
Sepsis is the leading cause of admission to intensive care and high dependency units, and its incidence continues to rise worldwide [1]. Several biomarkers reflecting the presence and intensity of inflammation are used to assess the severity of sepsis syndrome. As treatment strategies should be tailored to the individual, identifying patients at high risk of death is a critical step toward personalized management. However, an ideal biomarker for sepsis remains to be established. Such a biomarker should offer high accuracy in the early detection of sepsis and strong predictive value for the disease severity and clinical outcomes.
Pancreatic Stone Protein (PSP) is an acute-phase protein, acting as a pro-inflammatory mediator by binding to polymorphonuclear cells and triggering their activation in vitro. It has emerged as a novel biomarker with potential applications in diverse clinical settings. Notably, its pronounced elevation during septic episodes has prompted investigation in Intensive Care Unit (ICU) and Emergency Department (ED) populations, where early studies have reported encouraging results [2,3].
As a point-of-care test, it can predict unfavorable outcomes including bacteremia in patients with suspected infection, sepsis and need of antibiotic treatment escalation in intra-abdominal infection patients and increased Length of Hospital Stay in COVID-19 patients [4,5,6].
Beyond its role as an inflammatory biomarker, PSP has also been identified as a damage-associated molecular pattern (DAMP) released by stressed or injured pancreatic acinar cells. Upon release, PSP acts as a danger signal, amplifying local and systemic inflammation through activation of innate immune pathways and modulation of neutrophil responses [7]. This mechanistic insight underscores its potential role in linking tissue injury with the immune dysregulation characteristic of sepsis.
Despite these promising findings, evidence regarding PSP's prognostic value in community-acquired infections (CAIs) remains limited. This study aimed to evaluate the association between PSP levels at ED admission and LOS in adults with CAIs, including lower respiratory tract infections (LRTIs), urinary tract infections (UTIs), and intra-abdominal infections (IAIs).
This prospective observational study included 101 patients admitted to the Emergency Department (ED) of the University Hospital of Patras between March 2024 and December 2024. Eligible participants were aged ≥18 years and presented with signs and symptoms consistent with lower respiratory tract infection (LRTI), urinary tract infection (UTI), or intra-abdominal infection (IAI), as defined by the Infectious Diseases Society of America (IDSA).
Patients were excluded if they met any of the following criteria: (i) complicated co-infections on admission (endocarditis, central nervous system infections, septic arthritis, osteomyelitis, or polymicrobial infections); (ii) hospitalization or receipt of antibiotic treatment within the previous month; (iii) isolation of extended-drug resistant (XDR) or pan-drug resistant (PDR) microorganisms in the first culture (iv) severe immunocompromise, including neutropenia with <1000 polymorphonuclear cells (PMNs) or hematological malignancy (v) history of chronic pancreatitis, pancreatic surgery at any time, or abdominal surgery within the last 12 months (vi) for UTI, anatomical abnormalities of the urinary tract (vii) for respiratory tract infection, history of thoracic surgery, pulmonary or bronchial mass, or pulmonary fibrosis (viii) for IAI, history of peptic cancer.
PSP levels were measured within one hour upon ED admission using a quantitative point-of-care diagnostic capsule and a desktop spectrophotometer device (abioSCOPE). The system uses nanofluidic immunoassay technology to quantify PSP concentrations from a venous whole blood sample (5 μL), providing results within approximately 7 minutes.
We selected the threshold value of 50 ng/mL for PSP based on findings from our previous study, in which the optimal cut-off value of PSP for predicting prolonged hospitalization, determined using the Youden Index, was 51 ng/mL, with a sensitivity of 65% and a specificity of 91.3% [6].
The study was conducted in accordance with the International Conference on Harmonization (ICH) E6 guidelines for Good Clinical Practice, the Declaration of Helsinki, and all applicable local regulations. Ethical approval was obtained from the institutional review board and local ethics committee of the University Hospital of Patras (Approval No. 679/19.12.2023). A written inform consent was obtained from all participants.
All statistical analysis was performed using the IBM® SPSS® Statistic v.26 software. Normally distributed data is presented as mean ± standard deviation (SD). Spearman rank correlation coefficient (ρ) was used to assess the relationship between PSP and LOS. A p < 0.05 was considered statistically significant. A multiple linear regression analysis was performed to evaluate the association between patients' demographic and clinical characteristics, and the length of hospital stay (LOS). The independent variables included age, sex, type of infection, and pancreatic stone protein (PSP) levels.
A total of 101 patients were included in the study, with a mean age of 66.7 ± 20.8 years old. The majority were female (n = 56, 55.4%), while 45 patients (44.6%) were male. The most frequent site of infection was respiratory tract infection (RTI), observed in 53 patients (52.5%). The baseline demographic and clinical characteristics of the study population are summarized in Table 1.
Summary of demographic characteristics
| Parameter Group | Characteristic | Value |
|---|---|---|
| Demographics | Mean age ± SD | 66.7 ± 20.8 years |
| Sex: male / female | 44.6% / 55.4% | |
| Primary infection site(n) | Lower respiratory tract infections | 47.4% (54) |
| Urinary tract infections | 34.2% (39) | |
| Intra-abdominal infections | 18.4 % (21) | |
| Inflammatory biomarkers | Lactate (mmol/L) | 1.8 ± 2.8 |
| C-reactive protein (CRP, mg/dL) | 11.7 ± 2.7 | |
| High-sensitivity troponin I (ng/L) | 101.2 (10.2–2016.6) | |
| Median (min–max) | ||
| 435 (16–2593) | |
| Fibrinogen | 509.6±219.9 | |
| White blood count (K/μL) | 15910.2±3910.8 | |
| Comorbidities | Diabetes mellitus | 27% |
| Hypertension | 33% | |
| Cardiovascular disease | 17% | |
| Dyslipidemia | 28% | |
| Chronic kidney disease | 2% | |
| Cancer | 7% |
Abbreviations: LRTI: lower respiratory tract infections, UTI: urinary tract infections, CRP: C-reactive protein
Elevated PSP levels showed a statistically significant low-to-moderate positive correlation with prolonged LOS (Spearman's ρ = 0.369, p < 0.001). Using an optimal cut-off of 50 ng/ml, patients with PSP < 50 ng/ml had a median LOS of 4 days (95% CI: 3–5), while those with PSP ≥ 50 ng/ml had a median LOS of 9 days (95% CI: 6–13).
The multiple linear regression model showed a statistically significant overall fit (F = 4.54, p = 0.002), accounting for approximately 16% of the variance in the length of hospital stay (R2 = 0.159). Among the variables included, only PSP levels were significantly associated with prolonged hospitalization (β = 0.041, p < 0.001), indicating that higher PSP values were linked to longer hospital stays. Conversely, age, sex, and infection type did not exhibit significant associations. These results suggest that PSP could represent an independent marker of disease severity, and a useful predictor of hospital stay duration.
Receiver Operating Characteristic (ROC) curve analysis assessed the prognostic accuracy of various biomarkers for predicting prolonged hospital stay (> 9 days). PSP had the highest discriminative ability with an AUC of 0.910, followed by CRP (0.778) and WBC (0.743). Other biomarkers such as fibrinogen (0.708), hs-troponin I (0.597), lactate (0.556), and ferritin (0.479) showed poorer predictive performance, with ferritin and lactate near chance levels (AUC ~0.5). [Figure 1, Table 2].
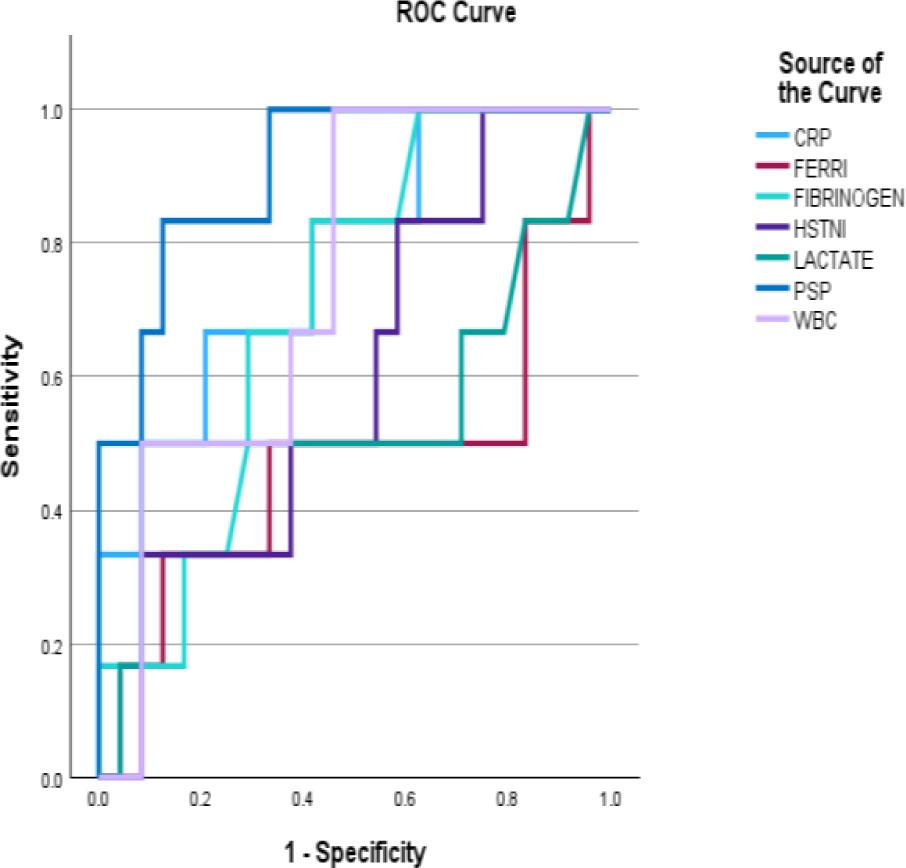
ROC analysis of C-reactive protein, hs-Troponin I (HSTNI), lactate, pancreatic stone protein, fibrinogen, ferritin and White Blood cells (WBC) on length of hospitalization of patients with community acquired infections.
ROC curve analysis for biomarkers predicting prolonged length of stay (>9 days)
| Biomarker | AUC | 95% CI | Sensitivity (%) | Specificity (%) | Threshold value |
|---|---|---|---|---|---|
| Pancreatic Stone Protein (PSP) | 0.910 | 0.851–0.970 | 86.5 | 87.3 | 76 ng/mL |
| C-Reactive Protein (CRP) | 0.778 | 0.678–0.878 | 69.2 | 79.3 | 25.9 mg/l |
| White Blood Cell count (WBC) | 0.743 | 0.635–0.850 | 63.5 | 75.0 | 8.84 ×103/L |
| Lactate | 0.726 | 0.620–0.832 | 61.5 | 72.6 | 2.20 mmol/L |
| Fibrinogen | 0.687 | 0.578–0.796 | 59.6 | 68.4 | 511 mg/dL |
| Ferritin | 0.655 | 0.540–0.770 | 55.8 | 65.3 | 1048 ng/mL |
Pancreatic stone protein belongs to the family of lectin-binding proteins and is constitutively secreted by pancreatic acinar cells into pancreatic juice alongside other enzymes (zymogens). As an acute-phase protein, PSP may contribute to promoting cell proliferation during tissue regeneration, a process regulated by IL-6 and other cytokines released following injury and stress. This supports the concept described by Reding et al., who referred to the pancreas as “an acute-phase organ” [1,8]. PSP has been studied and compared to other biomarkers across various infectious and septic conditions, both as a diagnostic marker and as a prognostic indicator of outcomes [5,9].
Our findings demonstrate a significant correlation between PSP levels measured upon Emergency Department admission and length of hospital stay in patients with community-acquired infections. PSP measured within one hour of ED admission could serve as an effective biomarker to identify patients at high risk for prolonged hospitalization, reflecting more severe disease. In the present study, a PSP cut-off of 50 ng/dl effectively discriminated against patients with significantly longer hospital stays. Furthermore, PSP offers advantages over traditional markers (e.g., CRP, procalcitonin, lactate) due to its rapid point-of-care measurement and its specificity in detecting infectious stress, particularly in the early inflammatory phase [10,11].
Regarding prediction of hospitalization length, PSP outperformed other measured acute-phase proteins, achieving a relatively high AUC. These results are consistent with previous studies indicating PSP as a reliable early biomarker of prolonged hospitalization, including cohorts of COVID-19 patients. A previous study reported that PSP effectively identifies COVID-19 patients at high risk for extended hospitalization, with an AUC of 0.800 [6]. PSP could therefore be incorporated into triage protocols to guide resource allocation and early therapeutic interventions, potentially improving outcomes and reducing LOS [12].
Moreover, the ROC analysis in our study underscores PSP's strong prognostic value for identifying patients at risk of prolonged hospitalization due to CAI. With an AUC of 0.910, PSP demonstrated excellent discriminative performance, substantially outperforming traditional inflammatory markers such as CRP and WBC, as well as other acute-phase proteins like fibrinogen and ferritin. These findings align with evidence from broader infection and sepsis studies. For example, Prazak et al. reported that PSP demonstrated superior diagnostic and prognostic accuracy compared to CRP or PCT, with AUC values ranging from 0.84 to 0.90, while a combined model including CRP revealed an AUC of 0.90 (0.87–0.92) [13]. Such data reinforces PSP's clinical utility as an early, point-of-care biomarker for risk stratification, enabling clinicians to anticipate resource needs and optimize patient management since ED presentation.
Our study has limitations that warrant consideration. First, it was conducted at a single tertiary care center, which may limit generalizability to other healthcare settings or patient populations. Second, the sample size was relatively small; although the association between PSP levels and LOS was statistically significant, larger multicenter studies are needed to confirm these findings and establish more precise cut-off values. Third, despite excluding patients with conditions known to influence PSP levels, residual confounding from unmeasured variables – such as comorbidity burden or differences in treatment strategies – cannot be ruled out. Moreover, the definition of a hospital stay longer than 9 days as prolonged hospitalization was established empirically. Another limitation is the lack of comparison with procalcitonin, as this biomarker is not measured in our hospital. Finally, as an observational study, causality between elevated PSP levels and prolonged hospital stay cannot be established.
In conclusion, PSP appears to be a valuable, rapid point-of-care biomarker and a useful tool for risk stratification in patients with community-acquired infections admitted to the ED. Its potential use, either alone or combined with other prognostic biomarkers, is encouraging.