respiratory devices.
Advantages of workouts and physical loading.
Energy saving during daily activities.
Healthy eating.
Avoiding provocative factors.
Early recognition and treatment of exacerbations.
Leisure.
Managing COPD.
A significant amount of scientific research in the field of educational services for patients with COPD is focused on the strategy of self-management. Self-management support interventions for patients with COPD are “structured but personalized and often multi-component interventions, with goals of motivating, engaging and assisting the participants to positively adapt their behavior(s) and develop skills to manage their disease better” [31].
The self-management concept includes self-monitoring, symptom management, management of emotional, psychosocial, and functional consequences of the disease, and collaboration with family, community, and healthcare professionals [32].
Interventions for supporting self-management are primarily based on informing patients and the formation of individual goals and strategies, focusing on motivation, achievements encouraging, and mental health [33].
Although at first sight they might look similar, the components of patient`s education and self-management education are really different [34]:
- –
self-management education is based on the person’s commitment and active involvement;
- –
issues, purpose, and tasks are to be set by patients, not by healthcare specialists;
- –
provided information and skills are problem-oriented, not nosological;
- –
it is suggested that behavior changes as a result of the increase in the level of self-efficacy regarding the ability to participate in self-management, rather than as a result of raising the level of awareness.
In general, self-management education strategy is based on the promotion of disease control and its consequences [35]. The educational component itself in pulmonary rehabilitation programs is inefficient, it is necessary to change behavior, in particular acquire self-care skills [36]. Moreover, Sohanpal R. et al. [37] state that education is a part of the self-management support component.
In the short term, self-management education can ensure improved health [38] and functional level, reduce the hospital stay, facilitate the development of planning, organization and control skills in patients with COPD , and improve management [39]. Thus, the study of the effectiveness of the relevant programs has revealed their positive influence on some areas of self-management (“Constructive attitudes and approaches,” “Skills and technique acquisition,” “Self-monitoring and insight”) [33], improving life quality [40, 41], awareness of the disease [42], prolongation of the remission period [40], reducing hospital stay and number of visits to a doctor [43, 44]. In a cohort study by Khan A. et al. [45], patients with a developed self-management plan more often attended training courses or consultations on physical activity, they obtained a higher level of awareness of COPD and better adherence to treatment. The optimal variant for implementation of self-management programs, their substantive content, and maintaining of self-management and self-monitoring skills, as well as feedback from healthcare professionals, can be considered as an introduction of the practice of online diary [46]. Patients with COPD who used such diaries were able to control their own lives and their disease. The influence of self-management program on the quality of life, physical performance or psycho-emotional state is still a controversial issue, its effectiveness may also be unsatisfactory, and the introduction of specific programs may cause certain barriers for both patients and those engaged into treatment/rehabilitation [47].
The main goal and related tasks addressed by the strategy of self-management [48]:
Health behaviors:
- –
leaving off smoking (as necessary);
- –
increasing physical activity;
- –
medical treatment (devotion and adequate inhalation technique).
- –
Disease management:
- –
avoidance of deteriorating factors (smoking, dust);
- –
dyspnea control (taking the appropriate medications, breathing through the pursed lips);
- –
use of energy saving methods (e.g., choosing the pace of walking);
- –
formation of exacerbation management strategies (a written action plan that includes key components to make exacerbation management easier);
- –
use stress management strategies (exercises for relaxation).
- –
There have been highlighted more different categories of self-care behaviors and strategies that can be used by patients with COPD [49]:
Self-care for the prevention, control, and management of COPD and respiratory symptoms.
Self-care for the prevention, control, and management in everyday activities.
Self-care for addressing trouble sleeping.
Self-care for exacerbation control and management.
Self-care for emotional-distress management.
Self-care for managing social life changes.
Contact with healthcare institutions.
Acquisition of self-care knowledge and skills.
The educational component is an indispensable component of all and any medical and rehabilitation measures [18]. Without raising the level of patient’s awareness of all COPD aspects, it is difficult to achieve a sufficient level of motivation to follow medical recommendations for treatment, physical therapy, behavioral changes in nutrition, physical activity, and daily routine [4].
It might look easy to provide specific knowledge on the disease and various aspects of life for patients with COPD , but it requires thorough planning [25], assessment, preparation of study and handout materials, subsequent support and access to educational resources (Figure 2).
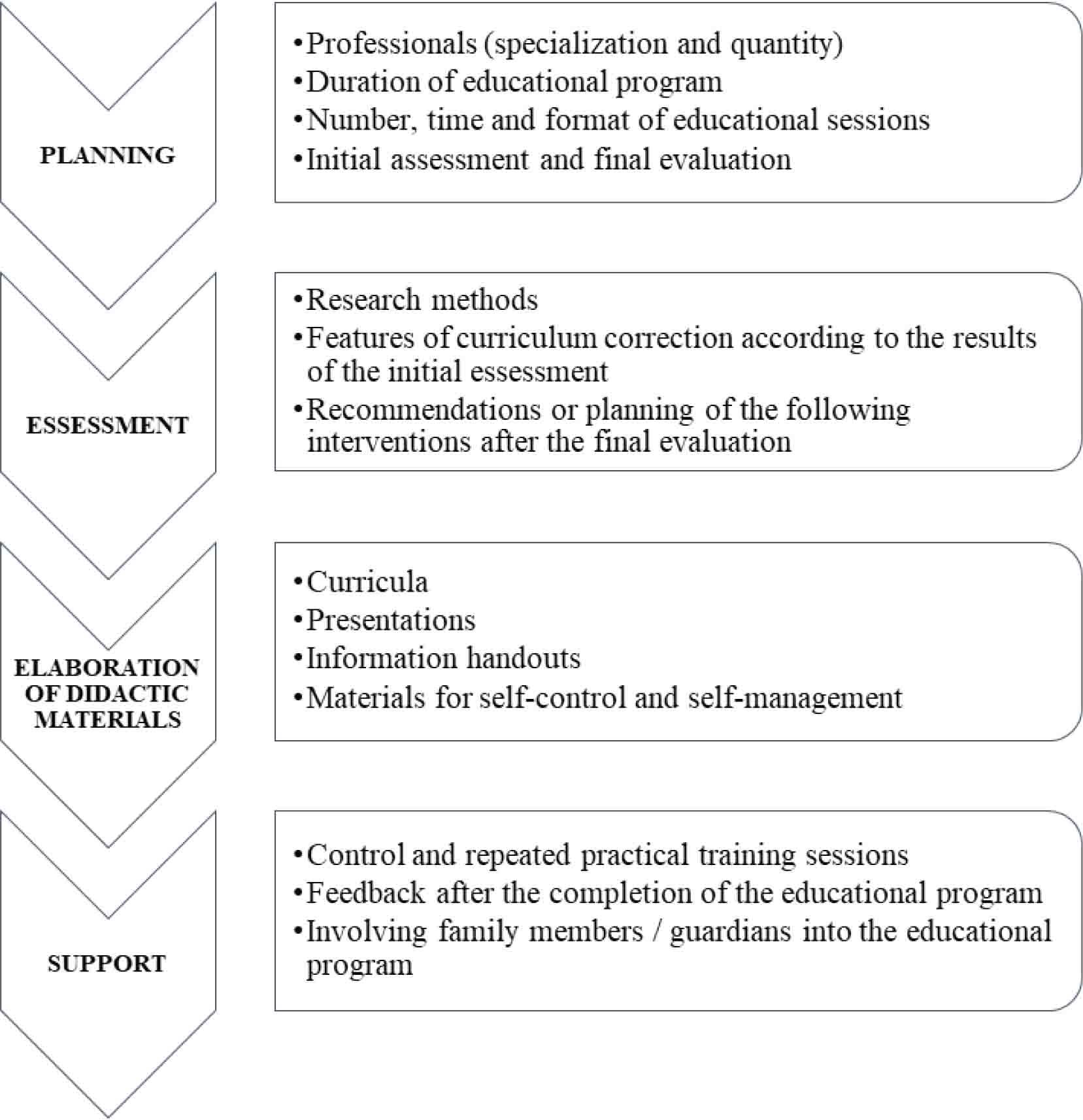
Stages and components of the educational program for patients with COPD
Based on already existing practice, it is advisable to review the recommendations which consider modern researches on the implementation of the educational component in the treatment and rehabilitation of patients with COPD (Table 5).
Recommendations on the implementation of the educational component in pulmonary rehabilitation programs based on the results of modern scientific researches
| No. | Recommendation | Implementation | Goal | |
|---|---|---|---|---|
| 1 | Attract professionals of different specialties for elaborating and implementing educational programs | Specialists |
| the involvement of professionals in certain specialties will enable the educational materials to be presented as efficiently as possible, and individual characteristics of patients with COPD should be considered |
| 2 | Additionally assess the knowledge level, self-management behavior, and psycho-emotional state before the implementation of the educational component of rehabilitation | Assessment |
| Definition of the initial level, elaboration of topics according to relevance for inclusion in the curriculum, the extraction of unnecessary or in-depth information from the curriculum, solving the issue with the method of training and providing training materials |
| 3 | Choose the most convenient for the patient methods and organization of training and ways to provide training materials | Educational methods |
| Cost-effective, result-oriented learning that reaches |
| Ways of providing learning materials |
| |||
| 4 | Provide patients with the opportunity to maintain the achieved level upon completion of the educational program | Methods |
| Achieving the maximum effect and availability of learning for each patient |
| 5 | Involve patients in choosing and planning strategies | Occurs at the stage of initial assessment and definition of curriculum purpose and objectives | Increase understanding and motivation, and patient’s active participation in the treatment, pulmonary rehabilitation, and self-management | |
| 6 | Operate the maximum amount of educational topics for a flexible choice according to patients’ needs | It is expedient to choose the subjects of studies after determining the knowledge level, and take into consideration the patient’s vision of the sphere where he/she is most in need of information | To improve the individual approach to the implementation of an educational component of a pulmonary rehabilitation program | |
| 7 | Include self-management strategy for improving efficiency | Main components |
| Increase the effectiveness of treatment and rehabilitation, prevent exacerbations, optimize financial savings |
The educational component is one of the crucial and significant parts of the pulmonary rehabilitation program [12]. The issue of accessibility and the proper level of educational services are of concern to many researchers and practitioners. A sufficient level of implementation of educational services and the professional provision of information on the given topics may be ensured by several specialists of different specialties, although a pulmonologists, physical therapists and psychologists are the key specialists [50].
Assessment and determination of the patient’s initial level of awareness, anxiety, depression [11], motivation, and peculiarities of everyday life will make it possible to consider the results while correcting the studied indicators and the educational program itself.
The search for an alternative way, except for traditional lectures, [13,21,29] and methods of providing educational services [30] for patients with COPD , and assessment of their effectiveness aims at attracting more patients to pulmonary rehabilitation programs, improving access to all components of pulmonary rehabilitation, in particular, educational ones. Thus, the choice of providing educational services through the use of traditional lectures, printed materials, videos, or online materials should be considered.
Increasing patient’s motivation, their cooperation with healthcare personnel, and active participation in the continuation of pulmonary rehabilitation programs will help to get feedback from the providers of pulmonary rehabilitation services. Once the pulmonary rehabilitation program is completed it is advisable to choose the most convenient ways of communication with patients. Such steps, along with the provision of awareness and skills in self-management, will allow the patients to monitor their condition more effectively and follow the recommendations of physicians and physical therapists more responsibly.
Having analyzed the studies it has been revealed that the issue of relationships between the effectiveness of the educational component or general rehabilitation program and the stage of COPD is poorly understood. Thus, the issue of improving the educational part, correction of frequency and duration of meeting, taking into account the phenotype or stage of COPD, remains crucial. It can be assumed that the COPD`s stage is vital for choosing the most appropriate topics to be included in the education component. In the mild stage, it is advisable to devote time to the issue of lungs’ work and functions, the benefits of exercise, healthy nutrition, active leisure, avoidance of provoking factors, and the issues of diseases management. In patients with moderate/severe COPD, it is essential to focus on breathing strategies, airway techniques, the role and justification for treatment, including oxygen therapy and effective use of respiratory devices, energy saving during daily activities, and early recognition and treatment of exacerbations. A critical issue to be considered with severe patients and their caregivers are the possible prognosis, treatment options, including non-invasive ventilation, admission to the intensive care unit, end of life.
Despite the great potential and benefits of the educational component of pulmonary rehabilitation programs, a lot of human, financial [25], organizational and intellectual resources are required for its appropriate introduction [2]. Considering modern practice of conducting and recommendations for the provision of education for patients with COPD, as well as modern technologies, will make it possible to properly implement this component in pulmonary rehabilitation programs, achieve the objectives and positive impacts.
Much attention is being paid to the study of the effective ways of implementation of the educational component in the treatment and pulmonary rehabilitation of patients with COPD . Effective educational strategies ensure long-term benefits for the patients, fewer exacerbations, better physical performance and quality of life. The correct inhaler technique is the fundamental practical skill to be learned by patients with COPD during training sessions. Based on the analyzed publications, a set of recommendations has been developed, and they should be considered when elaborating on the curriculum within the pulmonary rehabilitation for patients with COPD .
The prospect of further publications and research is a description of the educational component of pulmonary rehabilitation, evaluation of the effectiveness of the interventional program, considering practical recommendations given in this article. The educational topics will be divided into obligatory and selective parts, depending on the results of the assessment at the beginning of the pulmonary rehabilitation program, COPD`s severity and patient`s demands.