
Coronavirus disease 2019 (COVID-19), also known as novel coronavirus pneumonia, is a typical type of pneumonia caused by infection with severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2), which triggers a series of symptoms. COVID-19 caused a pandemic in Wuhan, Hubei, China, in 2019 and then rapidly spread worldwide (Rai et al. 2021). The global COVID-19 mortality rate in 2021 reached 120.3/100,000 people/year. Because the COVID-19 epidemic became a pandemic in a short period of time, a new epidemic prevention and control policy was established in December 2022 to standardize epidemic prevention and control strategies (Baloch et al. 2020; Wang et al. 2022).
Coinfection with respiratory viruses and other bacteria or viruses may increase morbidity or mortality. The underlying mechanism may involve viral destruction of the body’s immune system, leading to bacterial adhesion and aggravating the tissue damage caused by the virus, thereby leading to damage to the lung mucosal structure (Melvin and Bomberger 2016). Since there were relatively few studies on COVID-19 complicated by bacterial infection, and bacterial infection types and rates vary widely across hospitals and geographic regions, clinical physicians treating patients with coinfection prescribe medications based on their experience. Clinical trial data and scientific evidence are lacking (Lee et al. 2023). In most existing studies, the detection of microorganisms that cause coinfection was performed in only half of the study population, which did not represent all coinfection cases, and the results showed particular bias (Wang et al. 2021). Therefore, the purpose of this study was to retrospectively analyze bacteria associated with SARS-CoV-2 in Shaanxi Province by describing the epidemiological factors, clinical characteristics, bacterial infections, and drug-sensitivity test results of COVID-19 patients since the adjustment of China’s epidemic prevention policy. The findings of this study will help society better understand this infectious disease and will guide efforts to mitigate factors that influence coinfection and to treat bacterial infections associated with SARS-CoV-2.
The clinical data of COVID-19 patients since the adjustment of the epidemic policy in Shaanxi Province (from December 7, 2022, to February 15, 2023), including the epidemic history, history of present illness, symptoms, laboratory markers, and chest CT findings, were collected from the hospital laboratory information system (LIS) database. The patients were divided into mild, moderate, and severe COVID-19 groups according to the diagnosis and treatment protocol for SARS-CoV-2 infection (Trial Version 10) (NHC and NATCM 2023).
Positivity for SARS-CoV-2 RNA and antigen was confirmed by reverse transcription polymerase chain reaction (RT-PCR). High-quality sputum samples (those with < 10 epithelial cells/HPF and > 25 leukocytes/HPF) were eligible for analysis.
According to the diagnosis and treatment protocol for SARS-CoV-2 infection (Trial Version 10), the patients were divided into mild, moderate, and severe COVID-19 (Ramezani-Jolfaie et al. 2023) groups based on the following criteria: mild group: presence of upper respiratory tract infection, such as dry throat, cough, and fever, as the primary manifestation; moderate group: persistence of high body temperature for > 3 days and/or cough, shortness of breath, etc., with imaging examination revealing the characteristic manifestations of pneumonia caused by SARS-CoV-2; and severe group: presence of respiratory failure and the need for mechanical ventilation, shock or other organ failure requiring intensive care unit (ICU) monitoring and treatment. In line with standard clinical management in our region during the study period, all patients classified as moderate or severe were hospitalized (inpatients), while those with mild disease were managed as outpatients.
In accordance with standard procedures for bacterial identification, the collected sputum samples were inoculated onto blood, Mac-Conkey, and chocolate agar plates (Autobio Diagnostics Co., Zhengzhou) and cultured at 35°C in a 5% CO2 environment. Colonies were identified after 24–48 h of culture. Bacterial cultures were obtained based on clinical indications, including: i) respiratory symptoms persisting > 5 days, ii) purulent sputum, iii) recurrent fever, or iv) elevated inflammatory markers (PCT > 0.5 ng/ml). Sampling timing was determined by symptom presentation rather than fixed intervals from SARS-CoV-2 detection. Bacterial co-infection diagnosis required both positive culture results and compatible clinical findings.
After observing the colony morphology, smear staining was performed. BioMérieux identification cards were selected according to the staining results, and bacteria were identified using the VITEK®2 COMPACT instrument (bioMérieux, France) or the MALDI Biotyper® IVD MBT system (Bruker Daltonics GmbH & Co., Germany). The quality control strains Pseudomonas aeruginosa (ACTT 27853), Candida albicans (ACTT 14053), and Escherichia coli (ATCC® 25922™) were used.
Drug sensitivity testing (BioMérieux, France) of Gram-negative bacteria (GNB) was performed using AST-GN13, AST-GN09 and plate cards. The quality control strains used were Escherichia coli ATCC® 25922™, P. aeruginosa ATCC® 27853™, and Haemophilus influenzae ATCC® 49247™. This study primarily focused on the epidemiological characteristics of Gram-negative bacteria; therefore, systematic antimicrobial susceptibility testing was limited to this group of pathogens. A complete list of antibiotic abbreviations and their corresponding full names is provided in Table I.
Antibiotic susceptibility testing abbreviations.
| Abbreviation | Full Name |
|---|---|
| SAM | Ampicillin-sulbactam |
| TZP | Piperacillin-tazobactam |
| CZO | Cefazolin |
| CTT | Cefotetan |
| CAZ | Ceftazidime |
| CRO | Ceftriaxone |
| FEP | Cefepime |
| ATM | Aztreonam |
| ETP | Ertapenem |
| IPM | Imipenem |
| AMK | Amikacin |
| GM | Gentamicin |
| TOB | Tobramycin |
| CIP | Ciprofloxacin |
| LVX | Levofloxacin |
| SXT | Trimeth oprim-sulfameth oxazole |
| CSL | Cefoperazone-sulbactam |
| MEM | Meropenem |
| DOX | Doxycycline |
| MNO | Minocycline |
| TGC | Tigecycline |
| CS | Colistin |
IBM® SPSS® Statistics v26.0 (IBM Corp., USA) and GraphPad Prism v8 (GraphPad Software, USA, www.graphpad.com) were used for data analysis. Categorical variables are presented as frequencies and percentages; continuous variables are presented as the means and medians. p < 0.05 was considered statistically significant.
A total of 2,000 COVID-19 patients met the inclusion criteria. Among these, 300 patients developed bacterial coinfection (90 in the mild, 90 in the moderate and 120 in the severe COVID-19 group). As detailed in Table II, disease severity was significantly associated with both demographic and clinical profiles. The cohort was predominantly male, with the male proportion increasing significantly with severity (from 66.7% to 83.3%, p = 0.001). Furthermore, distinct patterns were observed in clinical symptoms: fatigue and vomiting increased with severity, whereas most respiratory symptoms were more common in mild and moderate cases.
Demographic characteristics of COVID-19 patients with bacterial infection.
| Overall sample (n = 300) | Mild group (n = 90) | Moderate group (n = 90) | Severe group (n = 120) | p-value | |
| Patient characteristics | |||||
| Median age (years) | 79 (59–92) | 79 (59–84) | 81 (68–89) | 78(69–92) | 0.578 |
| Sex (n (%)) | |||||
| Male | 240 | 60/90 (66.7%) | 80/90 (88.8%) | 100/120 (83.3%) | 0.001 |
| Female | 60 | 30/90 (33.3%) | 10/90 (11.1%) | 20/120 (16.6%) | 0.001 |
| Clinical symptoms | |||||
| Fever | 220 | 70/90 (77.8%) | 60/90 (66.7%) | 90/120 (75.0%) | 0.210 |
| Fatigue | 70 | 10/90 (11.1%) | 20/90(22.2%) | 40/120 (33.3%) | 0.001 |
| Difficulty breathing | 200 | 70/90 (77.8%) | 60/90 (66.7%) | 70/120 (58.3%) | 0.012 |
| Vomiting | 30 | 0 | 0 | 30/120 (25.0%) | < 0.001 |
| Cough and expectoration | 290 | 90/90 (100%) | 90/90 (100%) | 110/120 (91.7%) | < 0.001 |
A comparison of the three groups of patients according to age group revealed that the number of COVID-19 patients in the 70- to 90-year age group was higher than that in the other age groups, and the same was true for the number of patients with COVID-19 complicated with bacterial infection; all patients with moderate to severe COVID-19 with coinfection were over 60 years of age. The patients with severe COVID-19 were mainly between 70 and 90 years old (Fig. 1).
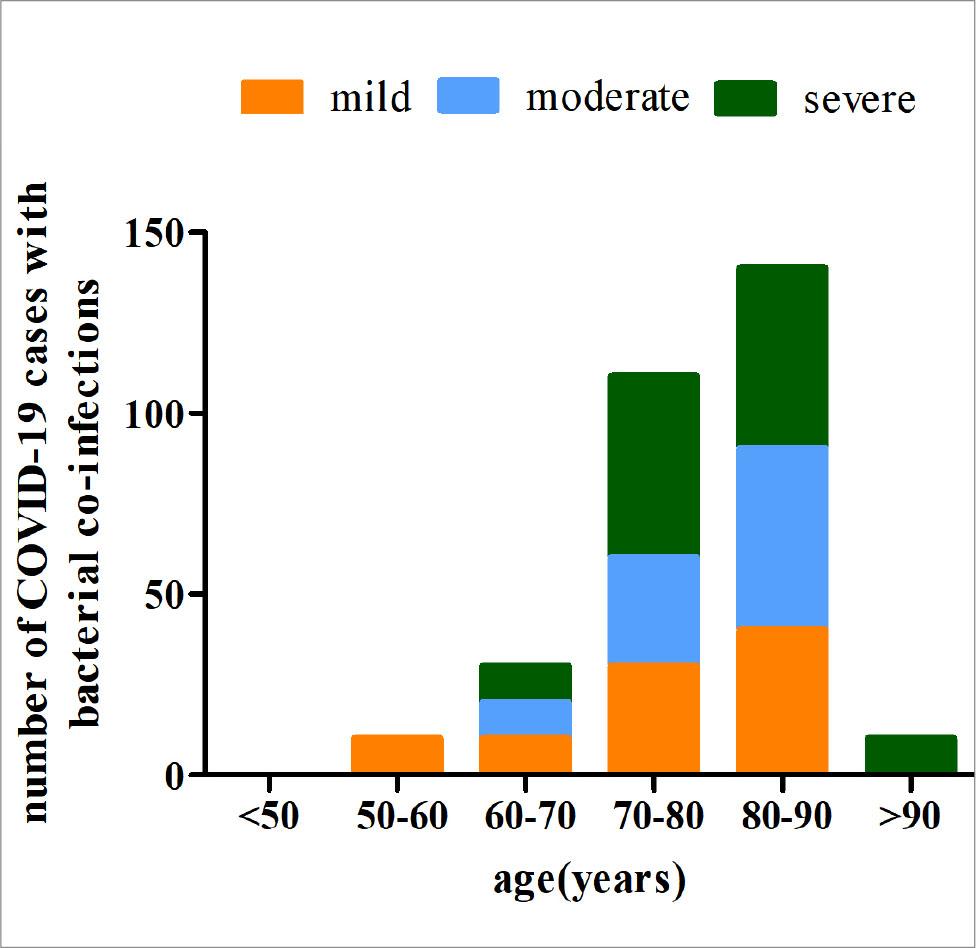
Age distribution of COVID-19 patients with bacterial co-infection, stratified by disease severity.
Among the 2,000 COVID-19 patients, 300 had coinfections with bacteria, mainly Klebsiella pneumoniae (38%) and Acinetobacter baumannii (13%) (Fig. 2). K. pneumoniae was the primary infectious bacterium in the mild group; K. pneumoniae and A. baumannii were the main infectious bacteria in the moderate group and the severe group (Fig. 3).
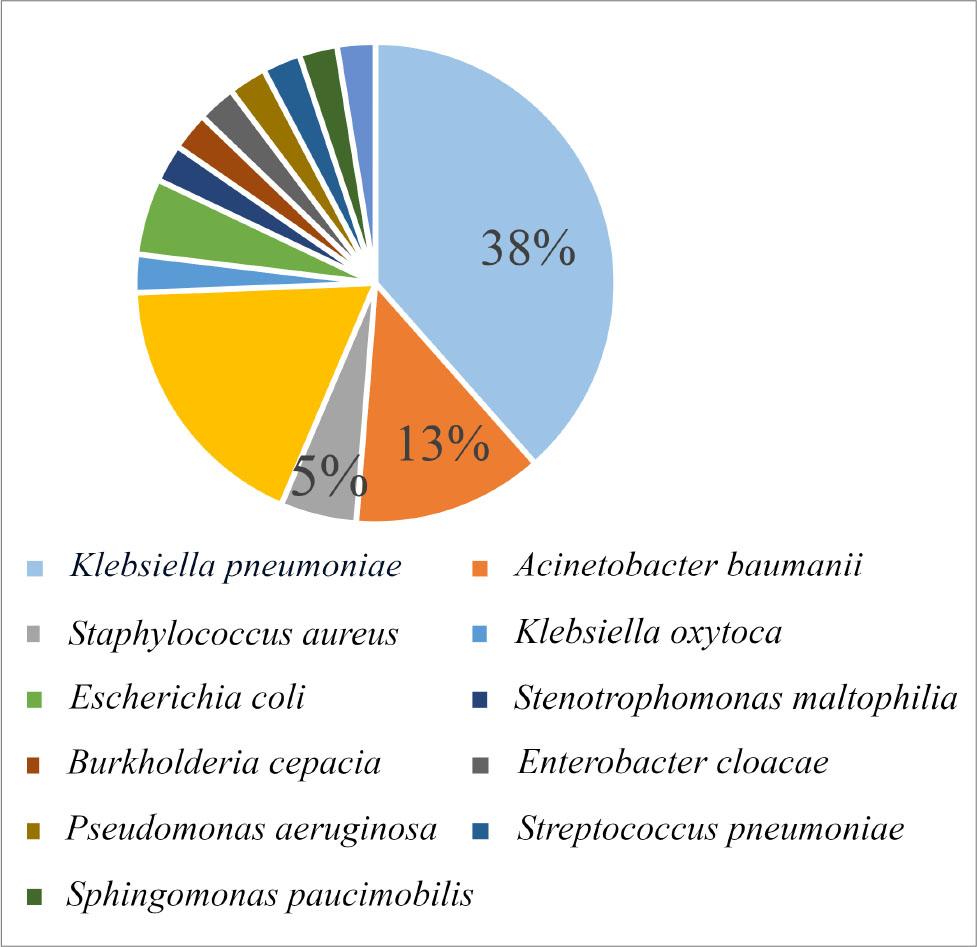
Types of bacterial infections in coronavirus disease 2019 (COVID-19) patients.
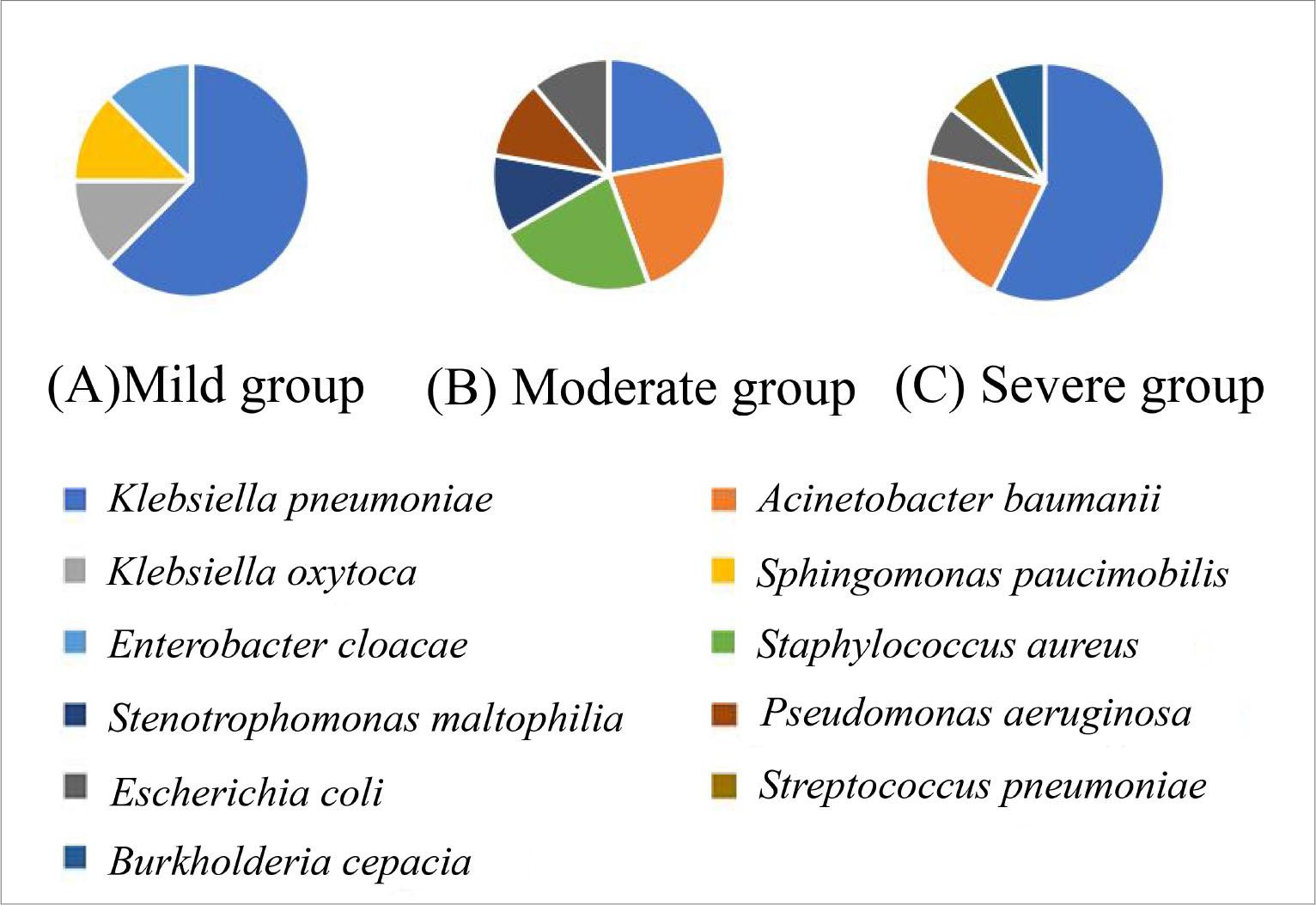
Distribution of bacterial pathogens in COVID-19 patients with co-infections, stratified by disease severity. A) Mild group (n = 90); B) moderate group (n = 90); C) severe group (n = 120).
K. pneumoniae was the most common coinfecting bacterium found in this study, accounting for 38% of the total number of isolated bacteria. In addition, according to the clinical definition of drug resistance, K. pneumoniae was classified as a multidrug-resistant bacteria (Shankar et al. 2017). According to the severity of the patient’s condition, among the antibiotics for K. pneumoniae, the degrees of drug resistance of the mild group and the moderate group were milder, K. pneumoniae strains were drug resistant in more than 60% of the patients with severe COVID-19, and some strains were relatively highly resistant to drugs such as ampicillin/sulbactam, cefazolin, and ceftriaxone (57.1%) and aztreonam and ciprofloxacin (42.9%) (Fig. 4).
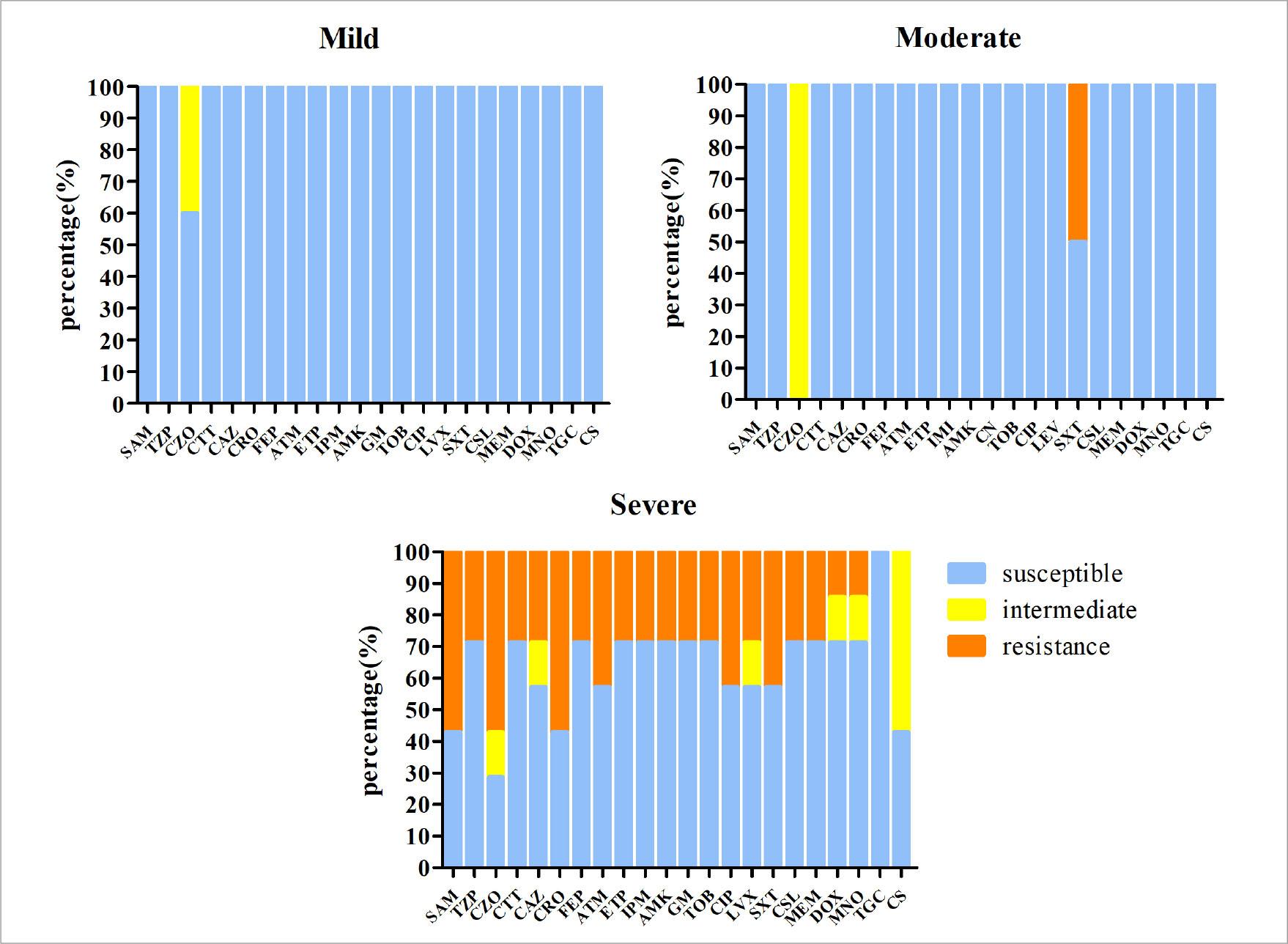
Drug resistance of Klebsiella pneumoniae in different groups.
A. baumannii was the third most common pathogen, accounting for 13% of isolates. There was no drug resistance in the mild or moderate COVID-19 group. In addition, the severe COVID-19 group was sensitive to tigecycline and colistin, and 100% of the A. baumannii strains resistant to piperacillin/tazobactam, ceftazidime, cefepime, imipenem, meropenem, amikacin, tobramycin, ciprofloxacin, doxycycline, and trimethoprim/sulfamethoxazole were completely drug resistant (Fig. 5).
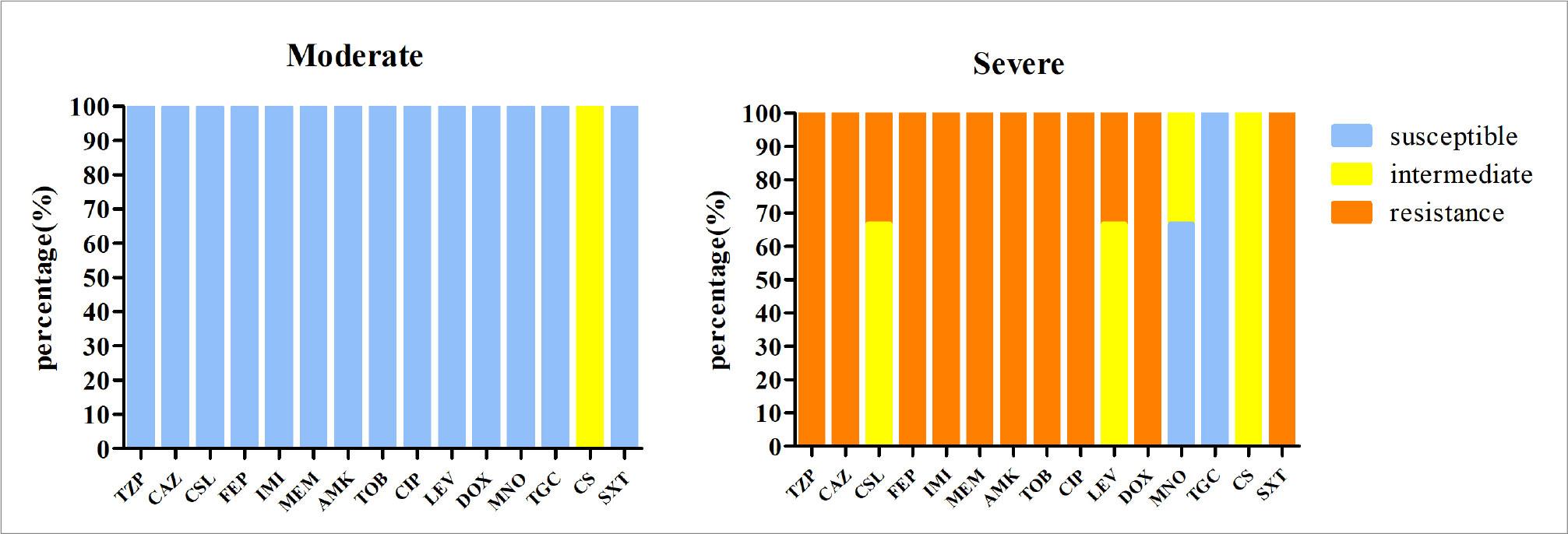
Drug resistance of Acinetobacter baumannii in different groups. Notably, no resistance to any tested antibiotic was detected in bacterial isolates from the mild COVID-19 group.
During the COVID-19 pandemic, SARS-CoV-2 infection complicated by bacterial infection has been a concern for clinicians and researchers. In most observational studies, the rate of bacterial coinfection in COVID-19 patients was low (Lee et al. 2023). However, for patients with severe and critical COVID-19, SARS-CoV-2 coinfection with bacteria makes diagnosis and treatment more difficult and leads to poor outcomes for affected patients.
Previous studies have shown that among COVID-19 patients admitted to the ICU, the mortality of elderly patients is far higher than that of other groups (Mutua et al. 2022). This finding was also confirmed in our study. For both patients with COVID-19 alone and those with COVID-19 combined with bacterial infection, the median age of the moderate-to-severe group was older than the overall median, with most patients in the 70- to 90-year age group. Elderly patients have other underlying diseases and conditions, such as acute myocardial infarction, acute liver injury, and diabetes, which increase the risk of coinfection and death. Although comorbidities were not investigated in our study, long-term ICU hospitalization has also become a potential factor for increased mortality.
Beyond the demographic and clinical risk factors discussed above, the potential role of gut microbiota dysbiosis in COVID-19 pathogenesis and outcomes warrants consideration. A growing body of evidence suggests that SARS-CoV-2 infection can induce gut microbiota dysbiosis, characterized by a reduction in beneficial commensals and an increase in opportunistic pathogens (Chakradhar et al. 2017). This dysbiosis may exacerbate disease severity through the gut-lung axis by impairing immune regulation and amplifying systemic inflammation. Furthermore, pre-existing or infection-aggravated dysbiosis could predispose patients to secondary bacterial infections by compromising mucosal immunity and altering the metabolic environment, potentially explaining part of the individual susceptibility observed in our and other studies. While not directly assessed in our cohort, acknowledging this mechanism provides a more comprehensive pathophysiological perspective on bacterial co-infections in COVID-19.
Among patients with COVID-19 complicated with bacterial infection, male patients were approximately three times more likely to acquire bacterial infection than female patients were, indicating that sex is an important factor affecting complications with bacterial infection. The reason may be that females have stronger immunity to bacterial infections, differences in lifestyle factors (such as less smoking and alcohol consumption), better treatment adherence, and better attitudes toward preventive measures for COVID-19 (Dias et al. 2022).
A 2020 meta-analysis revealed that the bacterial coinfection rate among COVID-19 patients was 4.9% (Langford et al. 2020). Calderon et al. (2023) reported that bacterial coinfections accounted for 4% of total infections, affecting 12% of critically ill patients, which is similar to our study. In previous viral pandemics, the leading cause of death was bacterial coinfection rather than direct viral damage (Pandey et al. 2022). This situation is more common in critically ill patients. In the published literature, the predominant bacterial strains causing coinfections in COVID-19 patients vary widely, with P. aeruginosa, E. coli, Staphylococcus aureus, and Streptococcus pneumoniae among the most common isolates (Garcia-Vidal et al. 2021). Bacterial culture predominantly yielded gram-negative bacilli (GNB), with K. pneumoniae and A. baumannii identified as the predominant pathogens. Both bacterial pathogens were significantly associated with disease exacerbation and mortality.
The high prevalence of multidrug-resistant organisms (MDROs), such as CRKP and CRAB, observed in our severe patient group is a significant finding. This is very likely attributable to the hospital environment, where prolonged stays, invasive procedures, and broad-spectrum antibiotic use create selective pressure for the emergence of resistant pathogens. Our finding that all severe patients with K. pneumoniae and A. baumannii coinfections were positive for MDROs strongly supports the notion that these infections were primarily hospital-acquired.
In our study, all K. pneumoniae isolates from the mild and moderate groups were ESBLs-negative. Both patient groups demonstrated relatively simple antibiotic resistance profiles, with no multidrug-resistant strains identified. This discrepancy may be attributed to shorter hospital stays, fewer invasive procedures, and lower antibiotic exposure among non-severe patients. In contrast, the severe group showed significantly higher incidence of ESBLs-positive and carbapenem-resistant K. pneumoniae. CRE infections were associated with increased mortality rates and poorer clinical outcomes. A retrospective study revealed that the incidence of CRE colonization increased from 6.7% in 2019 to 50% between March and April 2020 (Tiri et al. 2020). These findings indicate that carbapenemase-resistant K. pneumoniae is a significant threat to human life and health worldwide. Although the coinfection rate of A. baumannii is not as high as that of K. pneumoniae, the mortality caused by A. baumannii is far higher than that caused by K. pneumoniae. Therefore, A. baumannii is an opportunistic pathogen (Cultrera et al. 2021) and may cause secondary infections, especially when inpatients have viral respiratory infections that can evade antibiotic treatment, there-by affecting severely ill inpatients with low immunity (Monem et al. 2020). Compared with COVID-19-negative patients, CR-Ab infections are more common in SARS-CoV-2-positive patients admitted to the ICU (Cultrera et al. 2021). Therefore, A. baumannii is an opportunistic pathogen (Cultrera et al. 2021) and may cause secondary infections, especially when inpatients have viral respiratory infections that can evade antibiotic treatment, thereby affecting severely ill inpatients with low immunity.
Notably, our diagnostic workup also identified fungal organisms in a considerable number of patients. Specifically, Aspergillus species and Candida species were isolated in 18% and 2% of the cultured samples, respectively. However, in line with the primary objective of this study to characterize bacterial co-infections, and in the absence of systematic antifungal susceptibility testing (antimycograms), these fungal isolates were not included in the formal resistance analysis or statistical evaluations of clinical outcomes. Their potential clinical impact in our cohort, therefore, remains to be fully elucidated and represents an important avenue for future research.
In this study, among critically ill COVID-19 patients with coinfections by K. pneumoniae and A. baumannii, all were positive for multidrug-resistant CRE, CR-Ab, and ESBLs. There is no explicit agreement on empiric antibiotic treatment for hospitalized patients infected with SARS-CoV-2. Guidance and bacterial infection rates vary to some extent due to hospital environments and geographic factors. Given the potential risks of antibiotic treatment to patients and public health, there must be sufficient evidence to support frontline clinicians’ decision-making in appropriately balancing these risks. Our study revealed that, except for being sensitive to tigecycline, in patients with severe COVID-19 coinfected with K. pneumoniae, the K. pneumoniae strains were all resistant to third-generation cephalosporins (such as ceftazidime), third-generation quinolones (such as ciprofloxacin), aminoglycosides (such as amikacin), and carbapenem (imipenem) antibiotics to different degrees. In contrast, A. baumannii was 100% resistant to drugs other than tigecycline and colistin. When only antibiotic resistance was considered, Klebsiella spp. were resistant to β-lactam antibiotics (including third-generation cephalosporins and carbapenems), and A. baumannii was resistant to carbapenemase antibiotics (Sang et al. 2021). According to the Clinical and Laboratory Standards Institute (CLSI 2024) drug-sensitivity test criteria, colistin’s clinical efficacy is limited, and other drugs are recommended for use instead. One study revealed that, compared with the estimated prevalence of bacterial coinfection, the overall use of antibiotics in COVID-19 patients was higher; almost all patients in the coinfection group and all patients in the suspected coinfection group initiated antibacterial treatment immediately (Calderon et al. 2023). The purpose of this study was to understand the occurrence of bacterial coinfection in COVID-19 patients in Shaanxi Province, the distribution of strains and drug resistance, and to provide supporting evidence, thereby reducing the negative impact of empirical medication.
This study has several limitations that should be acknowledged. First, the retrospective design introduces an inherent risk of selection bias. Second, the fact that not all COVID-19 inpatients underwent sputum bacterial culture may have introduced statistical bias into the dataset. Third, our failure to systematically screen for co-infections with other viral pathogens, particularly Epstein-Barr virus (EBV) and other common respiratory viruses, prevents us from ruling out their potential confounding effects on the clinical outcomes and disease severity observed in our cohort. Fourth, the symptom-driven sampling strategy employed in this study, while reflecting real-world clinical practice, may have resulted in underdetection of subclinical infections or asymptomatic colonization, particularly in the mild case group; additionally, some degree of subjectivity may have been introduced in the sampling decisions due to potential inter-physician variation in the assessment of clinical indications. Nevertheless, we believe our findings provide valuable and representative insights into the real-world scenario of bacterial co-infections in COVID-19 patients in the Shaanxi region.