
The mortality rate exposed in patients with ST-segment elevation myocardial infarction is attributable to the development of short- and long-term complications [1,2]. Association with the no-reflow phenomenon presents a negative prognosis [3], because the 5-year survival rate is much lower compared to subjects without the phenomenon [4,5].
The incidence of no-reflow phenomenon [6] in STEMI patients [7] undergoing primary PCI is 2.3% [8]. Diagnosis criteria represent crucial elements in identifying the phenomenon since angiographic elements defined as TIMI flow rate and myocardial “blush” ≤ 2 [9] may be associated with underdiagnosis of the complication. However, this rate may increase significantly [10] if other paraclinical parameters, such as persistence of ST-segment elevation on the ECG pathway ≥50% of baseline after percutaneous coronary myocardial revascularization [4,11] are considered.
The no-reflow phenomenon is caused by the lack of blood flow in the coronary microcirculation, despite optimal blood flow restoration using the PCI procedure in coronary arteries responsible for myocardial infarction [12].
Patients with STEMI referred for percutaneous myocardial revascularization intervention may experience multiple complications [13,14]. In the short term, they may present malignant rhythm disturbances [15] or even cardiogenic shock that results when there is cardiac dysfunction accompanied by tissue hypoperfusion [15,16], triggers for the future no-reflow phenomenon. Myocardial rupture is the most feared complication because it involves the death of the patient if emergency surgical correction doesn’t occur quickly [17,18]. In time, patients suffering from acute myocardial infarction may present loss of viability of the myocardial mass, leading to remodeling of the left ventricle, which has consequences on changing ventricular geometry and a decrease in systolic function [19,20]. Due to myocardial remodeling, patients who develop no-reflow phenomenon may progress to left ventricular failure with a long-term negative prognosis. [21,6]
Following acute myocardial infarction with obstruction of the epicardial coronary artery, changes also involve the microcirculation [22]. Thus, ischemic myocytes, together with those in myocardial necrosis, may develop interstitial edema due to compression exerted by blood capillaries [23]. This process also triggers the edematous endothelial cells [24,25] that interact with numerous red blood cells, platelets, or even fibrin, causing embolization and capillary lumen obstruction [26]. Leukocytes participate actively [27,4] in the obstruction of coronary microcirculation by activation and phagocytosis of the necrotic area. The process involves secretion of free radicals, leukotrienes, and proteolytic enzymes that play a role in endothelial dysfunction [28,4]. Also, platelets are involved because they generate clots or emboli due to fragmentation, causing obstruction of the epicardial coronary artery [29,4].
Endothelial dysfunction of coronary microcirculation is a dynamic process induced by vasoconstriction through adrenergic hypertonia [30] and contraction of the smooth muscle cells of the blood vessels, promoting ischemia [31] (Figure 1).
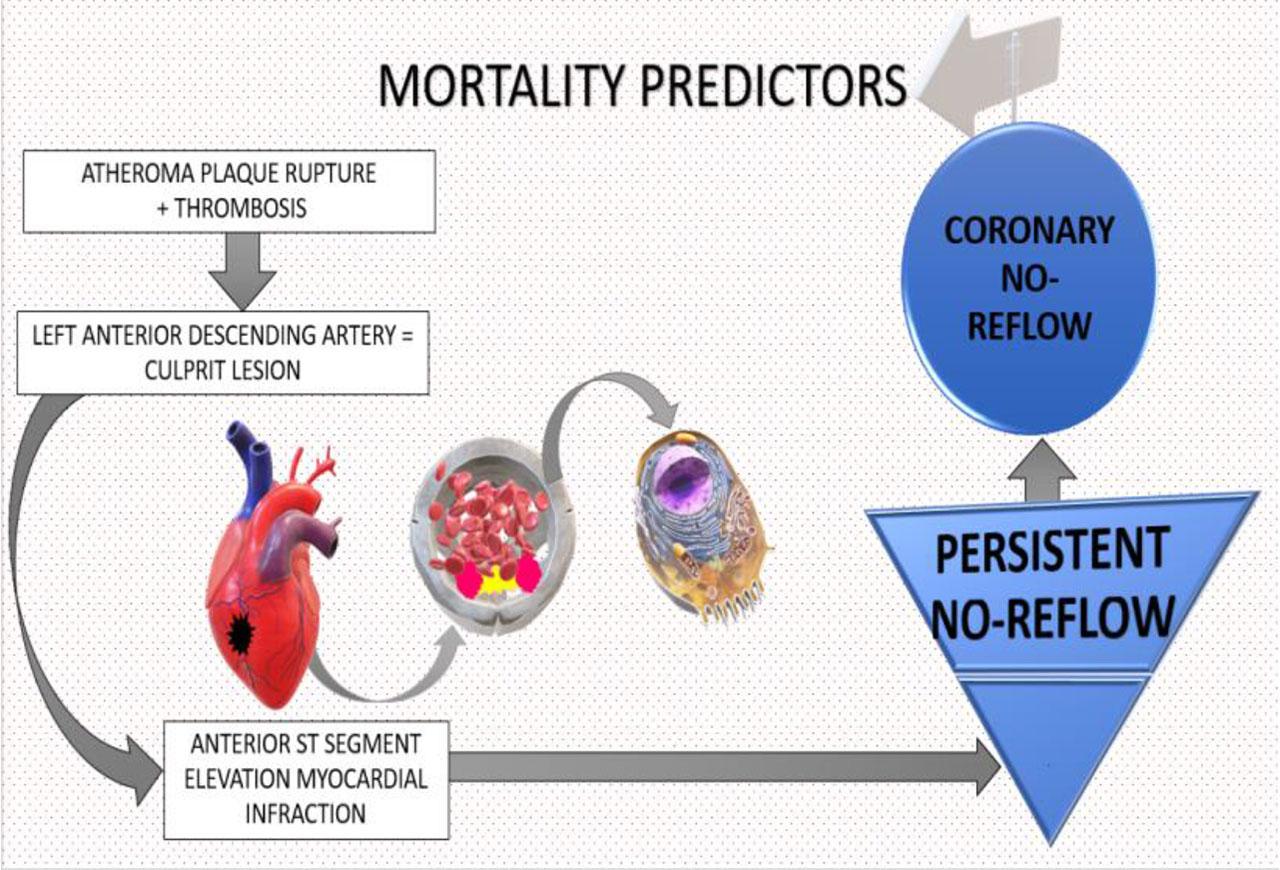
Graphical abstract revealing the pathophysiology of atherosclerosis and mortality predictors in STEMI subjects with no-reflow phenomenon.
Data from literature [32,33] reveal an important aspect in no-reflow phenomenon incidence, consisting in the choice of contrast substance used during the percutaneous interventional revascularization procedure [34], indicating that some may induce the appearance of a dense fibrin network that impairs myocardial reperfusion [4].
Our study aims to illustrate the mortality rate and prognosis predictors in patients with STEMI who develop no-reflow phenomenon after primary PCI.
Between 01.01.2016 – 31.03.2018, we performed a prospective study including 656 patients who had STEMI. We only included patients who had undergone myocardial revascularization through the primary PCI method and developed the no-reflow phenomenon. The Ethics Committee of Emergency Clinical County Hospital Bihor approved the study (21806), and the study adheres to the principles mentioned in the Declaration of Helsinki.
The group included in the research was clinically evaluated, and several parameters were noted (sex, age, STEMI characteristics, and type of no-reflow phenomenon, complications). The diagnosis of STEMI was established according to current guidelines [35].
Electrocardiography was performed using the 12-channel BTL-08 MT Plus electrocardiograph. From the blood test, we considered relevant myocardial necrosis enzymes, which were detected using the ARCHC4000 using the spectrophotometric method.
The angiography was performed using the Philips Tiam FD 10 device, and the procedure was able to detect the no-reflow phenomenon. The presence of no-reflow coronary phenomenon was noted when both the TIMI flow rate and myocardial “blush” grade were ≤ 2. A myocardial no-reflow phenomenon was defined by persistence of ST segment elevation on ECG more than 50–70% from the initial value associated with optimum blood flow evaluated through coronary angiography and good “blush” degree. We only considered for our study the deaths recorded during the hospitalization period.
Patients were categorized as having coronary or myocardial no-reflow based on angiographic findings and ECG changes, following previously published definitions. Coronary no-reflow was identified by reduced or absent antegrade flow (TIMI flow ≤2) despite successful mechanical reperfusion and no significant residual stenosis. Myocardial no-reflow was inferred in patients with restored coronary flow (TIMI 3) but persistent ST-segment elevation ≥50% at 60–90 minutes post-PCI, suggestive of impaired myocardial perfusion. While we acknowledge the limitations of using ECG as an indirect tool, it remains a widely accessible clinical surrogate in the absence of advanced perfusion imaging.
From all 14 deaths registered in our study lot with STEMI and no-reflow phenomenon after primary PCI, only 5 were autopsied. The others were exempted from autopsy by their caregivers. All autopsies were performed in the Pathology Department according to the hospital protocol. The procedure was realized within 24 hours and was recommended especially for cases without forensic issues. The auricle was dissected using bread loaf slicing technique because it reveals more clearly the myocardial infarction localization and the evolution of morphologic elements associated with myocardial ischemia. We did not use triphenyltetrazolium chloride, because it was not available in our department at that moment. On every heart slice we checked the lumen of coronary artery.
Myocardial fragments harvested from autopsy were fixed at least 48 hours in 10% buffered formalin and processed using paraffin embedding technique. Tissue blocks were sliced with a manual microtome at 4μ thick sections and the slides were stained with Hematoxylin and Eosin (with an automated staining station) and Masson trichrome (manual staining technique).
Our study included 96 patients with STEMI and no-reflow phenomenon after PCI procedure, of whom 14 died – 4 female subjects and 10 male subjects. The mortality rates according to the sex and age of the patients can be seen in Table 1.
Mortality rates by sex and age in our study
| Women | Years | No | Deaths |
| Under 50 yo | 3 | 0 | |
| 50–70 yo | 11 | 1 | |
| Over 70 yo | 18 | 3 | |
| Men | Under 50 yo | 15 | 0 |
| 50–70 yo | 32 | 4 | |
| Over 70 yo | 17 | 6 |
yo = years old; No = number
In this prospective cohort analysis, we examined the association between age and mortality, stratified by sex. Among women, the risk of death for those aged over 70 years was more than twice that of women aged 70 years or younger, with a risk ratio (RR) of 2.33 (95% confidence interval [CI]: 0.27–20.09). However, this association did not reach statistical significance, as the confidence interval included the null value. In contrast, among men, those aged over 70 demonstrated a significantly increased risk of death compared to their younger counterparts, with an RR of 4.15 (95% CI: 1.33–12.93). This suggests a more pronounced and statistically significant age-related increase in mortality risk among men in the cohort. These findings highlight potential sex differences in age-related mortality risk, though the wide confidence intervals, particularly among women, underscore the need for cautious interpretation and may reflect limited sample size or event frequency.
The mortality rates recorded in our study based on STEMI characteristics are illustrated in Figure 2 revealing the location of culprit coronary arteries and stents used for myocardial revascularization among patients with fatal outcomes.
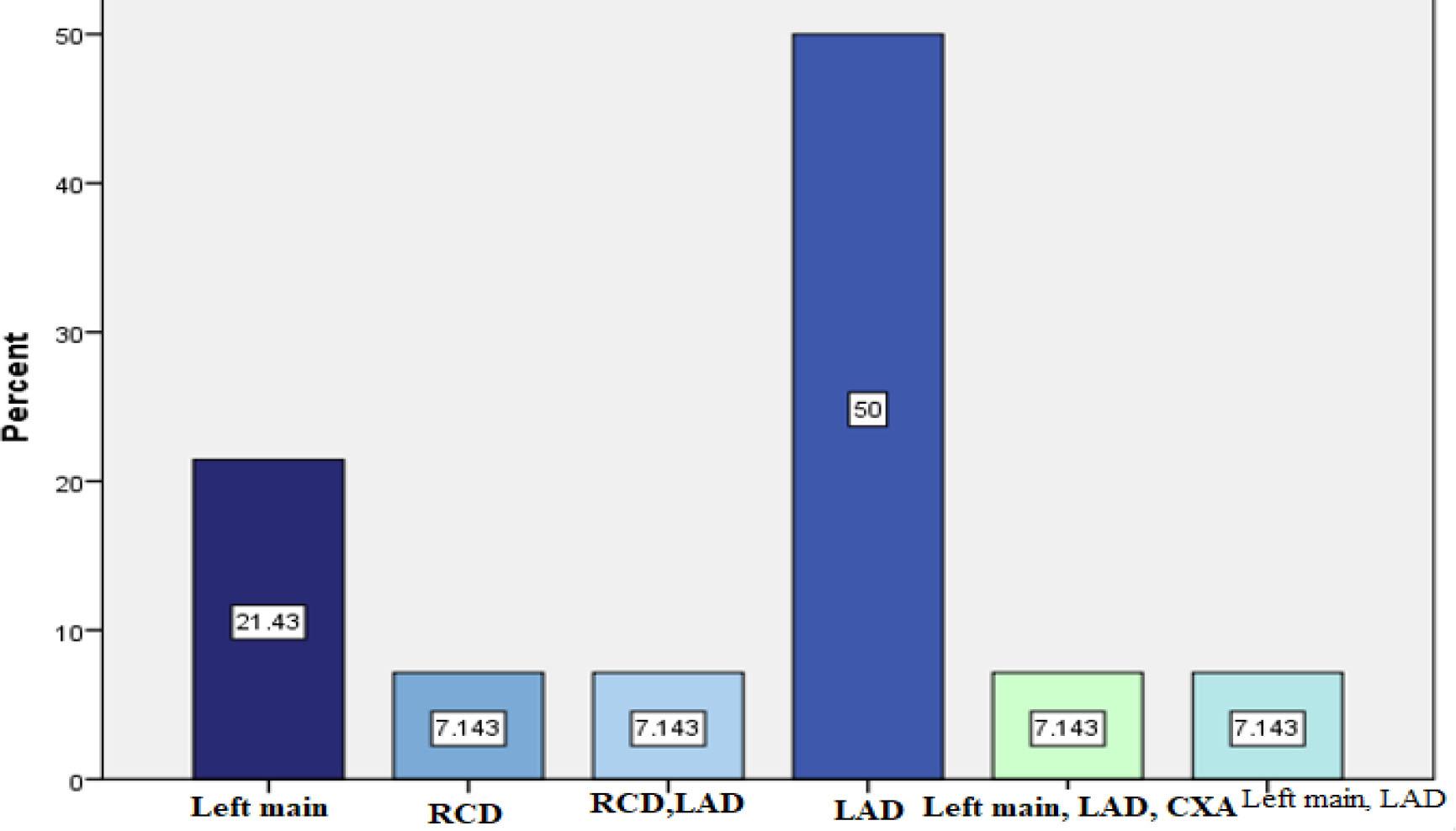
Stent implantation in culprit lesions during PCI performed in STEMI subjects.
In patients with anterior STEMI mortality rate was significantly increased compared with the inferior infarction group (42.9% vs. 14.3%), the risk of death being threefold higher for anterior localization.
STEMI subjects with culprit lesion involving left anterior descending artery (LAD) expressed the highest rate of fatal outcome compared with lesions of the other two epicardial coronary arteries, circumflex coronary artery (CXA) and the right coronary artery (RCA), as seen in Figure 2.
After PCI, mortality was significantly influenced by the magnitude of coronary artery lesions. A study illustrated increased mortality among patients with arterial stenosis > 75% to those with arterial stenosis <75% (21.3% vs. 7.1%). The risk of death after PCI is 3 times higher in patients with arterial stenosis > 75% than in those with stenosis < 75%.
Another mortality predictor is represented by atheroma plaque rupture complicated with thrombosis compared with plaque rupture without thrombosis, which expressed a lower mortality rate (78.57% vs. 21.43%). The death risk after PCI is 3.2 times higher in patients with atheroma plaque rupture and thrombus synthesis than in subjects with plaque rupture alone.
According to the no-reflow phenomenon type, the in-hospital mortality is illustrated in Figure 3.
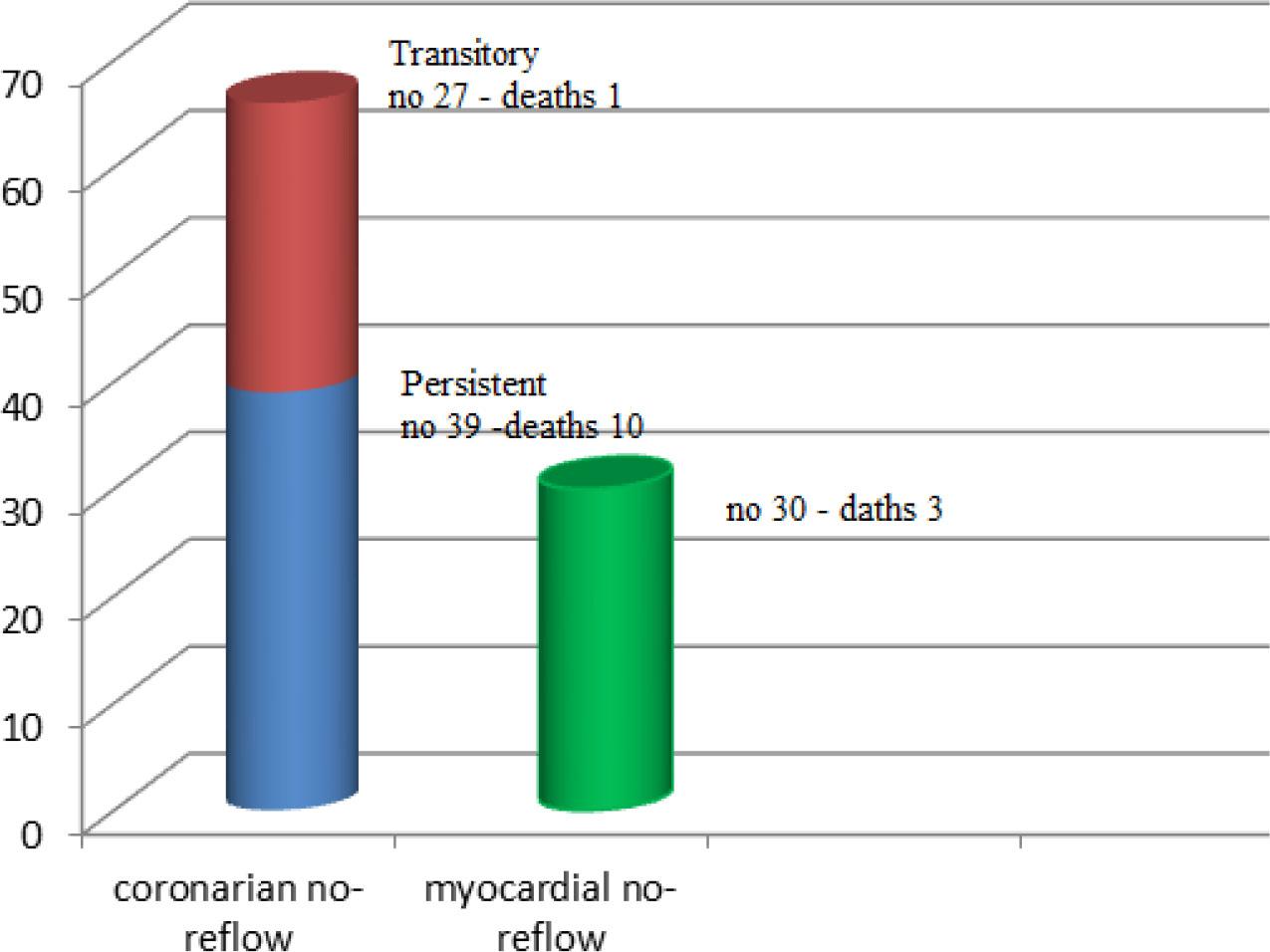
In-hospital mortality predicted by the no-reflow phenomenon type.
The fatality rate was significantly increased in subjects with coronary no-reflow phenomenon than in the myocardial no-reflow group (p = 0.039), and was significantly higher in persistent no-reflow patients versus transitory no-reflow subjects (25.64% vs. 3.70%, p = 0.010). The mortality rate was 1.8 times higher in patients with coronary no-reflow compared to those with myocardial no-reflow (OR = 1.80, 95% CI: 0.46–6.99) and 9 times higher in the persistent no-reflow group compared with those in transitory no-reflow group (OR = 8.96, 95% CI: 1.07–74.89).
Post-PCI fatal outcome was significantly higher in patients with associated complications than in those without complications (33.33% vs. 1.75%, p <0.001). The main complications that were identified in the study are illustrated in Table 2. The risk of death in patients with STEMI and associated complications is 28 times higher than in those without complications (OR = 28.00, 95% CI: 3.47–225.58). Most patients had a single complication (9 cases, of whom 5 – cardiogenic shock, 3 – rhythm disturbance, 1 – myocardial rupture). Association of complications was noted in two cases, one case with rhythm disorders and cardiogenic shock, and the other with rhythm disorders and pulmonary oedema. The other subjects had 3 or 4 complications (rhythm disorders + left ventricular aneurysm + cardiogenic shock, respectively, rhythm disorders + pulmonary oedema + myocardial rupture + heart failure).
Complications after PCI found in STEMI patients with no-reflow phenomenon included in our study
| Complications | Number of patients | Deaths |
| Rhythm disorders | ||
| No | 75 | 11 |
| Yes | 21 | 3 |
| Acute pulmonary oedema | ||
| No | 91 | 10 |
| Yes | 5 | 4 |
| Left ventricular aneurysm | ||
| No | 92 | 13 |
| Yes | 4 | 1 |
| Cardiogenic shock | ||
| No | 80 | 9 |
| Yes | 16 | 5 |
| Myocardial rupture | ||
| No | 95 | 13 |
| Yes | 1 | 1 |
Of the 96 patients with no-reflow phenomenon, 39 had complications, and 14 died. The group of subjects without complications had a lower mortality rate (only one subject with a fatal outcome).
Mortality predictors in the no-reflow phenomenon found in our study were represented by rhythm disturbances, pulmonary edema, ventricular remodeling, cardiogenic shock, and myocardial rupture. Lethality was significantly higher in patients with rhythm disorders compared with subjects without arrythmia (33.33% vs. 9.33%, p = 0.006), in pulmonary edema group versus no pulmonary congestion group (60.00% vs. 13.19 %, p <0.001) and in cardiogenic shock study lot versus hemodynamically stable study lot (50.00% vs. 7.50%, p <0.001). Subjects with ventricular aneurysm had a higher mortality rate than those without this complication (25.00% vs. 14.13%, p = 0.055).
Patients with myocardial infarction who died after primary PCI presented clear signs of full–thickness myocardial infarction during autopsy, and we correlated the age of the lesion with the clinical history from medical charts.
All autopsied patients presented with transmural left ventricular myocardial infarction. Table 3 reflects which coronary were totally occluded in our subjects. In patients with early myocardial infarction (1–3 days old), we could appreciate a central yellow tan lesion (corresponding with muscle fiber coagulative necrosis) and peripheral mottling as shown in Table 4 (Figure 4.1). The border became more hyperemic in older lesions, and its microscopic hallmark was represented by granulation tissue with intense fibro-vascular matrix.
Morphologic aspects of myocardial infarction in patients with STEMI and no-reflow phenomenon after primary PCI
| Coronary branch | Territory affected | Approximate age of lesion | Number of cases |
|---|---|---|---|
| Left anterior descending coronary artery | Anterior and interventricular septum | 24–120 hours | 2 |
| Left circumflex coronary artery | Lateral part of the left ventricle | 48–72 hours | 1 |
| Right coronary artery | Posterior part of the left ventricle | 24–96 hours | 2 |
Anatomic-clinical correlations were made, and no differences were found between the topography of the lesion at autopsy and angiography mapping. Coronary arteries had severe atherosclerosis, and no iatrogenic dissected coronary branches were observed during autopsies.
After examining histological slides from tissue harvested during autopsies, we confirmed death of myocardial fibers (Fig. 4.3) associated with heavy neutrophilic infiltration in the interstitial space and severe edema. We found in one case rupture of the myocardium after a full-thickness infarction, demonstrated also on HE slides as seen in Figures 4.4 and 4.5. In the mentioned case, we could appreciate the fissure in the myocardium fibers, extravasation of erythrocytes, and a mixed inflammatory infiltrate. In another case, we depicted intramuscular thrombosis after myocardial infarction (Fig. 4.6). In pericardial tissue, we found ruptured and thrombosed atherosclerotic plaques with a fibrous cap and calcification.
Table 4 presents a representative spectrum of gross and histopathological alterations observed in patients with ST-elevation myocardial infarction (STEMI) who exhibit the no-reflow phenomenon. Gross pathological findings (Figs. 4.1 and 4.2) demonstrate the temporal progression of infarction, from early transmural ischemia in a posterior myocardial infarction (2–3 days old) to extensive full-thickness necrosis in a posterolateral infarct (4–5 days old). Histological images further delineate the underlying myocardial pathology: transmural coagulative necrosis with dense neutrophilic infiltration (Fig. 4.3), disorganized myocardial architecture with interstitial hemorrhage and evidence of rupture (Fig. 4.4), and high-power views showing fissures between necrotic fibers (Fig. 4.5) as well as thrombotic occlusion accompanied by inflammatory infiltrates (Fig. 4.6). These findings reflect the multifactorial pathophysiology of no-reflow, characterized by ischemia-reperfusion injury, microvascular obstruction, and intramyocardial hemorrhage. The integration of macroscopic and microscopic evidence underscores the structural basis for impaired myocardial perfusion despite successful epicardial reperfusion and highlights the prognostic implications of no-reflow in the context of acute STEMI.
Gross and histological features in STEMI patients exhibiting the no-reflow phenomenon
| Macroscopy | |
| Fig. 4.1. Posterior myocardial infarction (2–3 days old): Gross appearance with early transmural ischemic changes. | Fig. 4.2. Posterolateral myocardial infarction (4–5 days old): Full-thickness infarction observed during autopsy. |
| Microscopy | |
| Fig. 4.3. H&E stain, 10×: Transmural necrosis with prominent neutrophilic infiltration in the interstitial space. | Fig. 4.4. H&E stain, 4×: Myocardial rupture with disorganized tissue architecture and interstitial hemorrhage. |
| Fig. 4.5. H&E stain, 20×: Detailed visualization of a fissure between necrotic myocardial fibers. | Fig. 4.6. H&E stain, 20×: Thrombosed myocardial region accompanied by inflammatory cell infiltration and necrosis. |
Previous studies revealed that there are no significant correlations between mortality and gender among subjects with acute myocardial infarction and no-reflow phenomenon [36,37], an aspect that is also revealed in our study, where female mortality was insignificantly smaller than the male fatal outcome.
In terms of age, this study shows that the average age of death is significantly higher for women than male subjects, which is in contradiction with some studies in the literature that report a higher average age of death among men [38].
Our study reflects that anterior STEMI involves mainly lesions of LAD, which is in accordance with the other studies [39].
Karwowski J. [40] promotes that the LAD culprit lesion responsible for STEMI is associated with significant cardiovascular mortality. This aspect is also shown in our study, which reveals that LAD was the main culprit lesion causing death among STEMI patients.
Mortality among patients with the coronary no-reflow phenomenon is higher compared with the myocardial no-reflow phenomenon group, a fact also pointed out in the literature [41]. The persistent coronary no-reflow phenomenon represents a mortality predictor in STEMI subjects with a major negative impact in comparison with transitory no-reflow. The same aspect was revealed by Kim MC et al. [42]. Their article suggested that persistent no-reflow phenomenon after primary PCI involves an increased risk of in-hospital mortality and complications development than the transitory no-reflow phenomenon.
Also, the literature states that prognosis is different in subjects who develop no-reflow phenomenon versus those with optimal myocardial perfusion. The presence of the mentioned phenomenon predicts long-term complications and increased mortality [43], so strategies for prevention and optimal management should be considered.
Regarding atheromatous plaque or thrombosis that are incriminated in acute myocardial infarction, Badimon L. and Vilahur G. revealed that atheroma plaque rupture complicated with thrombosis is a common finding in autopsies compared with plaque erosion [44], which is consistent with our study.
It is already known that STEMI patients with no-reflow phenomenon may be associated with frequent cardiovascular complications compared to those without the phenomenon [6]. Kaul S. [45] believes that the no-reflow phenomenon leads to a decrease in the ventricular systolic function, with the increase of the infarct-related area and subsequent ventricular remodeling, followed by malignant rhythm disorders, which also results from this study. Cardiogenic shock occurrence after primary PCI in subjects with no-reflow phenomenon is a negative prognostic factor that increases mortality according to the literature [3], an aspect also revealed by our article. Acute pulmonary predicts negative outcome and influences the risk of death among STEMI patients, results illustrated in existing studies [46] and our paper.
Ventricular aneurysm is a complication of acute myocardial infarction [47] and also expresses the consequence of the no-reflow phenomenon [48,49]. Pathological ventricular remodeling predicts poor prognosis in STEMI subjects. According to Shamshad F. and co-workers [50,51,52], myocardial wall rupture is less common in patients with myocardial infarction compared with other complications. The incidence of myocardial wall rupture is less than 1% and without proper surgical emergency intervention, the outcome is fatal, which is similar to our study data.
While electrocardiography (ECG) remains a widely accessible and commonly used tool for assessing myocardial perfusion, its utility in accurately characterizing the no-reflow phenomenon is limited. In the absence of advanced imaging modalities such as cardiac MRI or myocardial contrast echocardiography, we relied on ECG-based criteria in conjunction with angiographic findings. We acknowledge that this approach, while practical in many clinical settings, may reduce diagnostic specificity and should be interpreted with caution.
A key limitation of our study lies in the diagnostic differentiation between coronary and myocardial no-reflow. Although ECG is less specific and can be influenced by various confounders, its use in clinical settings remains common, particularly when other modalities are unavailable. We recognize this constraint may impact the precision of classification and have addressed this limitation accordingly in our interpretation of the results.
Several limitations should be considered when interpreting the findings of this study.
First, the relatively small sample size of patients who developed the no-reflow phenomenon after primary PCI (n = 96), and particularly the limited number of deaths (n = 14), may reduce the statistical power to detect certain associations and contribute to wide confidence intervals in risk estimates. This may particularly affect the robustness of subgroup analyses, such as those comparing coronary and myocardial no-reflow, or anterior versus inferior STEMI.
Second, the study was conducted at a single center, which may limit the generalizability of the findings to broader or more diverse populations. Local clinical practices, patient demographics, and operator expertise may have influenced both procedural outcomes and complication rates.
Third, although the study prospectively enrolled patients, potential residual confounding cannot be excluded. Factors such as infarct size, time to reperfusion, medication adherence, and pre-existing comorbidities may have influenced mortality risk but were not fully controlled for in the analysis.
Fourth, the definition and classification of the no-reflow phenomenon into “coronary” and “myocardial” subtypes, while clinically relevant, may be subject to diagnostic variability, especially in the absence of uniform criteria or advanced imaging to quantify microvascular obstruction.
Another limitation of this study is the small number of cases that underwent pathological examination, including triphenyltetrazolium chloride (TTC) staining. This limited pathological sample size constrains the ability to draw definitive correlations between histopathological findings and clinical or angiographic features, and therefore warrants cautious interpretation of these results.
A key limitation of this study is the reliance on ECG for identifying myocardial no-reflow, given its limited specificity and sensitivity compared to advanced perfusion imaging. Additionally, the relatively small number of patients with confirmed no-reflow and in-hospital mortality events restricts the statistical power and generalizability of our findings. These factors should be considered when interpreting the results and underscore the need for larger, multicenter studies incorporating comprehensive imaging strategies.
A major limitation of our study lies in the differentiation between coronary and myocardial no-reflow phenomena. In the absence of advanced imaging modalities such as myocardial contrast echocardiography or cardiac magnetic resonance imaging, we relied on a combination of angiographic findings (TIMI flow and myocardial blush grade) and electrocardiographic changes (persistent ST-segment elevation) to classify no-reflow types. However, ECG is a nonspecific tool for assessing myocardial perfusion, subject to multiple confounding factors and limited diagnostic accuracy. This approach may introduce misclassification bias and reduce the precision of our no-reflow subtype categorization. We acknowledge this methodological constraint and emphasize that our findings should be interpreted within the context of these diagnostic limitations. An important limitation is the reliance on electrocardiographic (ECG) criteria for identifying myocardial no-reflow. While ECG remains a widely accessible and practical tool in clinical settings, it has limited specificity and sensitivity for directly characterizing myocardial perfusion compared to advanced imaging modalities. Therefore, the interpretation of myocardial no-reflow in our study may be subject to diagnostic uncertainty. Additionally, the relatively small sample size of patients with the no-reflow phenomenon further limits the statistical power and generalizability of our findings. These constraints underscore the exploratory nature of our analysis and support the need for future multicenter studies with more robust diagnostic tools. Finally, follow-up was limited to the in-hospital period, preventing assessment of long-term mortality predictors and outcomes. Further research with larger, multicenter cohorts and extended follow-up is necessary to confirm these findings and refine risk stratification in this high-risk patient population.
The coronary no-reflow phenomenon has the highest risk of mortality, accounting for more than half of the cases of infarction, compared with the myocardial no-reflow phenomenon.
In STEMI subjects with no-reflow phenomenon, LAD was the common culprit lesion responsible for a negative outcome.
Associated cardiovascular complications caused most deaths in STEMI patients with no-reflow phenomenon.