
There is a growing body of research that emphasizes the important role of heart rate variability (HRV) in reflecting the balance between the sympathetic and parasympathetic nervous system [1–6]. Heart rate variability is a simple and informative indicator of autonomic dysfunction and predictor of cardiovascular pathology [7–10]. Heart rate variability reflects the activity of the cardiovascular system, regulation mechanisms of the whole organism, as well as the individual’s emotional state. The findings of Lee et al. [11] indicate that HRV analysis could be used as a prognostic factor and survival in patients with breast cancer. The importance of assessing HRV in this population is due to the close association with adverse surgical effects and autonomic dysfunction in breast cancer survivors. Furthermore, assessment HRV has become an efficient test of woman’s cancer rehabilitation [3,4].
High rates of cardiovascular diseases in patients with breast cancer are associated with the excessive activity of the sympathetic nervous system. Specific cancer therapies have a great impact on autonomous regulation of cardiac rhythm, which reflects the slightest changes in organism [6,8–10]. Physical activity is increasingly recognized as effective method of reducing cardiovascular risk and improving autonomic modulation for patients who survived cancer.
A growing body of research demonstrates the benefits of yoga exercises for improving mental and physical health in patients with breast cancer. This research suggests that yoga exercises can be an effective tool for relieving fatigue, arm pain, improving sleep disturbance and fitness outcomes in patients with cancer [12–19]. However, the impact of yoga’s effects on HRV in breast cancer survivors is not well understood. Most of the current Pilates studies are primarily focused on the impact on fitness, shoulder range of motion, upper extremity circumference, and quality of life in patients with breast cancer [20–22]. Therefore, the question of the effect of Pilates on HRV also requires further investigation.
Consequently, the effects of yoga and Pilates on autonomic dysfunction in patients with breast cancer performed in a rehabilitation setting is relevant.
This research received approval from the Khortytsia National Academy and followed the tenets of the Declaration of Helsinki. Comprehensive sociodemographic characteristics of patients are shown in Table 1. There were no baseline differences between the studied groups. The focus on women aged between 50 and 60 years was used, because of the incidence of breast cancer is highest in this age category.
CONSORT flow diagram is presented at figure 1.
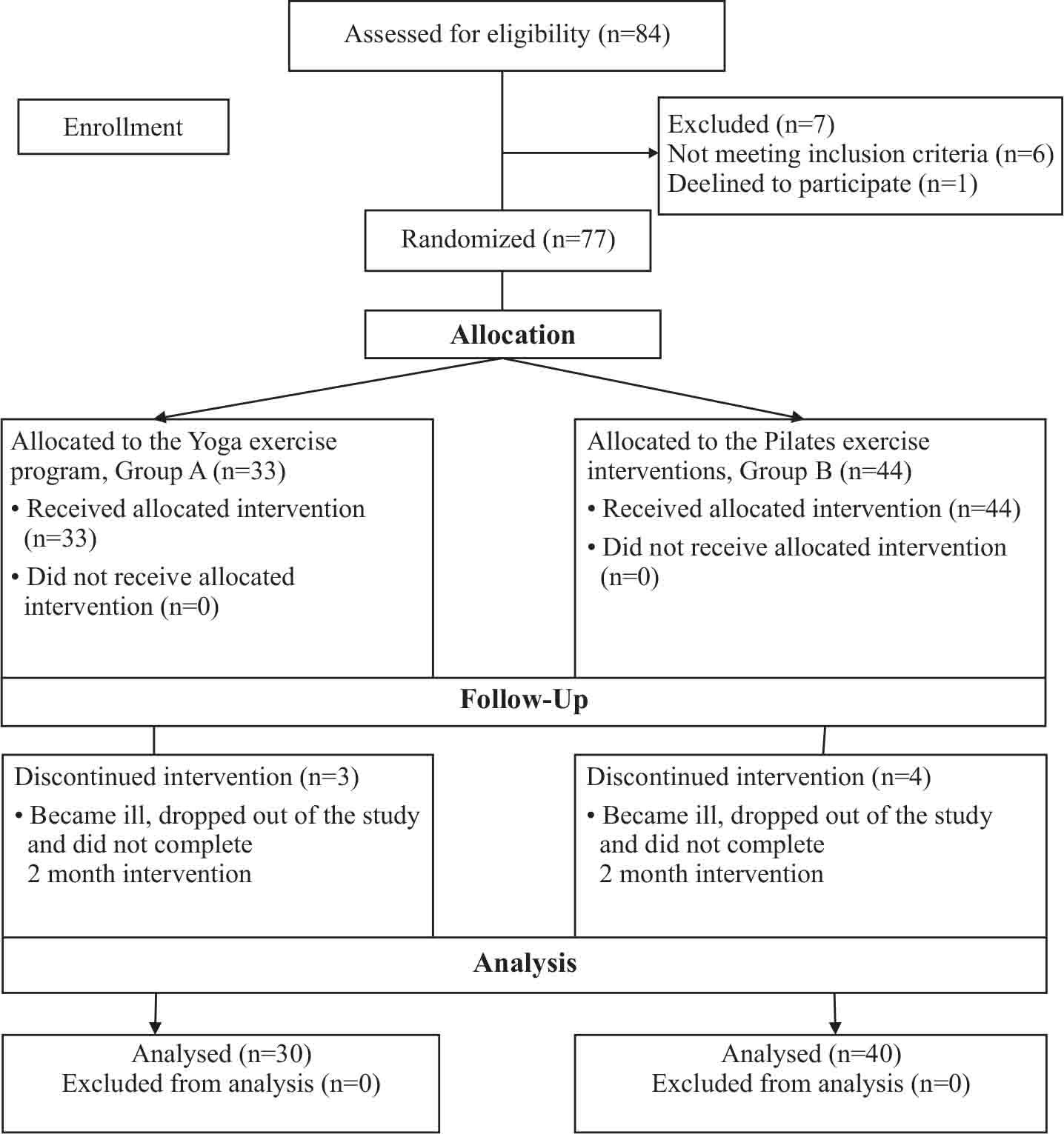
CONSORT flow diagram
Sociodemographic and treatment-related characteristics of study participants
| Characteristics | Groups | p | ||
|---|---|---|---|---|
| A (n=30) | B (n=40) | |||
| Age, (M±SD) | 59.10±1.37 | 59.40±1.24 | >0.05 | |
| Race | White, n (%) | 29 (97%) | 38 (95%) | >0.05 |
| Black, n (%) | 1 (3%) | 2 (5%) | >0.05 | |
| Married/committed relationship, n (%) | 28 (93%) | 36 (90%) | >0.05 | |
| High school graduate, n (%) | 16 (53) | 20 (50%) | >0.05 | |
| College graduate, n (%) | 13 (43%) | 18 (45%) | >0.05 | |
| Post-graduate, n (%) | 1 (3%) | 2 (5%) | >0.05 | |
| Body mass index, kg/m2, (M±SD) | 24.11±0.38 | 24.20±0.44 | >0.05 | |
| Treatment | Radiotherapy, n (%) | 27 (90%) | 38 (95%) | >0.05 |
| Chemotherapy, n (%) | 3 (10%) | 2 (5%) | >0.05 | |
| Surgery type (mastectomy by Madden), n (%) | 30 (100%) | 40 (100%) | >0.05 | |
| Time since treatment completion, months (M±SD) | 5.13±2.87 | 5.13±2.79 | >0.05 | |
| Cancer Stage | Stage 1, n (%) | 9 (30%) | 14 (35%) | >0.05 |
| Stage 2, n (%) | 21 (70%) | 26 (65%) | >0.05 | |
Eighty-four patients with breast cancer were eligible for this study. The inclusion criteria were as follows: 50–60 years of age, recent history of modified radical mastectomy, 6 months after breast cancer surgery, body mass index no more than 25 kg/m2, consent to participate in the study. Exclusion criteria consisted of women with bilateral mastectomy, chronic obstructive lung disease, metastases, ischemic heart disease, III stage of breast cancer.
After the exclusion of 7 women, 77 participants were randomly allocated to a yoga exercise program (group A, n=33) and Pilates exercise program (group B, n=44). We used Pilates for control group B since there was some research about the effect on HRV in patients with breast cancer. Heart rate variability parameters were evaluated at baseline, after six and twelve months of yoga exercises. 7 women did not complete the interventions and dropped out. Attendance rate of the sessions in group A was 92%, in group B was 90%. Finally, 30 women of group A and 40 women of the group B completed the intervention and were analyzed. There were no baseline differences between the two intervention groups.
Short-term recordings of the beat-to-beat intervals were used to obtain the following HRV parameters: SDNN (standard deviation of the normal-to-normal intervals), RMSSD (square root of the mean of the squared differences between adjacent normal RR interval), TP (total power), VLF (very low frequency), HF (high frequency), LF/HF ratio, SI (stress index) [23]. HRV indicators were assessed with the electrocardiographic complex KARDIOLAB (Scientific and Technological Centre of Radio Electronic Medical Equipment and Technologies XAI-Medica of the National Aerospace University, Kharkiv, Ukraine, registration certificate number 6037/2007, conformity certificate number UA-MI/2p-2765-2009).
Data recorded (mean, and standard error of the mean) were analyzed using Statistica for Windows (version 8.00). Data was evaluated for normality assumption, homogeneity, and occurrence of extreme scores before concluding analysis. The distribution of the data recorded was tested using the Shapiro-Wilk test. This analysis was performed as preliminary measure before parametric calculations of the analysis of difference. Dependent T-tests were used to analyze HRV parameters in one group between baseline and post-intervention. Independent sample t-tests were used to compare post-intervention HRV parameters between two groups of women.
Group A attended three Yoga exercises sessions per week for twelve months. The components of yoga exercise program were based on the patients’ individual baseline functional state of the cardiovascular system (FSCS) that was classified as average, lower-than-average and low level by the following form [24]:
A – age, years;
HR – heart rate, beats/min;
MBV – minute blood volume, l/min;
LVW – left ventricular work, kgm;
1,778 – absolute term of regression;
0,006; 0,012; 0,099; 0,076 – multiple regression coefficients;
58,97; 5,47; 73,38; 8,98; 3,35; 0,63; 4,09; 0,79 – constant coefficients.
Proposed yoga exercise program for patients with breast cancer also differentiated depending on the duration and intensity of the session, the number of exercise repetitions, as well as their percentage. The breathing exercises performed with an emphasis on a long exhalation and were coordinated with movements. The duration of asana retention, its complexity and number of repetitions was different depending on the level of the functional state of the woman. Exercise intensity was gradually increased from low to moderate. Women constantly concentrated on their own feelings while doing the exercises. Respiratory exercises were performed in stable sedentary poses that allowed to concentrate attention on the act of breathing. The general structure and content of yoga-therapy exercises for women with different levels of functional state of cardiovascular system is given at Figure 2.
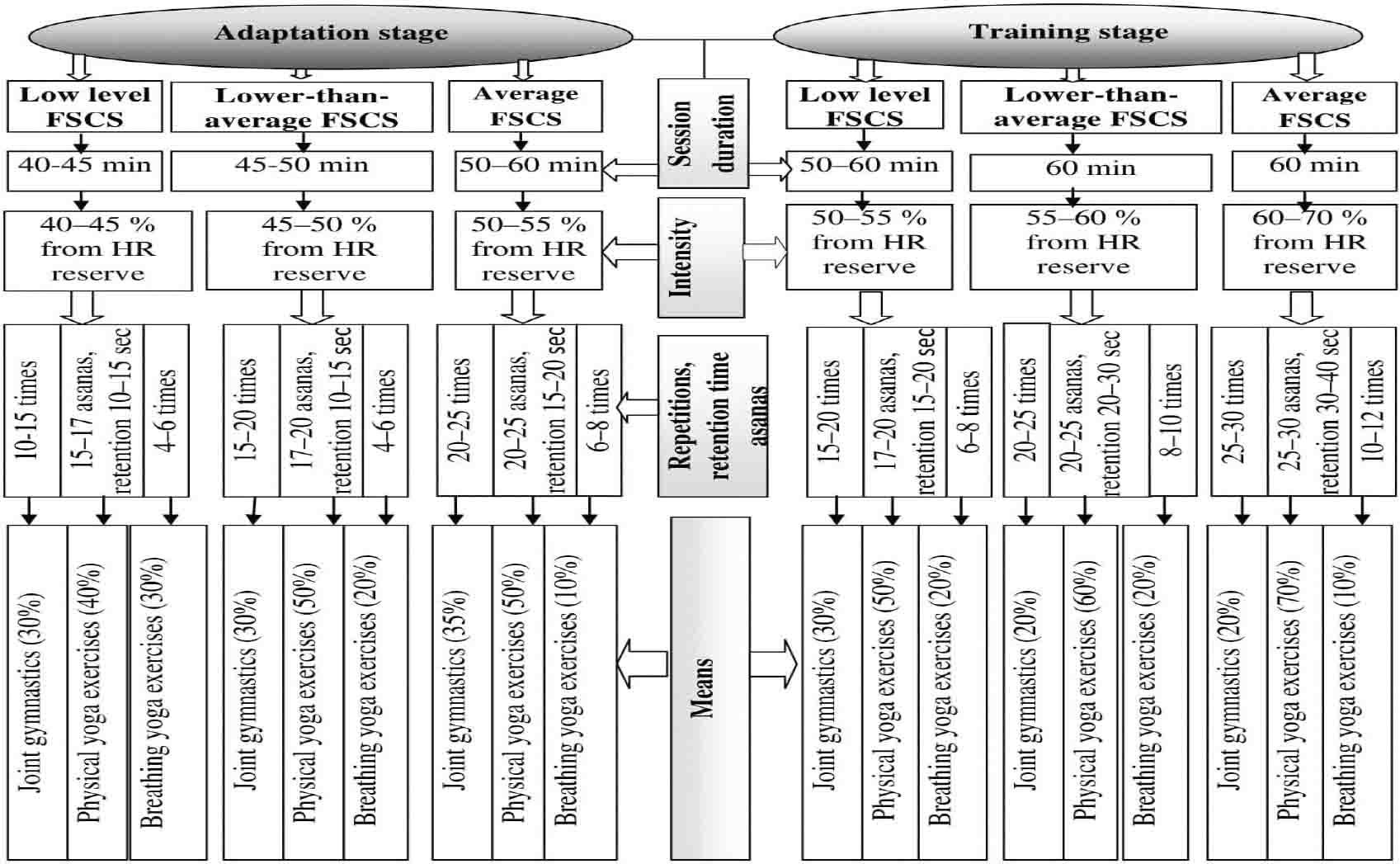
Structure and content of yoga program for breast cancer patients
Group B participated in Pilates exercises 3 times per week for twelve months. Aggregated time of Pilates also depended on the functional state of the cardiovascular system and lasted from 40-45 minutes at the adaptation rehabilitation stage to 1 hour at training stage. The intensity was varied from 40-45% to 60-70% of reserve heart rate. Heart rate was monitored using Polar in both interventions. The Pilates program included active and passive stretching, exercises for good posture, and resistive exercises, with their intensity related to the cardiovascular functional status. Resistance and flexibility exercises targeted at all major muscle groups. All exercises were performed with musical accompaniment and clearly showed by physiotherapist.
Pilates mat work was the most important part of the session for women at adaptation and training stages. It was necessary for the formation of initial Pilates skills, principles and successful task solution in patients with breast cancer.
The dynamics of HRV parameters in group A is shown in Table 2 during the outpatient rehabilitation. Based on the results of the six-month monitoring, it was found that the yoga intervention resulted in a significant improvement in autonomous modulation.
Dynamics of HRV indicators in group A during outpatient rehabilitation
| Indicator | Baseline data | Duration of rehabilitation | |
|---|---|---|---|
| six months | twelve months | ||
| SDNN (ms) | 21.19±1.08 | 23.60±1.04** | 26.72±1.17••• |
| RMSSD (ms) | 18.59±1.50 | 21.64±1.18 | 23.50±0.99•• |
| TP (ms2) | 440.91±42.08 | 541.96±45.82** | 720.69±61.93••• |
| VLF (ms2) | 113.29±18.02 | 160.32±14.19* | 223.05±27.93•• |
| LF (ms2) | 167.92±20.33 | 179.92±21.61 | 256.30±27.47•• |
| HF (ms2) | 158.96±22.44 | 199.29±21.67 | 236.56±22.57• |
| LF/HF (c.u.) | 1.82±0.33 | 0.98±0.10** | 1.35±0.19 |
| Si (c.u.) | 361.80±32.21 | 265.36±17.22** | 224.56±18.66•• |
Notes: – p<0,05;
– p<0,01; compared with the baseline data;
– p<0,05;
– p<0,01;
– p<0,001 compared with the baseline data
Analysis of HRV showed that SDNN intervals significantly improved by 2.41 ms (p<0.01), TP improved by 101.05 ms2 (p<0.01), VLF improved by 47.03 ms2 (p<0.05), and Si improved by 96.44 c.u. (p<0.01). Dynamics of spectral indicators in group A showed an increase in TP, but changes for spectral components were different. The structure of HRV was characterized by an increase in overall variability due to preferential growth of VLF component and a slight increase of HF and LF parameters. Sympathicotonia reduction was indicated by a decrease in LF/HF ratio by 0.84 c.u. (p<0.01).
After twelve months of performing yoga, the above mentioned parameters of HRV also changed significantly: SDNN improved by 5.53 ms (p<0.001), RMSSD improved by 4.91 ms (p<0.01), TP improved by 279.78 ms2 (p<0.001), VLF improved by 109.76 (p<0.01), LF improved by 88.38 ms2 (p<0.01), HF improved by 77.60 (p<0.05), and Si improved by 137.24 c.u. (p<0.01). Dynamics of overall activity of the autonomic effect on the heart rate was characterized by a significant increase in all spectral components (VLF, LF and HF).
Women of group B showed a substantial increase TP by 108.80 ms2 (p<0.05) due to preferential growth of VLF by 112.27 ms2 (p<0.01) after 6-month performing of Pilates exercises (Table 3). A significant decrease was observed in Si by 70.80 c.u. (p<0.05), which indicated an exertion reduction of regulatory processes after 12 months of Pilates training.
Dynamics of HRV indicators in group B during outpatient rehabilitation
| Indicator | Baseline data | Duration of rehabilitation | |
|---|---|---|---|
| six months | twelve months | ||
| SDNN (ms) | 21.30±1.08 | 23.36±1.07 | 23.44±1.19 |
| RMSSD (ms) | 19.46±1.96 | 17.77±1.05 | 20.16±1.08 |
| TP (ms2) | 436.91±41.04 | 545.71±30.36* | 550.36±41.02 |
| VLF (ms2) | 98.74±12.35 | 211.01±30.54** | 150.73±32.46 |
| LF (ms2) | 161.94±14.96 | 191.61±20.50 | 227.36±36.43 |
| HF (ms2) | 173.79±32.76 | 143.09±14.74 | 172.23±20.65 |
| LF/HF (c.u.) | 1.82±0.25 | 1.69±0.31 | 1.49±0.22 |
| Si (c.u.) | 351.85±25.53 | 290.72±19.86 | 281.05±17.69• |
Notes: – p<0,05;
– p<0.01 compared with the baseline data;
– p<0.05 compared with the baseline data
Women of group A showed significantly better results compared to group B in SDNN by 3.28 ms (p<0.05), RMSSD by 3.34 ms (p<0.05), TP by 170.33 ms2 (p<0.05), HF by 64.33 (p<0.05), and Si by 56.49 c.u. (p<0.05) after 12 months (table 4).
Comparison of HRV indicators between the group A and group B during outpatient rehabilitation
| Indicator | six months | twelve months | ||
|---|---|---|---|---|
| group A | group B | group A | group B | |
| SDNN (ms) | 23.60±1.04 | 23.36±1.07 | 26.72±1.17 | 23.44±1.19• |
| RMSSD (ms) | 21.64±1.18 | 17.77±1.05* | 23.50±0.99 | 20.16±1.08• |
| TP (ms2) | 541.96±45.82 | 545.71±30.36 | 720.69±61.93 | 550.36±41.02• |
| VLF (ms2) | 160.32±14.19 | 211.01±30.54 | 223.05±27.93 | 150.73±32.46 |
| LF (ms2) | 179.92±21.61 | 191.61±20.50 | 256.30±27.47 | 227.36±36.43 |
| HF (ms2) | 199.29±21.67 | 143.09±14.74* | 236.56±22.57 | 172.23±20.65• |
| LF/HF (c.u.) | 0.98±0.10 | 1.69±0.31* | 1.35±0.19 | 1.49±0.22 |
| Si (c.u.) | 265.36±17.22 | 290.72±19.86 | 224.56±18.66 | 281.05±17.69• |
Notes: – p<0.05 compared data between groups for six months;
– p<0.05 compared data between groups for twelve months
In general, the beneficial effect of yoga exercises on autonomic regulation was characterized by an increase of the parasympathetic and baroreflex effects on the cardiovascular system and a decrease in the tonic effects of the sympathetic nervous system.
This study demonstrated the significant impact of yoga exercises can have on improving the functional state of autonomic nervous system in patients with breast cancer.
Based on the results after 12 months of participating, it was found that Yoga exercise intervention was a more valuable and effective tool than Pilates for increasing overall HRV, especially of the parasympathetic nervous system.
The results agreed with recent studies that patients with breast cancer present with dramatically low HRV values [2,6,8,10,11] and that regular physical exercise is considered as effective tool for enhancing autonomic function and balance [3,4].
Previous studies [13,15,25] have been focused on the effects of yoga on reducing fatigue, depression and stress in patients with breast cancer.
A number of studies have investigated different yoga breathing patterns and meditative practice on HRV in healthy volunteers [25–28], but information about effects of yoga on autonomic regulation in patients with breast cancer is almost absent.
Unique to this study, we considered the current level of the functional state of cardiovascular system of our participants in the proposed yoga exercise program. The prescribed yoga program for our participants with breast cancer also varied depending on the duration and intensity of the session, the number of exercise repetitions. The combination of various asanas technique, breathing exercises and relaxation modes had a great impact on the autonomic function and balance in patients with breast cancer. The findings obtained in the current study demonstrated the benefits of longterm yoga practice in reducing stress and increasing overall HRV in patients with breast cancer.
Despite these strengths, the current research also had some important weaknesses. HRV analysis was analyzed only by short-term indicators and differences in emotional condition of women could have an impact on the obtained results. Further studies are needed to investigate the effectiveness of yoga on HRV parameters in heterogeneous population.
Performing the yoga exercise program resulted in an increase of the parasympathetic and baroreflex effects on the cardiovascular system and a decrease in the tonic effects of the sympathetic nervous system. Yoga should be considered as an effective tool in normalizing the functional state of the autonomic nervous system.