
Benign hypermobility joint syndrome is characterised by the laxity of joint capsules and ligaments, increased range of joint mobility as well as improper functioning and operation of organs and systems containing connective tissue. With regard to biomechanics, in this disorder, a safe physiological barrier shifts towards increasing joint mobility up to the anatomical barrier, at times even crossing it and showing abnormal symptoms [1–3]. Joint capsule laxity, ligament elongation, increased range of motion in peripheral and spinal joints are both the effect and cause of benign hypermobility syndrome [4].
Aside from increased joint mobility, clinical symptoms of BHJS include: joint subluxation or luxation, back pain, mild tissue damage, thin skin and joint pain [5]. Pain is often accompanied by edema, which appears mostly during increased physical activity [6].
Modified Beighton Scale is the basic scale for the assessment of BHJS [7]. Each maneuver is assessed with points on a 0-1 scale for both right and left side of a body. Diagnosis is based on the following maneuvres: passive dorsiflexion of the fifth MCP (metacarpophalangeal) joint ≥ 90°, apposition of the thumb to the forearm, hyperextension of the elbow joint ≥ 10°, hyperextension of the knee joint ≥ 10°, laying hands flat on the floor during forward flexion of the trunk while maintaining extension of knee joints. BHJS diagnosis for girls requires at least 5 points, while diagnosis for boys requires at least 4 points [8].
Increased joint mobility might be congenital as well as acquired. The latter is a result of systematic performance of exercises, such as dancing exercises [9]. Isolation movements, maintaining low center of gravity, high dance dynamics as well as leaning the trunk forward and putting the bodyweight from hindfoot to forefoot (‘collabs’) ]10] form the basis of the jazz dance technique. This technique also requires increased range of motion in certain joints, stretching of certain muscle groups and strengthening of the whole muscular system.
The purpose of this paper was the analysis of the relationship between BHJS and the occurrence of injuries among people practicing jazz dance.
On obtaining permission from Science Commission SKE 01-18/2018, trials began with 60 participants: 30 dancers (26 women and 4 men) constituting the study group and 30 people (24 women and 6 men) constituting the control group of people not engaged in professional sport or dancing. The two groups did not differ in terms of age, height, body mass and BMI (tab. 1).
Description of study and control group
| Age | Height | Body mass | BMI | |
|---|---|---|---|---|
| Study group | avg. 24.9 yrs sd. 2.1 | avg. 1.7 m sd. 0.1 | avg. 60.1 kg sd. 7.7 | avg. 20.5 sd. 1.4 |
| Control group | avg. 25 yrs sd. 3.5 | avg. 1.7 m sd. 0.1 | avg. 58.5 kg sd. 10.3 | avg. 20.2 sd. 1.8 |
| Test statistic | -0.1 | 0.6 | 0.7 | 0.7 |
| p-value | 0.2 | 0.4 | 0.1 | 0.4 |
The average span of dancing experience was 14.6±4.5 years.
In both groups, subjects engaged in supplementary physical activity. The aforementioned supplementary physical activities most often included running, swimming, gym exercises and fitness. The average time spent every week by the dancers from study group on supplementary physical activities was 4.1±2.8h, while for the control group this amounted to 2±1.4h. 20 subjects (67%) from study group worked in a sedentary job for 35.1±2.54h weekly on average. 18 subjects (60%) from control group were also employed in a sedentary job but their average weekly working hours amounted to 37.5±1.5h.
The study was conducted using a survey designed by the author. The common part of the survey for both groups consisted of basic personal details of the subjects, physical activity they engaged in, past injuries and treatment thereof, performed stabilization exercises as well as joint pain, its frequency and intensity on the VAS scale. Second part of the survey was given only to dancers (study group) and consisted of three additional questions about the span of dancing experience, technique and character. Beighton scale was used to assess benign hypermobility joint syndrome.
Pearson correlation coefficient was calculated for all the compared variables. A weak or strong positive relationship between the studied variables was determined, depending on the value of correlation coefficient. Statistical hypothesis H0: r = 0 was tested along with alternative hypothesis H1: r≠0 in order to generalise results to the population. The average values for study group
Among the 30 subjects who were professional jazz dancers, 27 subjects (90%) was diagnosed with BHJS, while in control group only 9 subjects (30%) were diagnosed with BHJS.
23 dancers (77%) suffered injuries during their career and 21 of them (91%) were diagnosed with BHJS. In control group, 10 subjects (33%) suffered injuries, while only 3 of them were diagnosed with BHJS. The most frequent injury in study group was biceps femoris strain suffered by 12 dancers, and comprising 26% of all injuries. Fractures were the most frequent injury in control group, comprising 64% of all injuries. Types and location of the injuries are shown in tables 2 and 3.
Types of injuries suffered by study and control group subjects
| Type of injury | Study group | Control group | ||||||
|---|---|---|---|---|---|---|---|---|
| HS diagnosed | HS not diagnosed | HS diagnosed | HS not diagnosed | |||||
| No. of subjects | % | No. of subjects | % | No. of subjects | % | No. of subjects | % | |
| Fractures | 3 | 8% | 0 | 0% | 2 | 67% | 4 | 57% |
| Joint injuries | 10 | 26% | 0 | 0% | 1 | 33% | 1 | 14% |
| Muscle injuries | 21 | 53% | 1 | 100% | 0 | 0% | 2 | 29% |
| Other | 5 | 13% | 0 | 0% | 0 | 0% | 0 | 0% |
| Total | 39 | 100% | 1 | 100% | 3 | 100% | 7 | 100% |
Body parts affected by the injuries suffered by study and control group subjects
| Location of injury | Study group | Control group | ||
|---|---|---|---|---|
| No. of subjects | % | No. of subjects | % | |
| Lower extremity injuries | 40 | 89% | 6 | 55% |
| Shoulder joint injuries | 3 | 7% | 1 | 9% |
| Other | 2 | 4% | 4 | 36% |
| Total | 45 | 100% | 11 | 100% |
Correlation between benign hypermobility joint syndrome and the number of injuries suffered by dancers was deemed statistically significant (tab. 4).
Correlation between the injuries of dancers and BHJS
| Study group | Control group | |
|---|---|---|
| Pearson linear correlation coefficient | 0.45 | -0.10 |
| Student’s t-test value | 2.63 | -0.54 |
| p-value | 0.02 | 0.34 |
The survey also contained questions about stabilization exercises. The majority of the subjects – 23 dancers (77%) and 20 control group subjects (67%) performed those exercises. However, the time spent on performing the exercises was different for each of the groups. On average, study group subjects performed the exercises twice weekly for a total of 34.3±28.3 minutes, while control group subjects performed them once per week for ca. 13±27 minutes.
Stabilization exercises which the subjects performed most frequently, include exercises 1, 2 and 4 (figure 1). Figure 2 shows a detailed percentage distribution of performed exercises in both groups.
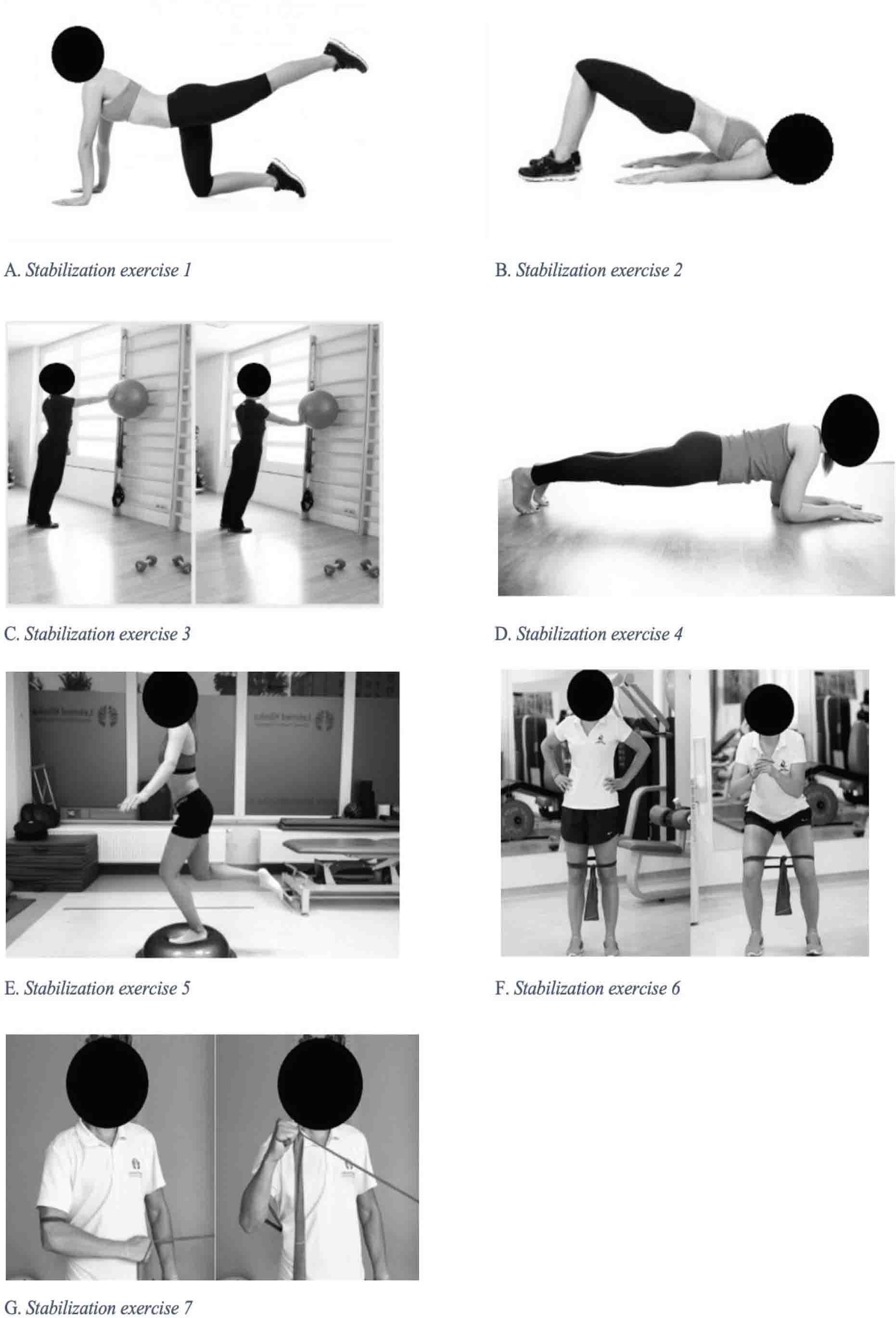
List of stabilization exercises
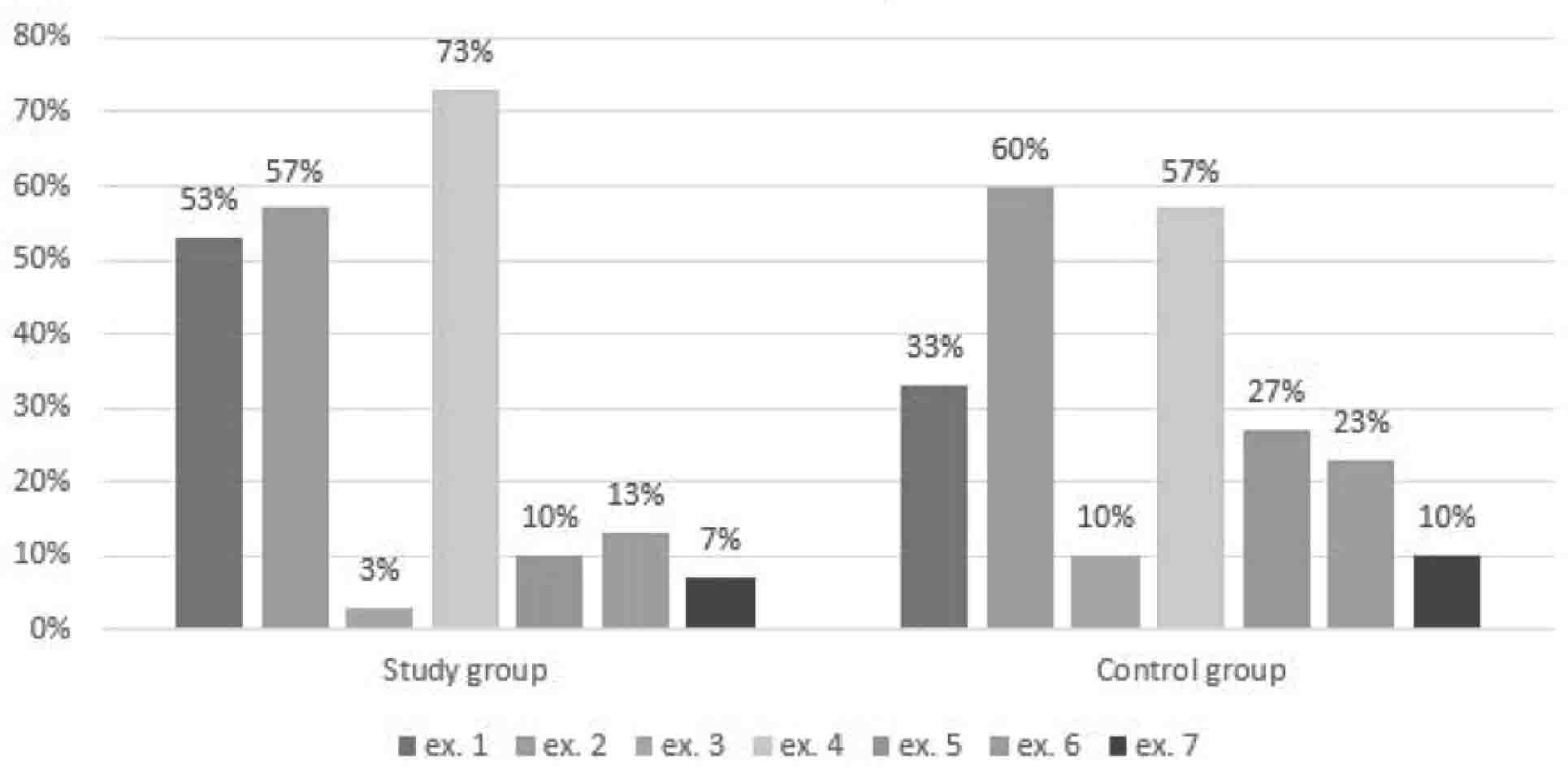
Percentage distribution of performed stabilization exercises in study and control group
A relation between the average time spent weekly on stabilization exercises and the average weekly frequency of pain occurrence was also measured for the dancers. It was determined that the more time the subjects spent on exercising, the rarer was the occurrence of pain (tab. 5). Trendline in the chart no. 2 depicts the studied correlation.
Relation between the average time spent weekly on the exercises and the frequency of pain occurrence in study group
| Pearson linear correlation coefficient | -0.38 |
|---|---|
| Student’s t-test value | -2.16 |
| p-value | 0.04 |
Another relationship related to the exercises performed by subjects concerned the time spent on stabilization training and number of injuries suffered within the period during which the subjects performed the exercises (figure 3). The exercising group was defined as comprising of subjects who spent at least 30 minutes on training every week. It was demonstrated that the training time did not have an effect on the number of injuries. There were no noticeable differences between the numbers of average number of injuries in control and study group. Figure 4 shows the relationship studied in the sample.
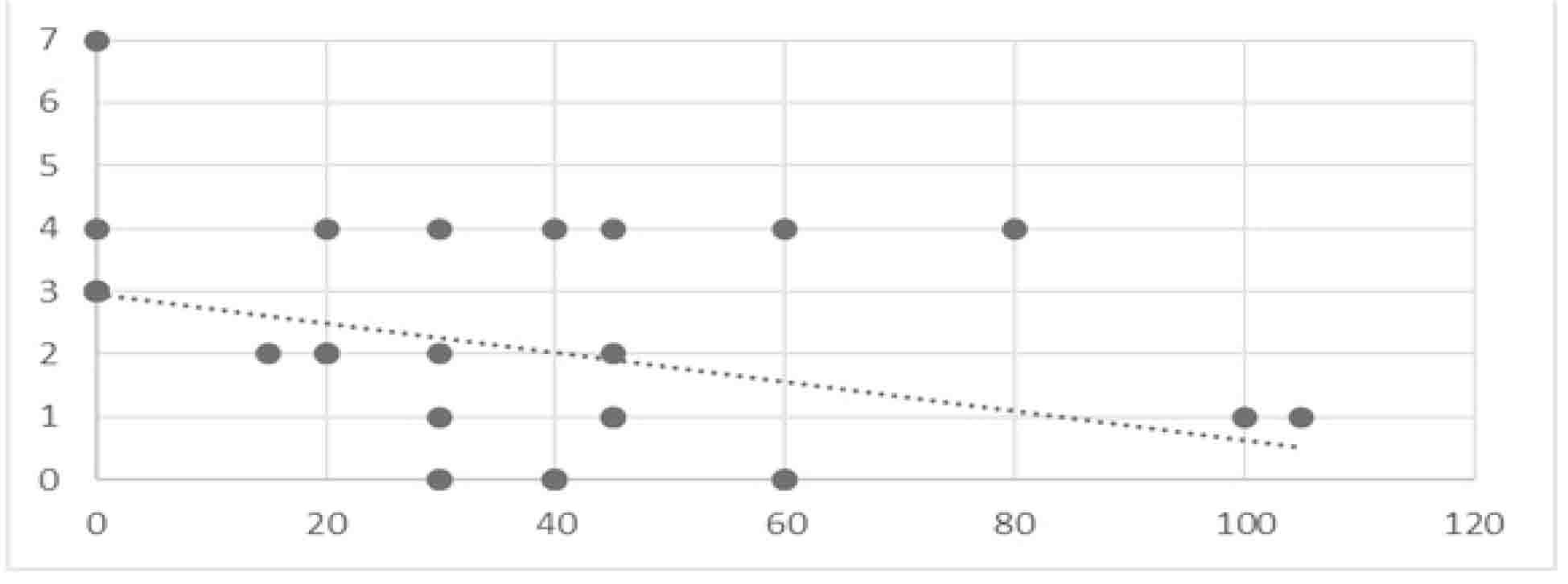
Relationship between the number of suffered injuries and the average time spent weekly on performing stabilization exercises in study group
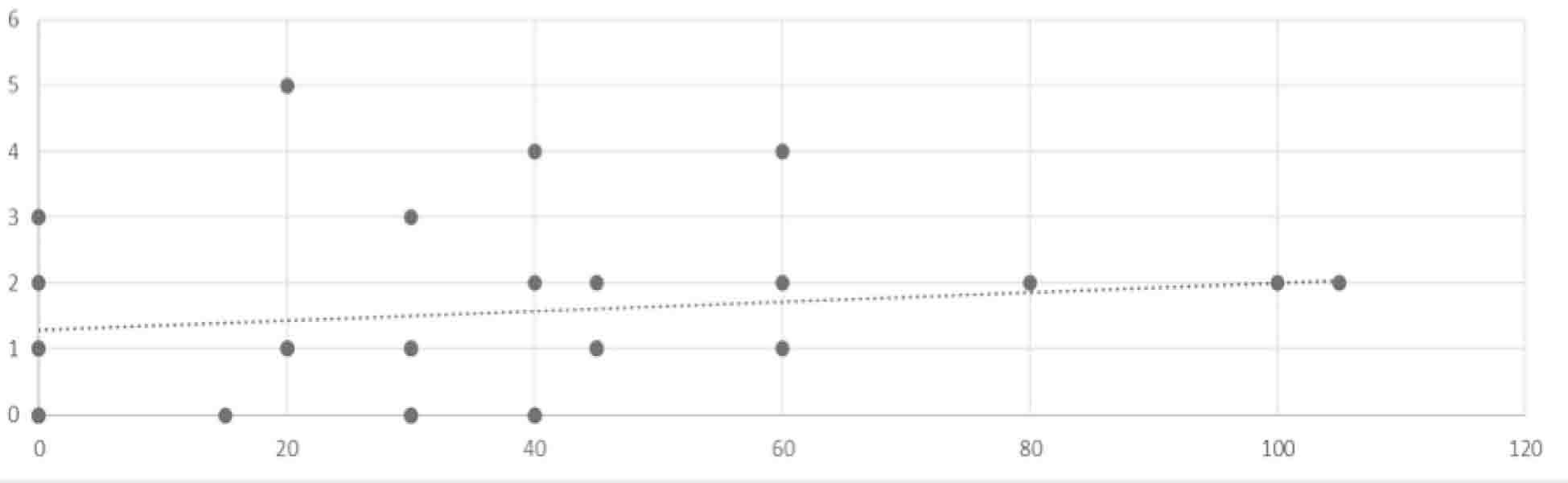
Relationship between the average time spent weekly on stabilization exercises and average weekly frequency of pain occurrence in study group
An important component of the performed study was for the subjects to determine, whether they experience any pain and what joint did the pain occur in. Moreover, the respondents assessed pain intensity on the VAS scale as well as pain occurrence frequency. The most frequent area where study group dancers reported pain was knee joint – 15 subjects, with the avg. VAS-scale intensity of 2.1±2.4. It was also the most reported joint, in terms of pain occurrence frequency – avg. 1.1±1.4 days per week. In terms of both pain intensity and occurrence frequency, the second most reported area in study group was lumbar spine – 11 subjects, with the avg. VAS-scale intensity of 1.8±2.7 and average pain occurrence of 1±1.5 times per week. The same component was assessed in control group. The most reported area of pain occurrence was lumbar spine – 12 subjects (40%). The average VAS-scale intensity amounted to 1.3±1.8, while the pain occurred 1±1.84 times per week, on average.
Dancing exercises generate strain which exceeds the ability of tissue to repair itself, which leads to chronic damage, inflammation and regressive changes. There are two kinds of factors which facilitate the overload of motor organs – acceleration and the results of lifestyle factors [12].
The longer a person has practiced dancing, the higher the risk and frequency of injury among dancers is. This risk, however, is still lower than in other sport disciplines [13]. The most common injuries among dancers include: meniscus tears in knee joint, chronic recurring bursitis, injuries of collateral and cruciate ligaments, avascular necrosis of tibial tuberosity, patellofemoral arthritis, overuse of peroneus muscles, fallen foot arch, hallux valgus, mallet toes and Achilles tendon enthesopathy (an area often compressed by straps of ballet or pointe shoes) [12,14]. Reynolds et al. have demonstrated that jazz dancers much more commonly suffer from injuries in distal joints and in lower extremities [15]. The authors’ own study results have confirmed this. Most of the injuries suffered by dancers were located in lower extremities.
Most dancers and gymnasts have lumbar lordosis which deviates from the norm to a moderate or significant degree. Extreme range of motion, which is necessary for dancing and gymnastics, may contribute to excessive lordosis among dancers, which might later cause severe abnormalities of the spine [16]. Dancers from the analysed group did not report any problems in lumbar spine area, presumably because of their young age.
Schleper et al. have shown that psychological aspect of benign hypermobility joint syndrome. People suffering from BHJS have also been reported to have decreased physical fitness as well as increased fatigue and depression, as compared to control group [17]. This aspect, albeit important, was not analysed in the authors’ study.
One of the indicated preventive measures in terms of injuries and overload is the incorporation of stabilization exercises to one’s training routine, which helps strengthen weakened structures and increase neuromuscular coordination [1]. Preventive measures also include: the use of joint braces and Kinesio tape as well as proprioception training [18]. In order to prevent injuries and overload dancers are advised to perform stabilization exercises, which are also beneficial in pain reduction.
Importance of the study. This is one of the first studies in the available literature which analyses the relationship between BHJS and injury proneness among jazz dancers.
Limitations of the study. The analysis of injuries was conducted with the use of a survey created by the authors. Financial constrictions prevented any other form of study.
Benign hypermobility joint syndrome occurred more frequently among jazz dancers than people who do not practice dance or other sport disciplines professionally.
Injury proneness of jazz dance was linked to BHJS.
Stabilisation exercises appear to be beneficial in pain reduction.