
In acute myocardial infarction patients, parameters of right ventricular systolic function such as 2D TAPSE, S’
Echocardiographic assessment after acute myocardial infarction (AMI) focuses on left ventricular (LV) systolic function, given its prognostic significance and importance in guiding selection of appropriate therapies in these patients. [1] Right ventricular involvement is, however, frequently encountered in AMI patients. [2] Although frequently overlooked in this context, RV dysfunction has been shown to be a significant independent predictor of outcome, including arrythmias, in-hospital mortality, long-term mortality, and risk of developing heart failure. [3,4,5,6,7,8,9,10,11]
Routine evaluation of RV systolic function is done by measurement by 2D echocardiography (2DE) of tricuspid annular plane systolic excursion (TAPSE), right ventricular systolic wave velocity (S’
Although all of the aforementioned 2DE parameters have been shown to have prognostic significance in the context of AMI [3,6,15,16], recent data suggested that cut-off values for these parameters are only modestly associated with results obtained by 3D RVEF, resulting in significant misclassification of patients, depending on the parameter used and underlying pathology. [17] Furthermore, patients that had initially been found to have normal values of standard parameters but were subsequently reclassified as having RV dysfunction by 3D RVEF, had a 4-fold increase in mortality risk. [17]
Thus, our objective was to analyse reproducibility of assessment of RV systolic function by TAPSE, S’
This was a single-center, prospective, observational study, that included patients hospitalized with AMI. All patients underwent coronary angiography and treatment, complying with the current European Society of Cardiology guidelines. [18,19] Local Ethics Committee approved the study protocol (Approval No. 14463/12.06.2018), while written informed consent for study participation was obtained before inclusion, during the first 24 hours of hospitalization.
The following inclusion criteria were used: (1) patients aged >18 years-old who signed an informed consent; (2) patients diagnosed with AMI according to the Fourth Universal Definition of Acute Myocardial Infarction; [20] (3) patients with sufficient image quality to perform 2DE and 3DE analysis (clear visualization of RV endocardium and tricuspid valve, lack of stitching artifacts). The exclusion criteria were: (1) patients with a history of heart failure (HF) or any documented LV (defined as LVEF<50%) or RV dysfunction (defined as TAPSE < 17mm, FAC < 35%, S’
Demographic and clinical data were retrieved from the clinical records obtained during hospitalization.
Image acquisition was performed by the advanced echocardiographer with at least 5 years of training in 2DE and 3 years of training in 3DE. All examinations were performed within 48 hours of admission, using a state-of-the-art ultrasound system (Vivid E90 or Vivid E95 – GE Vingmed Ultrasound, Horten, Norway). Two-dimensional acquisitions were done using a M5 S probe, while a 4Vc-D probe was used for 3DE acquisition.
In accordance with current guidelines, image datasets were obtained using ECG-gated apical views optimised for the right ventricle. [12,13] Datasets of 2D images were digitally stored in raw-data format and analysed offline using commercially available dedicated software (EchoPAC version 203, GE Vingmed, Horten, Norway). Tricuspid annular plane systolic excursion (TAPSE) was obtained analysing M-mode acquisition with the cursor placed on the lateral tricuspid annulus in the A4C view optimised for the RV. Fractional area change (FAC) was calculated using ECG-gated end-diastolic and end-systolic area values obtained from A4C view optimised for the RV. Right ventricular systolic wave velocity (S’
Three-dimensional datasets analysis was carried out offline, using semiautomated, commercially available software packages (4D Auto RV Quantification tool, EchoPAC version 203, GE Vingmed, Horten, Norway). Full volume 3D datasets were reconstructed using ECG gating from sequences of 6 cardiac cycles. Images were obtained using breath-hold techniques to avoid stiching artifacts. [13] The semi-automated tool used for 3D reconstruction required manual placement of a vertical axis through the center of the tricuspid valve and the RV apex, respectively. Points of interest were placed at the medial and lateral borders of the tricuspid annulus and at the RV apex. Subsequently, a multislice model showing endocardial border delineation at end-diastole and end-systole was displayed where manual corrections were performed to ensure accurate endocardial tracing. End-diastolic and end-systolic volumes were then automatically calculated by the software and provided together with a time-volume curve, 3D RVEF and other volumetric parameters values.
Measurements were done by three echocardiographers with different levels of expertise: advanced – labelled as Reader 1 (R1), with 5 years of experience in 2DE and 3 years of experience in 3DE, was also the one that carried out image acquisition; intermediate – labelled as Reader 2 (R2), with 3 years of training in 2DE and 1 year of training in 3DE; beginner – labelled as Reader 3 (R3), with one year of training in 2DE and 3 months of training in 3DE. All measurements were independently performed in a blinded fashion on the same echocardiographic images. The sequence of reading was the following: Reader 1 conducted the initial assessment followed by Reader 2 and, finally, Reader 3.
Statistical analysis was performed using SPSS (ver. 26, IBM Corporation, Armonk, USA) and Microsoft Excel (ver. 2503, Microsoft Corporation, Redmond, USA). Continuous variables are expressed in mean ± SD, while categorical variables are presented as absolute numbers and percentages. Bland-Altman method was used to assess inter-observer variability and agreements by quantifying their mean difference (bias). Limits of agreement (LOA) were expressed as the mean difference ± 1.96*SD, thus defining the range within which 95% of individual differences are expected to lie. Agreements between measurements were assessed by Pearson’s correlation coefficients with an R-value of >0.80 considered a very good correlation, and p-value <0.05 considered statistically significant. Intraclass correlation coefficients were quantified by the 2-way random effects with absolute agreement for multiple raters. ICC values were considered as follows: <0.5 was considered poor, 0.5 ≤ ICC < 0.75 was considered moderate, 0.75 ≤ ICC < 0.90 was considered good and a value ≥0.90 was considered excellent.
Between December 2019 and June 2022, a total of 63 Caucasian patients were included. Study population consisted mainly of male patients (n = 52, 82.5%) with a mean age of 56.8 ± 10.3 years; Patient characteristics are presented in Table 1.
Demographic and clinical characteristics
| 20 | Total (n=63) |
| Demographic characteristics | |
| Age, years | 56.86 ± 10.3 |
| Male, n (%) | 52 (82.5) |
| BMI, kg/m2 | 28.57 ± 3.14 |
| BSA, m2 | 1.98 ± 0.21 |
| AMI type and revascularization | |
| ST-segment elevation myocardial infarction, n (%) | 43 (68.3) |
| Percutaneous coronary intervention, n (%) | 54 (85.7) |
| Risk factors and medical history | |
| History of smoking, n (%) | 38 (60.3) |
| Diabetes, n (%) | 16 (25.4) |
| Hypertension, n (%) | 44 (69.9) |
| Obesity, n (%) | 21 (33.3) |
| Dyslipidaemia, n (%) | 61 (96.8) |
| Peripheral artery disease, n (%) | 1 (1.6) |
| Chronic kidney disease, n (%) | 17 (27.0) |
Abbreviations: AMI – acute myocardial infarction, BMI – body mass index, BSA – body surface area
Bland-Altman plots showed a bias of 0.24 (95% CI: −0.08;0.55) between the advanced and intermediate readers, with LOA of −2.27 (95%CI −2.82;−2.27) to 2.75 (95%CI 2.2;3.29); 0.38 (95% CI: 0.09;0.76) between the advanced and beginner readers, with LOA of −1.9 (95% CI −2.45;−1.94) to 2.7 (95% CI 2.19;3.21); and 0.14 (95% CI −0.17;0.46) between the intermediate and beginner readers, with LOA of −2.37 (95% CI −2.92;−2.37) to 2.65 (95% CI 2.11−3.2) (Figure 1.A). All Pearson correlations were good (R1 vs R2: r=0.93, p<0.001; R1 vs R3: r=0.94, p<0.001; R2 vs R3: r=0.93, p<0.001) (Figure 1.B). ICC was excellent with a value of 0.977 (95% CI: 0.965−0.985).
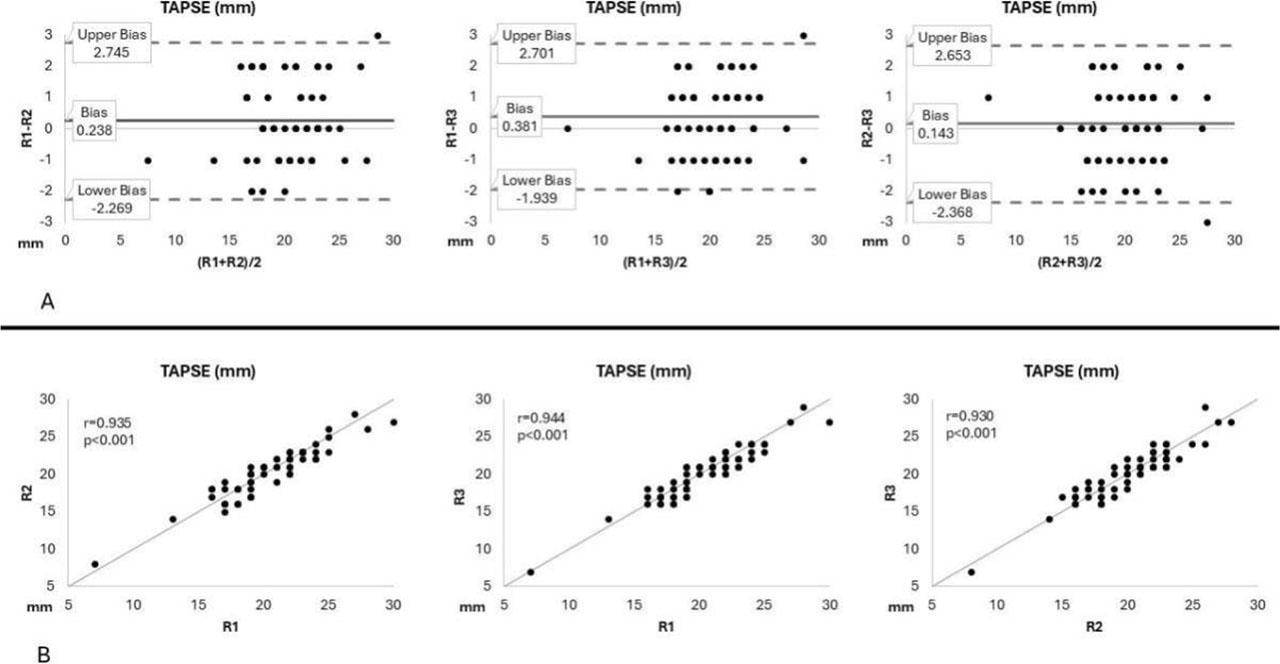
Bland-Altman plots (panel A) and correlations (panel B) for measurements of tricuspid annular plane systolic excursion (TAPSE) by advanced (R1), intermediate (R2), and beginner (R3) readers.
Bland-Altman plots showed a bias of 0.19 (95% CI 0;0.38) between the advanced and intermediate readers, with LOA of −1.3 (95% CI −1.62;−1.3) to 1.7 (95% CI 1.35;2); 0.37 (95% CI 0.11;0.62) between the advanced and beginner readers, with LOA of −1.64 (95% CI −2.07;−1.64) to 2.37 (95% CI 1.93;2.8); and 0.17 (95% CI −0.13;0.48) between the intermediate and beginner readers, with LOA of −2.25 (95% CI −2.78;−2.25) to 2.6 (95% CI 2.07;3.13) (Figure 2.A). All Pearson correlations were good (R1 vs R2: r=0.96, p<0.001; R1 vs R3: r=0.90, p<0.001; R2 vs R3: r=0.88, p<0.001) (Figure 2.B). ICC 0.967 (95% CI: 0.95–0.98) also showed excellent reproducibility.
Bland-Altman plots showed a bias of 0.36 (95%CI −0.3;1.02) between the advanced and intermediate readers, with LOA of −4.9 (95% CI −6.05;−4.9) to 5.62 (95% CI 4.47;6.77); 0.09 (95% CI −0.73;0.91) between the advanced and beginner readers, with LOA of −6.44 (95% CI −7.86;−6.44) to 6.6 (95% CI 5.19;8.04); and −0.27 (95% CI −1.25;0.71) between the intermediate and beginner readers, with LOA of −8.07 (95% CI −9.77;−8.07) to 7.53 (95% CI 5.83;9.23) (Figure 3.A). All Pearson correlations were good (R1 vs R2: r=0.96, p<0.001; R1 vs R3: r=0.94, p<0.001; R2 vs R3 r=0.91, p<0.001) (Figure 3.B). ICC value was 0.98 (95% CI: 0.97–0.99) showing excellent correlation.
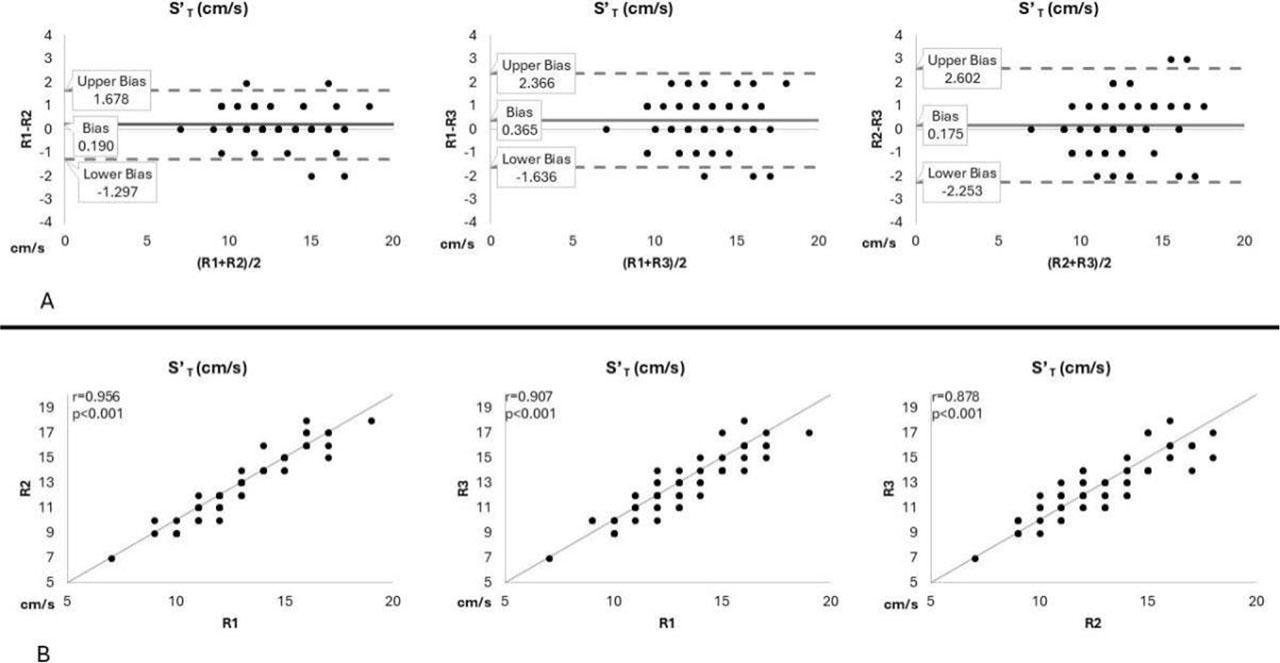
Bland-Altman plots (panel A) and correlations (panel B) for measurements of right ventricular systolic wave velocity (S’
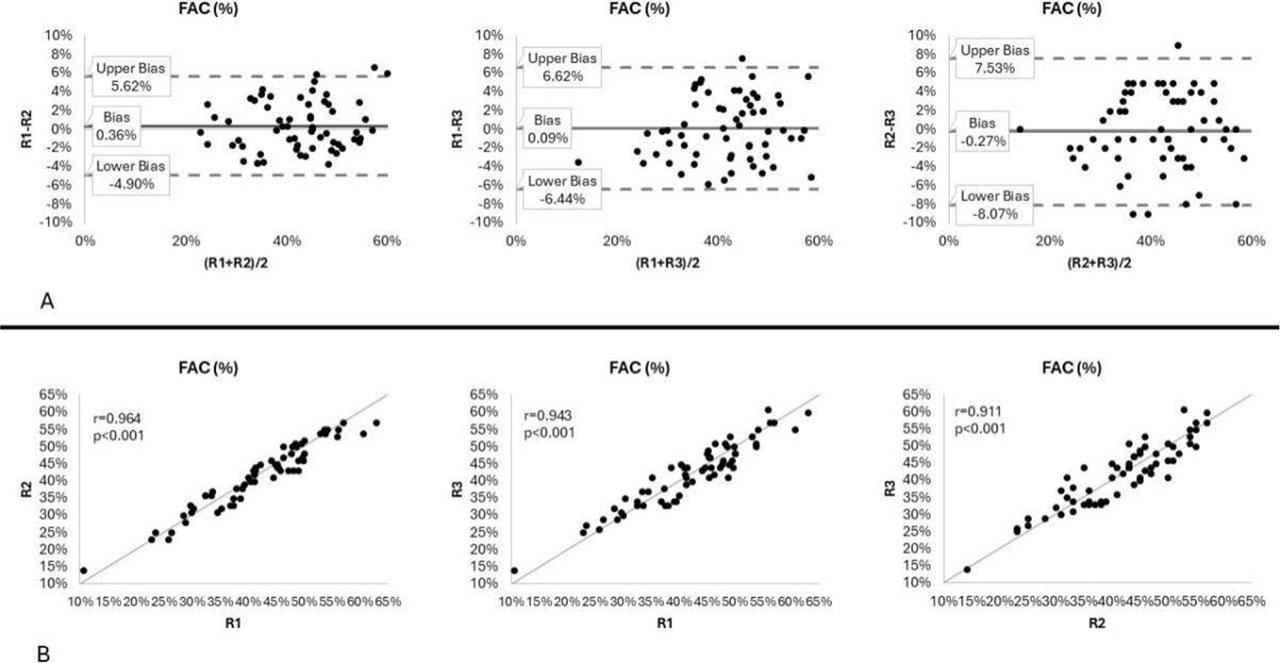
Bland-Altman plots (panel A) and correlations (panel B) for measurements of fractional area change (FAC) by advanced (R1), intermediate (R2), and beginner (R3) readers.
Bland-Altman plots showed a bias of −0.02 (95% CI −0.64;0.60) between the advanced and intermediate readers, with LOA of −4.96 (95% CI −6.03;−4.96) to 4.91 (95% CI 3.84;5.99); −0.38 (95%CI −1.15;0.39) between the advanced and beginner readers, with LOA of −6.48 (95% CI −7.81;−6.48) to 5.72 (95% CI 4.39;7.05); and −0.36 (95% CI −1.01;0.3) between the intermediate and beginner readers, with LOA of −5.57 (95% CI −6.70;−5.57) to 4.85 (95% CI 3.72;5.99) (Figure 4.A). All Pearson correlations were good (R1 vs R2: r=0.96, p<0.001; R1 vs R3: r=0.93, p<0.001; R2 vs R3 r=0.94, p<0.001) (Figure 4.B). ICC value was 0.98 (95% CI: 0.97–0.99).
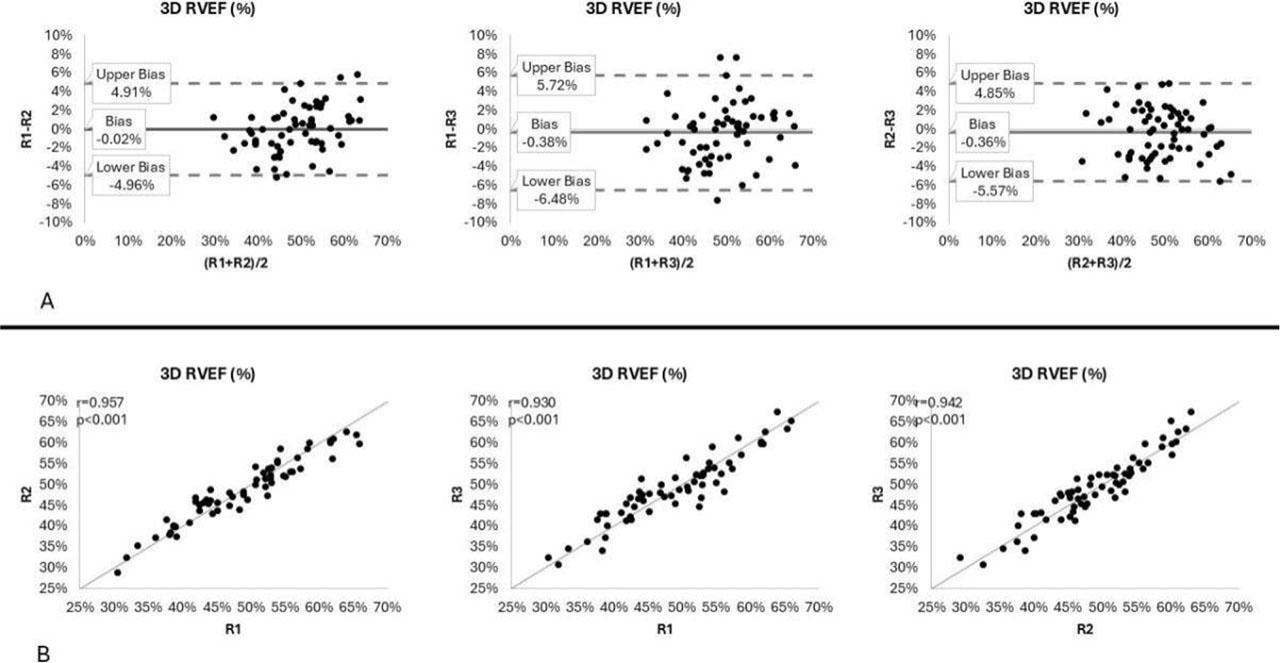
Bland-Altman plots (panel A) and correlations (panel B) for measurements of 3D Right ventricular ejection fraction (3D RVEF) by advanced (R1), intermediate (R2), and beginner (R3) readers.
Comparative values of interobserver variability and agreement are provided in Table 2.
Interobserver variability and agreement between echocardiographers with different levels of experience for TAPSE, S’
| R1 vs R2 | TAPSE | S’ | FAC | 3D RVEF |
| Bias (95% CI) | 0.24 (−0.08:0.55) | 0.19 (0.0;0.38) | 0.36 (−0.3;1.02) | −0.02 (−0.64;0.6) |
| Lower LOA (95% CI) | −2.27 (−2.82; −2.27) | −1.3 (−1.62;−1.3) | −4.9 (−6.05;−4.9) | −4.96 (−6.03;−4.96) |
| Upper LOA (95% CI) | 2.75 (2.20;3.29) | 1.68 (1.35;2.0) | 5.62 (4.47;6.77) | 4.91 (3.84;5.99) |
| R1 vs R3 | TAPSE | S’ | FAC | 3D RVEF |
| Bias (95% CI) | 0.38 (0.09;0.67) | 0.36 (0.11;0.62) | 0.09 (−0.73;0.91) | −0.38 (−1.15;0.39) |
| Lower LOA (95% CI) | −1.94 (−2.45;−1.94) | −1.64 (−2.07;−1.64) | −6.44 (−7.86;−6.44) | −6.48 (−7.81;6.48) |
| Upper LOA (95% CI) | 2.7 (2.19;3.21) | 2.37 (1.93;2.80) | 6.62 (5.19;8.04) | 5.72 (4.39;7.05) |
| R2 vs R3 | TAPSE | S’ | FAC | 3D RVEF |
| Bias (95% CI) | 0.14 (−0.17;0.46) | 0.17 (−0.13;0.48) | −0.27 (−1.25;0.71) | 0.36 (−1.01;0.3) |
| Lower LOA (95% CI) | −2.37 (−2.92;−2.37) | −2.25 (−2.78;−2.25) | −8.07 (−9.77;−8.07) | −5.57 (−6.7;−5.57) |
| Upper LOA (95% CI) | 2.65 (2.11;3.2) | 2.60 (2.07;3.13) | 7.53 (5.83;9.23) | 4.85 (3.72;5.99) |
| ICC (95% CI) | 0.977 (0.965–0.985) | 0.967 (0.95–0.98) | 0.98 (0.97–0.99) | 0.98 (0.97–0.99) |
Abbreviations: 3D RVEF – three-dimensional right ventricular ejection fraction, FAC – fractional area change, ICC – intraclass correlation coefficient, LOA – limits of agreement, TAPSE – tricuspid annular plane systolic excursion, S’
Currently, 2DE is the most widely used method to assess RV systolic function in clinical practice. All three parameters used in this study have previously been shown to have good correlations with other imaging methods. TAPSE has been shown to have a strong correlation with RVEF obtained by CMR [21] and radionuclide angiography [22], FAC displayed strong correlation with RVEF values obtained by CMR [23], while S’
3DE assessment of right ventricular function by 3D RVEF has recently emerged as an alternative to 2DE methods, being extensively validated with CMR measurements, with correlation coefficients R>0.75 in most studies. [30] 3D RVEF measurements are highly reproducible, with low intra- and inter-observer variability varying from 0 to 0.9% in most studies. [30,31,32,33,34,35] A frequently cited limitation is operator experience, but recent studies have addressed this issue, showing that 3DE quantification provides good reproducibility even in novice operators. [35,36,37]. Our study also demonstrated very good values of reproducibility that are similar to those found for 2DE parameters. Moreover, bias between the advanced and intermediate user was the lowest in the entire study, while bias when comparing with the beginner operators were similar to the 2DE parameters. Thus, although 3D RVEF assessment exhibits a learning curve, our study suggests that it is highly reproducible among operators with different levels of experience when image acquisition is carried out by an advanced operator.
The current study has a series of limitations that must be acknowledged. These are related mostly to the inherent limitations of 3D echocardiography. Image quality is essential for 3D RVEF assessment, but also FAC. Image acquisition was carried out only by the advanced echocardiographer, and caution should be taken in considering that these results can be extended to a scenario in which acquisition is made by multiple operators with different levels of expertise. However, it is a common scenario in institutions that image acquisition is carried out by an experienced practicioner, followed by offline analysis by operators with different levels of expertise. Further analysis in this direction is warranted to clarify our better understanding of feasibility and reproducibility of 3DE RVEF assessment when image acquisition is carried out by less experienced operators. Patients with history of heart failure, documented LV or RV dysfunction, atrial fibrillation, significant valvular disease and pulmonary hypertension were excluded from our study. Multi-beat full-volume acquisition remains the recommended method for obtaining adequate temporal resolution, and highly irregular rhythms such as atrial fibrillation can generate significant artifacts. [13,38] Pre-existing ventricular dysfunction, valvular disease and pulmonary hypertension can result in significantly enlarged and deformed RVs that can also lead to poor image quality. [38] As such, our findings cannot be extended to these categories of patients. Finally, our study did not include patients evaluated by CMR, which remains the gold standard of RV quantification. However, CMR is currently not widely available for all patients in everyday clinical use due to its costs, non-portable nature and significant patient-related contraindications. Moreover, our study was focused on reproducibility of echocardiographic parameters of RV systolic function that have all been previously validated by CMR.
Our study demonstrates that both 2DE, as well as more advanced 3DE parameters of right ventricular systolic function, are highly reproducible, and independent of operator experience when image acquisition is carried out by an advanced echocardiographer. Our findings support the use of these methods in current clinical practice in patients with AMI, in cases when CMR is not available, given that RV function assessment has been shown to provide supplemental prognostic value in addition to standard evaluation of left ventricular function.