Despite recent innovative diagnostic and therapeutic techniques, pancreatic neoplasia remains one of the most lethal malignancies due to its late clinical onset [1]. In the last decades, endoscopic ultrasound (EUS) has reshaped the management of pancreatic masses, due to its capacity to diagnose and classify malignancies with excellent sensitivity and specificity [2].
EUS guided-fine needle aspiration (EUS-FNA) is currently considered the gold-standard method for pancreatic tissue acquisition. However, the emergence of targeted therapies as part of personalized medicine in pancreatic cancer indicates the need to provide larger core tissue biopsies, amenable to histopathologic, molecular and genetic studies [3]. Recently, EUS-fine needle biopsy needles (EUS-FNB) have gained much attention. EUS-FNB seems to improve the diagnostic yield of prior negative EUS-FNA by obtaining larger samples with a preserved architecture, amenable to excluding difficult-to-diagnose pathologies like lymphoma, autoimmune pancreatitis, neuroendocrine tumors and many others [4]. This is due to its unique biopsy technique, which is not related to the needles’ diameter, but to the storing mechanism, requiring fewer needle passes for a better result. Even though FNB is widely used in clinical practice, more studies are needed to ascertain the accuracy of these innovative needle types [4].
Our study focuses on a cohort of patients with pancreatic lesions suggestive of neoplasia. First, we intended to assess the accuracy of EUS-guided tissue acquisition, either using FNA, FNB or both. Secondly, we set out to analyze the parameters that might influence the histological results and the accuracy of the needle used.
This study is a retrospective, 5-year spanning analysis of all tissue acquisitions using EUS, between June 2017 and October 2022, at the Gastroenterology Department of the Clinical Emergency Hospital of Bucharest, a tertiary, large referral center. All patients were older than 18 years and signed an informed consent before each procedure, in accordance with the Helsinki Declaration.
During the period mentioned above, 484 patients underwent 515 EUS-guided tissue acquisition procedures for suspicion of pancreatic neoplasia. Ultimately, 401 patients out of 484 were eligible for our study, having a biopsy result of pancreatic cancer established by either EUS-FNA, EUS-FNB or surgical intervention. These were the patients included in the statistical analysis. We excluded from our study those patients with benign results despite initial imagistic evaluations suggestive of neoplasia.
A retrospective analysis was conducted on patient demographics and medical information. Various factors were examined, including age, sex, pre-EUS imaging techniques (CT and/or MRI), diagnostic yield of EUS-FNA and EUS-FNB, pancreatic tumor characteristics (location and size), and details of EUS procedures (needle types, number of passes, procedures required for malignancy diagnosis, and presence of biliary/pancreatic stents).
All procedures were performed by a senior endoscopist. We used the 22G EUS-FNA ExpectTM and the 22G EUS-FNB AcquireTM (Boston Scientific Corporation, Marlborough, MA, USA). For lesions in the pancreatic head or uncinate process, both needles were inserted through the duodenum. In contrast, stomach punctures were used for tumors in the pancreatic body and tail. To avoid vascular interference with the needle trajectory, Doppler-mode was utilized. The sampling procedure remained consistent for both FNA and FNB needles: after puncturing the lesion, the stylet was slowly removed, and suction was applied using the 20 cubic centimeter syringe, at the same time moving the needle to-and-from in a fanning pattern. The needle was withdrawn after releasing suction. Following each extraction, the collected samples were initially preserved in a formalin-based liquid container and labeled. Subsequently, the samples were processed and embedded in paraffin blocks. As our center doesn’t carry out rapid on-site evaluations (ROSE), the samples were sent to the Pathology Department. There, the tissue underwent staining with Hematoxylin-Eosin and various immunohistochemistry markers. Subsequently, it was examined under a microscope to determine its histological particularities.
All of the data was statistically examined and incorporated in a database made specifically for this study. We utilized the IBM SPSS v.20 software package for data analysis, and a p-value of less than 0.05 was accepted as statistically significant. For continuous variables, descriptive statistical findings were presented as medians and ranges or as means ± standard deviations and ranges. Furthermore, frequencies and absolute numbers with percentages were used to express categorical variables. Based on our databases, we conducted a number of tests, including the ANOVA unifactorial test and the Chi-Square test to evaluate a statistical hypothesis.
In accordance with today's norms of care, all examined data was obtained as part of normal diagnosis and treatment process. All subjects of the study, or their authorized representatives, gave written informed consent prior to beginning of any procedures.
Between June 2016 and October 2021, 484 patients were addressed to our hospital for pancreatic tissue sampling by EUS guidance, following sectional identification of pancreatic neoplasia. Out of the initial 484 patients and 515 EUS procedures for purported malignancy, we selected 401 patients with 426 EUS procedures to be included in the study, due to their malignant state confirmed by histopathological examination at either EUS or surgery. The demographics and tumoral aspects of these patients are presented in Table 1. The mean age of the patients' lot was 63.99±10.91 years. The distribution according to gender showed slightly more males (211) than females (190). The mean diameter of the pancreatic lesion was 36.59±16.23 mm, and 75% of the tumors were found in the head or uncinate process. At the moment of the EUS procedure, one-third of the patients had a biliary or pancreatic stent in situ. In 94.5% of all patients included, EUS-guided tissue sampling was performed as a single procedure, while the rest of the patients underwent 2 (4.8%) or 3 EUS procedures (0.7%).
Demographics of the patients and pancreatic tumor details in the current lot
| Parameters | Total number of patients (n=401) |
|---|---|
| Mean age ±SD, years | 63.99±10.91 |
| Gender, no. (%) | |
| Male | 211 (52.6%) |
| Female | 190 (47.4%) |
| Lesion diameter, mean±SD, mm | 36.59±16.23 |
| Tumor localization, no. (%) | |
| Head/uncinate | 301 (75.1%) |
| Body | 75 (18.7%) |
| Tail | 25 (6.2%) |
| Presence of biliary/pancreatic stent, no. (%) | |
| Yes | 118 (29.4%) |
| No | 283 (70.6%) |
| Number of EUS procedures per pacient, no. (%) | |
| One procedure | 379 (94.5%) |
| Two procedures | 19 (4.8%) |
| Three procedures | 3 (0.7%) |
| Final malignant diagnosis, no. (%) | |
| EUS-FNA/FNB | 365 (91.02%) |
| Surgery | 36 (8.97%) |
Abbreviations: SD=standard deviation; EUS-FNA/FNB=endoscopic ultrasound-fine-needle aspiration/biopsy
Overall, the final diagnosis of pancreatic neoplasia was obtained through EUS-guided sampling in 91.02% of the patients. Most of them were positive after the first procedure (95.34%). The others were confirmed after repeated procedures: second EUS (16 patients) or third EUS (1 patient). There were 36 patients (8.97%) who had false-negative results after EUS-FNA/FNB. However, these patients were referred to surgery and ultimately confirmed with pancreatic malignancy (Table 2).
Positive and false-negative results of the 401 patients included in the study
| Patients with pancreatic neoplasia detected through EUS-FNA/FNB | 365 (91.02%) |
| Positive results after first EUS, n (%) | 348(95.34%) |
| Positive results after second EUS, n (%) | 16 (4.38%) |
| Positive results after third EUS, n (%) | 1 (0.27%) |
| Patients with pancreatic neoplasia false-negative at EUS examination, confirmed by surgery | 36 (8.97%) |
| Negative results after first EUS, n (%) | 31 (86.11%) |
| Negative results after second EUS, n (%) | 3 (8.33%) |
| Negative results after third EUS, n (%) | 2 (5.55%) |
Abbreviations: EUS-FNA/FNB=endoscopic ultrasound-fine-needle aspiration/biopsy
A total of 426 procedures were recorded for the 401 patients included in the study, out of which 334 were EUS-FNA and 92 EUS-FNB (Table 3). Both FNA and FNB were successful in the lot of patients (Figure 1). However, EUS-FNB exceeded EUS-FNA regarding the diagnostic yield (91.3% compared to 84.1%, p-value<0.05). In addition, the number of passes for the FNA procedures was on average 1.99 per case, compared to a significantly lower mean of 1.63 passes for each FNB procedure (p-value<0.05).
Regarding the general cohort, most subjects’ tumoral location was either in the head or the uncinate process of the pancreas. However, when analyzing the two FNA and FNB subcohorts, we observed that a higher percentage of the FNB procedures were carried out for tumors found in the body and tail (n=28, 30.4%) as compared to the FNA procedures (n=76, 22.8%). However, there was no statistical difference between the two groups (p-value=0.312). The presence of biliary or pancreatic stent was significantly more prevalent among FNB procedures compared to FNA procedures (39.1% vs. 26.9%, p-value<0.05). There were no major immediate or late complications recorded after the EUS sampling outside of two minor self-limiting episodes of bleeding (1 FNB procedure and 1 FNA procedure) and 3 mild acute pancreatitis or symptomatic hyperlipasemia (1 for the FNA and 2 for FNB needles).
Technical aspects and outcomes of FNA and FNB
| Total number of procedures (n=426) | p | ||
|---|---|---|---|
| FNA | FNB | ||
| Technical EUS success, no. (%) | 334 (100%) | 92 (100%) | |
| Diagnostic EUS yield, no. (%) | |||
| Positive | 281 (84.1%) | 84 (91.3%) | 0.048 |
| False-negative | 53 (15.9%) | 8 (8.7%) | |
| Number of passes, mean±SD | 1.99±0.52 | 1.63±0.60 | <0.001 |
| Lesion diameter, mean±SD, mm | 36.11±15.68 | 37.74±17.08 | 0.388 |
| Tumor localization, no. (%) | |||
| Head/uncinate | 258(77.2%) | 64(69.6%) | |
| Body | 58 (17.4%) | 21 (22.8%) | 0.312 |
| Tail | 18 (5.4%) | 7 (7.6%) | |
| Presence of biliary/pancreatic stent, no. (%) | |||
| Yes | 90 (26.9%) | 36 (39.1%) | 0.017 |
| No | 244 (73.1%) | 56 (60.9%) | |
| Major complications, no. (%) | 0 (0) | 0 (0) | |
Abbreviations: SD=standard deviation; EUS=endoscopic ultrasound; FNA=fine-needle aspiration; FNB=fine-needle biopsy
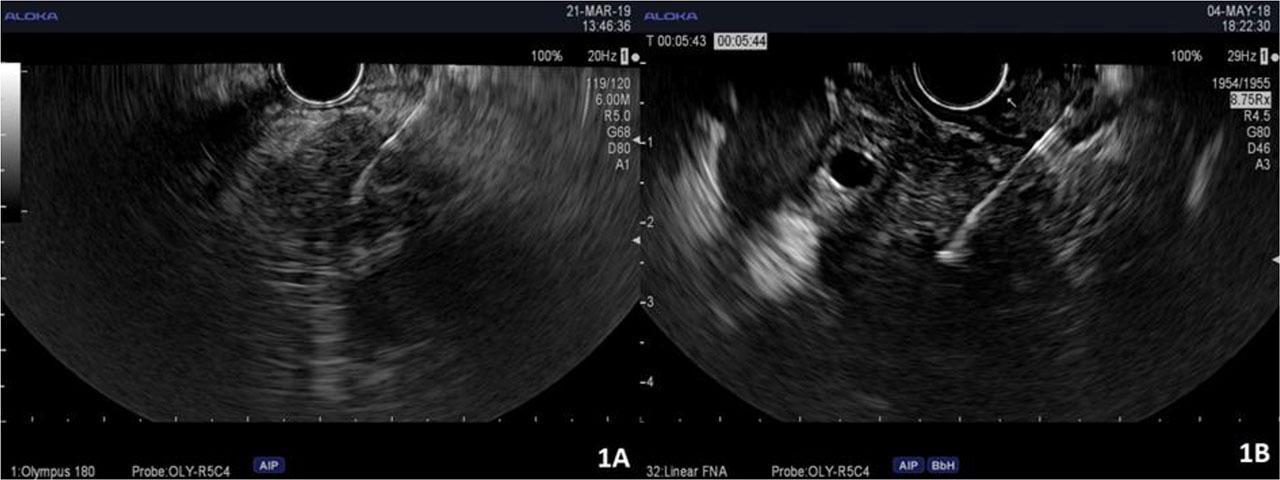
FNA (1A) and FNB (1B) EUS-guided biopsies from pancreatic tumors.
Histopathological results obtained by either EUS-FNA, FNB or following surgical intervention are shown in Table 4. The most frequently encountered pancreatic malignancies were the primary ones: ductal adenocarcinomas (n=332), followed by neuroendocrine tumors (pNETs) (n=26), cystadenocarcinomas (n=18), intraductal papillary mucinous neoplasms (n=3), one solid pseudopapillary tumor and one acinar-cell tumor (Figure 2). Out of the 36 patients rendered as false-negative at EUS-guided sampling, 35 had ductal adenocarcinoma and one patient was diagnosed with pancreatic neuroendocrine tumor (Figure 3). Regarding tumors with an extrapancreatic origin, there were 20 patients with secondary pancreatic malignancies: 7 myeloproliferative disorders (e.g. non-Hodgkin’s lymphoma), 3 gastric gastrointestinal stromal tumors (GISTs), 3 breast carcinomas, 3 renal carcinomas, 2 colonic carcinomas, 1 pulmonary neuroendocrine tumor, 1 hepatocellular carcinoma.
Histopathological results of EUS-FNA, FNB and surgery
| Histopathological diagnosis | FNA positive | FNB positive | FNA/FNB false-negative (surgery positive) |
|---|---|---|---|
| Pancreatic adenocarcinoma (n=332) | 232 | 65 | 35 |
| Pancreatic cystadenocarcinoma (n=18) | 15 | 3 | 0 |
| Pancreatic neuroendocrine tumor (n=26) | 16 | 9 | 1 |
| Non-Hodgkin lymphoma/leukemia (n=7) | 5 | 2 | 0 |
| Neoplastic gastric GIST (n=3) | 1 | 2 | 0 |
| Neoplastic IPMN (n=3) | 2 | 1 | 0 |
| Breast carcinoma metastasis (n=3) | 2 | 1 | 0 |
| Clear-cell renal carcinoma metastasis (n=3) | 2 | 1 | 0 |
| Colonic carcinoma metastasis (n=2) | 2 | 0 | 0 |
| Pulmonary neuroendocrine metastasis (n=1) | 1 | 0 | 0 |
| Hepatocellular carcinoma metastasis (n=1) | 1 | 0 | 0 |
| Pancreatic acinary carcinoma (n=1) | 1 | 0 | 0 |
| Solid pseudopapillary neoplasia (n=1) | 1 | 0 | 0 |
Abbreviations: FNA= fine-needle aspiration; FNB= fine-needle biopsy; GIST=gastrointestinal stromal tumor; IPMN=intraductal papillary mucinous neoplasms
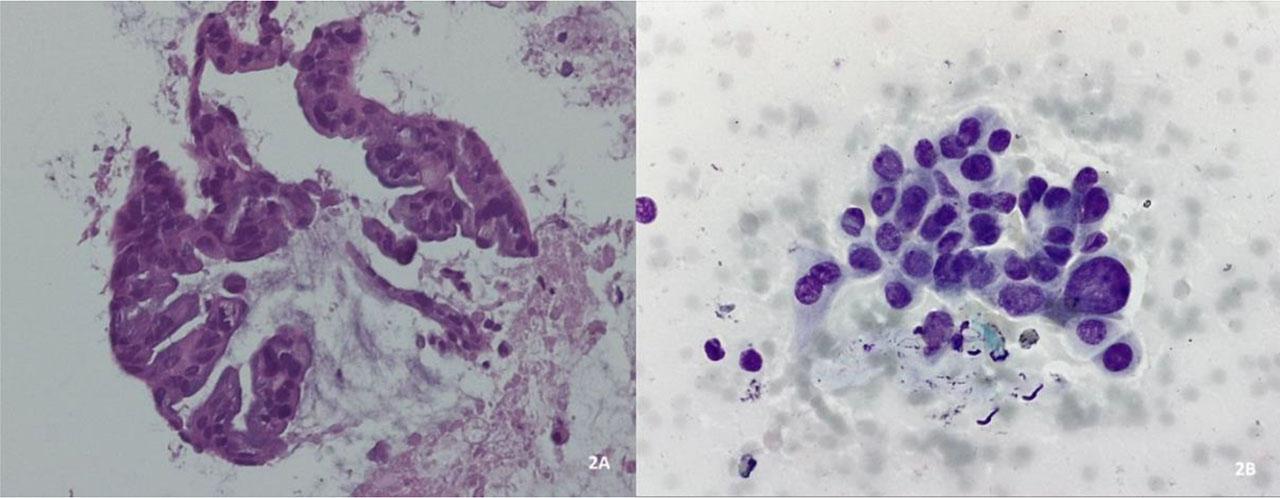
Histological evaluation of with hematoxylin and eosin staining of pancreatic ductal adenocarcinoma.
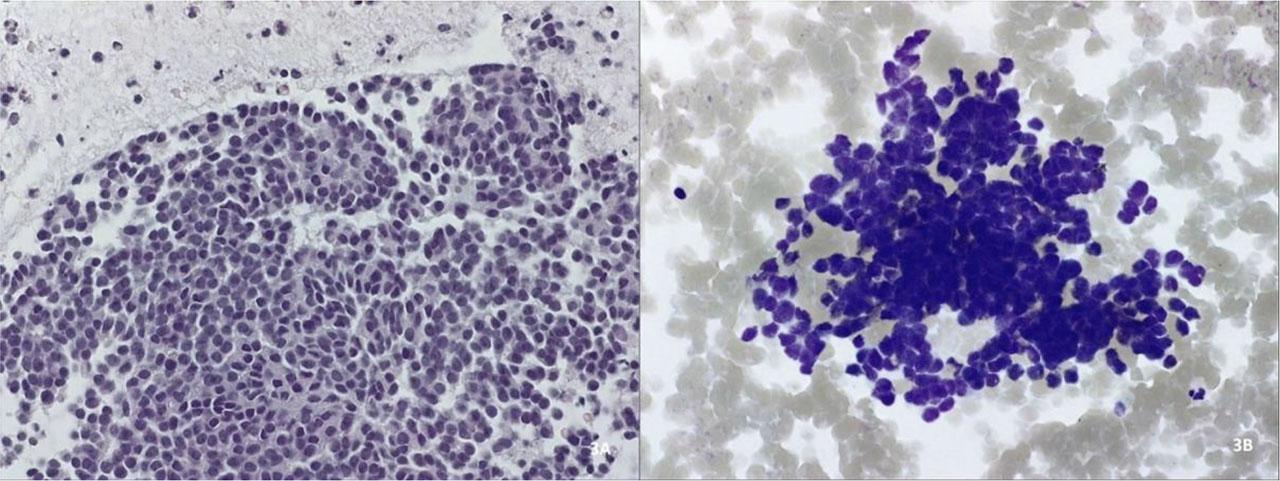
Cytological examination with hematoxylin-eosin (3A) and Giemsa (3B) staining of a pancreatic neuroendocrine tumor.
Eventually, due to staging or performance status, 93 out of the total 401 subjects were sent for surgical management, mostly for palliative or resectional reasons, but also for diagnostic laparoscopy.
Pancreatic disorders have represented a mystery since ancient times, when Herophilos first described in 2300 B.C. the organ later named by Rufus of Ephesus, in the first century A.D, by the term “pancreas”, from the Greek “all flesh” [5]. Pancreatic history has evolved through the centuries from the 70 grams “cushion of the stomach” and “the finger of the liver” as described by Galen and the Talmud, to the nowadays glamourous, still mysterious “pancreatology” [5,6]. After the development of endoscopic techniques at the dawn of the 20th century and a war-driven development of ultrasonographic techniques such as the SONAR (sound navigation and ranging), EUS naturally surfaced in 1982, when DiMagno and collaborators carried out the first human endosonography using an optical echoendoscope prototype, followed by the first EUS-guided tissue sampling, performed by Vilmann in 1992 [7,8]. During recent decades, this peculiar part of science, pancreatology, has apparently gained momentum as newly introduced techniques such as EUS have surged to the imaginably utmost development, enabling unimaginable state-of-the-art bio-molecular, immunochemical and genetic techniques, and setting year-by-year new directions toward what has already delineated as personalized medicine [9]. Currently, EUS-tissue acquisition is widely accepted as the gold-standard for many pathologies of upper eso-gastrointestinal and mediastino-pulmonary lesions, but most of all represents an invaluable tool for biliary-pancreatic disorders, especially for pancreatic masses suspected of being malignant [10]. Through the years, EUS-FNA has been the sole method of obtaining samples amenable to diagnostic testing, with impressive diagnostic accuracy in the range of 87–92% for extradigestive masses, but recent innovations have brought about the EUS-FNB needles, with multiple types and features [4,11]. The need to precisely diagnose gastrointestinal wall lesions, lymphoma, autoimmune pancreatitis, neuroendocrine tumors and others, has led to the emergence of a variety of FNB needles, such as the beveled side-slot or the forward facing biopsy needle (Quick-Core® and ProCore®, Cook Medical, Bloomington, IN, USA) and the crown-cut, fork-tipped needle, with two opposite cutting edges introduced in 2014 (SharkCoreTM, Medtronic, Minneapolis, MN, USA) [10]. Franseen-type needles were further introduced, the first with three cutting edges, symmetrically distributed at the tip (AcquireTM, Boston Scientific, Marlborough, MA, USA), which is the one used in our study, and another one with a slight adjustment to the angle of the cutting edges as compared to the first one (TopGain®, Mediglobe, Achemühle, Germany) [4]. Numerous studies have been performed for the assessment of the FNB needles with no overall difference noted in sample adequacy, histologic core, procurement rate or adverse event rate, but with fewer needle passes necessary for reaching a diagnostic sample in the case of the reversed bevel FNB needle, as compared to the FNA needle [12,13]. Nevertheless, the medical context of the present day, which sets a great deal of burden upon the cost-efficiency of medical procedures, still raises questions about the best needle option for large tertiary centers worldwide, in poorer or richer countries. Recent studies have compared EUS-guided punctioning with the FNB needle to the FNA needle, either alone or added by the ROSE technique, but at the same time ascertain that most tertiary centers lack the ability to do the on-site evaluation [14,15]. While costs and accuracy of the FNB and FNA+ROSE are relatively similar [16], FNA without ROSE is still performed in many European centers, ROSE being more popular on the American continent or limited to cases with a previous negative diagnosis [17,18]. Other studies also compared the diagnostic yield, procedure time and costs of EUS-FNB to EUS-FNA+ROSE and describe the higher diagnostic efficiency of the EUS-FNB, as well as a two-thirds procedure time as compared to their counterparts. Procedural costs are significantly higher for FNA+ROSE, due to the ROSE costs ($144 higher than FNB in one study), but the mean pathology costs were higher for the FNB, due to their larger tissue specimens, more likely to undergo additional tissue testing ($107 higher in the same study) [19]. Another US study revealed that the diagnostic yield of FNB was higher compared to the FNA without, showing the cost-effectiveness and superiority of the FNB [20]. Moreover, a meta-analysis of FNA+ROSE reviewed the impact of ROSE on the diagnostic yield of pancreatic FNA and it showed no improvement outside of cases where the adequacy rate without ROSE is low [21]. Alternatively, studies have identified MOSE (macroscopic on-site evaluation) using a FNA 19G needle or a FNB 22G Franseen tip needle as a feasible substitute for ROSE with high adequacy and accuracy of over 90% [22,23,24].
Our study sets the scene for one of the still intriguing questions of large tertiary centers dedicated to EUS-guided tissue acquisition where ROSE is not available. The solution includes the use of the cheaper FNA needle or the more expensive FNB needles, which come with modern different–shaped tips. Another approach is the surgical alternative for the cases with strong indications based on sectional imaging. Despite a better staging, it comes with numerous drawbacks such as a relatively high morbidity and mortality, higher risk of fistulous tract, and last but not least, a higher medical cost [25,26,27,28].
In our study, we retrospectively reviewed the data of a statistically significant cohort of 484 patients selected by sectional imaging, having a pancreatic nodule susceptible to differential diagnosis between a benign lesion (e.g., pseudotumoral chronic pancreatitis) and pancreatic cancer. They ultimately underwent 515 EUS-FNA or FNB procedures for determining the nodules’ histologic origin. We eventually included in the study 401 pancreatic cancer patients identified using either EUS-guided tissue acquisition procedures (n=365, 91%) or surgery (n=36, 9%). All in all, the patient lot underwent 426 EUS-FNA or FNB procedures and a further 93 were sent for surgical management, most of them for palliative or resectional reasons, but also for diagnostic laparoscopy. Cohorts’ demographic (age, gender) or topographical (lesions’ diameter, location) characteristics showed no discrepancies when compared to other studies [29,30], except the slightly higher percentage of FNB punctures carried for body and tail lesions (30.4% versus 22.8% for FNA). The presence of a biliary or pancreatic stent, noted in about 30% of the cohort subjects, did not influence the accuracy of FNA or FNB, but it was significantly more prevalent among FNB procedures than FNA (39.1% vs. 26.9%, p <0.05). This result is in accordance with the medical literature [31] and can be justified by the preference of FNB for a patient with an already advanced stage of the disease, considering the larger diagnostic yield, lesser false-negative results, and fewer number of passes for FNB compared to FNA, resulted in our study.
Combined diagnostic methods after EUS-FNA/FNB provided a positive result in 91.02% of the cases. After the first EUS, we had a 95.34% rate of positive results, revealing the high accuracy of EUS in diagnosing pancreatic cancer, even in the first procedure. Despite a much larger number of FNA procedures, both FNA and FNB subcohorts reached a high degree of success percentage – 84.1%, respectively 91.3% (p-value<0.05), despite the nearly doubled percentage of false negative results for the FNA needles (15.9% versus 8.7%, p<0.05). As anticipated, the mean number of passes used for the FNA needle to reach the diagnostic yield percentage was slightly higher than for the FNB needle (1.99±0.52 versus 1.63±0.60, p-value<0.001).
Histological analysis showed an interesting picture of the pancreatic adenocarcinomas (n=35) with false-negative results on EUS-FNA or FNB. They were mostly ductal adenocarcinoma, except for a pancreatic neuroendocrine tumor (pNET). The confusion could be explained by the ambiguous histological image due to a more frequent cystic or necrotic degeneration, carcinoma alternating with benign tissue in chronic pancreatitis patients that developed cancer, other technical or anatomical peculiarities, or even misinterpretation by the pathologist of well-differentiated pancreatic tissue samples [32,33,34,35]. Another particularity of the study is the relatively high number of non-ductal adenocarcinomas identified by histological studies (n=69, 17.2%). We found in our lot 18 cystadenocarcinoma, 26 pNETs, 7 myeloproliferative disorders (e.g. non-Hodgkin’s lymphoma), 3 gastrointestinal stromal tumors (GIST), 3 intraductal papillary mucinous neoplasms (IPMN), 3 breast carcinoma metastases, 3 clear-cell renal carcinoma metastases, 2 colonic cancer metastases, 1 pulmonary neuroendocrine metastasis, 1 hepatocarcinoma metastasis, 1 acinar-cell carcinoma and 1 solid pseudopapillary neoplasia. Out of the total 84 positive for malignancy nodules identified by EUS-FNB, a relatively high 10.7% were pNETs (n=9), which in the context of the single misdiagnosed surgical patient with pNET being offered the FNA, sets the accuracy of the FNB for pNET diagnosis at 100%.
The variables presented in the study reinforce the literature data available of FNB needles performing better than FNA’s when looking at technical efficiency, procedural safety and costs [3,4,36,37]. Cytological and histological examinations found that FNB was significantly higher than FNA regarding the diagnostic yield (91.3% vs. 84.1%; p-value<0.05). Moreover, FNB required fewer needle punctures than FNA to achieve diagnosis (1.63 vs. 1.99; p-value<0.05). In the context of several pancreatic pathologies presenting with similar features to pancreatic neoplasia (e.g. lymphoma, autoimmune pancreatitis, pNET, etc.), architecturally-preserved samples are of utmost need and the future will eventually belong to an improved FNB-type needle. At present, in the context of a brutal and rapid disease course and of many countries’ medical systems lacking necessities, FNA without ROSE seems for the moment a cheaper solution with a relatively high diagnostic yield and will much likely continue to be used in the years to come.
This study has some inherent limitations that should be addressed. Firstly, we are concerned about the large difference in sample size between the two groups (FNA vs. FNB), which could impair the statistical results. The medical literature affirms that FNA is the gold standard EUS technique for the diagnosis of pancreatic cancer [3], a fact reflected in our clinic where the FNA procedure is more frequently performed. Secondly, being a retrospective study with no randomization in choosing patients, we faced the issues of selection bias for the patient lot and non-replicable results. However, to enhance data quality and mitigate biases, further studies should be conducted in the future on similar FNA and FNB groups with randomized patient lots.
Both EUS-FNA and EUS-FNB are safe procedures with high accuracy for pancreatic malignancies. While EUS-FNA has been the gold standard until recently, the technological advancement is implacable and the future will inexorably belong to an improved FNB needle. Still, due to the lower costs of the FNA needle and to a relatively high diagnostic yield, the aspiration needle has a long way to go.