
Heart failure (HF) is a progressive syndrome associated with a high risk of death, frequent hospitalizations, and substantial consumption of healthcare resources. Despite advances in pharmacological and device-based therapies, HF remains one of the leading causes of hospitalization among adults and is associated with poor short- and long-term prognosis [1]. One-year mortality after an HF hospitalization ranges between 15% and 20%, while recurrent admissions are common, exceeding 30%, and often signal disease progression and suboptimal continuity of care [2]. Population aging, improved survival after acute cardiovascular events, and particularly the growing prevalence of the noncardiac comorbidities [3] are expected to further increase the burden of HF hospitalizations worldwide.
Contemporary HF epidemiological reviews reported a prevalence of 1–3% in general adult population, and one-year mortality of ~6–10% [4]. The Global Burden of Disease study reported recently a HF age-standardized prevalence rate of 683 cases per 100,000 people, translating into tens of millions of affected individuals globally [5]. Importantly, HF accounts for a disproportionate share of cardiovascular mortality and disability-adjusted life years, largely driven by repeated hospitalizations and high fatality rates following acute decompensation [6].
In terms of prevalence, incidence, survival, and hospitalization rates of HF, there is considerable heterogeneity between regions, reflecting differences in population structure, risk factor profiles, healthcare organization, and study methodologies [7]. In Europe, the European Society of Cardiology (ESC)/Heart Failure Association (HFA) Atlas provides comprehensive comparative data on HF epidemiology and healthcare utilization [8]. ESC/HFA Atlas reported a median value of HF prevalence of 17.20 (IQR 14.30–21) cases per 1000 people, and a hospitalization rate for HF (primary diagnosis) of 6107 per million. The median number of HF hospitalizations was 2671 (IQR 1771–4317) per million people annually, ranging from < 1000 in Latvia and North Macedonia to >6000 in Romania, Germany and Norway [9].
Romania faces a substantial burden of HF. Previous population-based studies estimated that approximately 4.7% of adults over 35 years present this condition [10]. In a secondary analysis including national data from ESC-HF-Long-Term Registry, approximately one-third of Romanian patients hospitalized for HF either die or are readmitted for HF within one year of follow-up; the one-year HF readmission rate is 15.2%, the one-year all-cause mortality rate is 24.4%, and the combined outcome rate is 35.8% [11]. In the Romanian Acute Heart Failure Syndromes (RO-AHFS) registry, in-hospital all-cause mortality was 7.4%, and the mean length of stay was 7.3 +/-3 days [12].
However, Romania, like many other European countries, lacks a national HF registry with continuous enrollment, and available evidence is largely derived from time-limited registries, which may not fully capture the real-world national burden of the disease. In this context, routinely collected administrative hospital data represent a valuable and underutilized source of epidemiological information. Retrospective analyses of diagnosis-related group (DRG) databases allow comprehensive national coverage over extended periods, enabling the assessment of hospitalization volumes, patient demographics, outcomes, and temporal trends, including the impact of major system-level crises such as the COVID-19 pandemic.
This study was designed as a national, multiannual, retrospective analysis of HF hospitalizations in Romania, using aggregated DRG reimbursement data reported by all public and private hospitals between 2017 and 2022. By examining hospitalization rates, age distribution, length of stay, in-hospital mortality, and readmission frequency before and during the COVID-19 pandemic, this research aims to provide a comprehensive overview of the hospital burden and outcomes associated with HF at the national level. The principal advantages of this study include large sample size, population-level representativeness, and feasibility in settings where prospective registries are unavailable. Quantifying the magnitude of HF-related hospitalizations, mortality, and recurrent admissions can support the development of national HF prevention and management strategies, including early detection, optimization of guideline-directed medical therapy, structured discharge pathways, and integrated post discharge follow-up. In a healthcare system facing demographic aging and constrained resources, such evidence is essential to prioritize interventions that may improve survival, reduce avoidable hospitalizations, and mitigate the long-term clinical and economic impact of HF in Romania.
This retrospective real-world study used national-wide aggregated data from all hospitals, public and private, reporting the minimum patient level dataset for DRG based reimbursement to the National Institute for Health Services Management (INMSS) (Table 1). Romanian national health care services and Hospital DRG-based financing were previously described in another paper [13]. RO DRG V1, the diagnosis coding system for hospital cases, was established in 2010, primarily for DRG classification and reimbursement purposes [14].
Number of hospitals included in the analysis, number of hospitals reporting DRG data, and number of hospitals reporting one-year readmission frequencies.
| Year | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|---|---|
| Total number of hospitals in Romania* | 535 | 524 | 532 | 541 | 543 | 544 |
| Number of hospitals reporting DRG data | 505 | 508 | 517 | 514 | 526 | 528 |
| Number of hospitals reporting HF readmission frequencies | 356 | 352 | 357 | 345 | 348 | 363 |
Reference 15
INMSS oversees the collection of anonymized patient data including age, sex, length of hospital stay, primary or secondary diagnoses, surgery or other procedures and vital status at discharge [14].
In the current analysis, we included the aggregated data covering hospital episodes (length of hospital stay) and hospitalized patients, as reported to INMSS by all public and private hospitals in contract with the National Health Insurance House (NHIH). Eligible HF patients were of any age, and had a primary and/or secondary HF diagnosis coded according to ICD-10 AM: I50.0 (Congestive heart failure), I50.1 (Left ventricular failure), I50.9 (Heart failure, unspecified), or I11.0 (Hypertensive heart disease with (congestive) heart failure). Annual data were obtained for the 2017–2022 period. Hospitalizations with less than 24 h in-hospital stay were excluded.
Endpoints: for inpatients, “cases” were defined as hospital episodes (including multiple hospitalizations from the same patient), whereas “patients” represent unique individuals. Age distribution was assessed for the overall HF population across the entire analyzed period and categorized into nine age groups. In-hospital mortality was calculated as the percentage of in-hospital deaths relative to the total number of hospitalizations. Length of hospital stay was defined as the difference between the date of discharge and the date of admission. All-cause and HF-related rehospitalizations were defined as readmission episodes for any reason, and for HF respectively. Frequency of readmissions were calculated as the percentage of rehospitalization, any diagnosis, and HF diagnosis, for each annual cohort of patients admitted with a primary diagnosis of HF (number of hospitalization episodes in the following years divided by the number of HF patients in each annual cohort). Readmission frequencies were calculated for 2017, 2018, 2019, 2020, and 2021 cohorts.
We used Microsoft Excel for descriptive statistical analysis. Continuous variables were expressed as mean ± standard deviation or median and interquartile range (IQR), and categorical variables as absolute numbers and corresponding percentages. Categorical variables, in-hospital mortality and annual proportions of hospitalization of total number of cases, were compared by the chi-square test. Annual hospitalization counts from 2017–2019 were pooled and compared with pooled counts from 2020–2022 using a binary time-period indicator (pre-pandemic vs. pandemic). For each outcome, total hospitalizations, any HF hospitalizations, and HF hospitalizations with HF as the primary diagnosis, the odds of hospitalization during 2020–2022 were divided by the odds during 2017–2019 to obtain the OR. Odds ratios and corresponding 95% confidence intervals (CIs) were estimated using logistic regression models with time period as the independent variable.
Comparisons in statistical analysis were produced using SAS release 9.1 (SAS Institute, Inc., Cary, NC, USA), R (R Core Team, 2020). A threshold for significance was set at a p-value of .05
Patients’ informed consent and additional review by the Ethics Committee were not required, because all data were de-identified, and no medical product was in scope. The present study complies with the Declaration of Helsinki.
Between 2017 and 2022, over 500 public and private hospitals (ranging from 505 to 528 hospitals) annually reported DRG cases for any diagnosis, while a number of 345–363 hospitals reported hospitalizations with a HF primary and/or secondary diagnosis, indicating broad national coverage and consistent participation across years (Table 1).
During the pre-pandemic period (2017–2019), more than 4 million hospitalizations (cases) for all diagnoses were reported each year (Figure 1). Total hospital cases decreased to approximately 2.5 million in 2020–2021, with partial recovery in 2022. The overall volume of hospital activity showed a 39% decline during the COVID-19 pandemic (Figure 2). A similar but more pronounced pattern was observed for HF hospitalizations. HF cases declined from 553,084–591,479 annually before the pandemic to 311,900–318,274 during 2020–2021 (–45%), increasing again to 432,473 in 2022 (Figure 2). HF, as primary and secondary diagnosis, represented a substantial proportion of hospital activity, accounting for 12.3–14.3% of all hospital cases across six-year of follow-up. During 2017-2019 approximately 100,000 hospital admissions were reported with a primary diagnosis ICD-10 code for Heart Failure (I50.0, I50.1, I50.9, I11.0) and decreased by a half during 2020-2022. Hospitalizations for HF as primary diagnosis, represented 1.8-2.7% (2.3% on average) of total hospital cases and 16-20% of total HF hospitalizations (primary and secondary diagnosis).
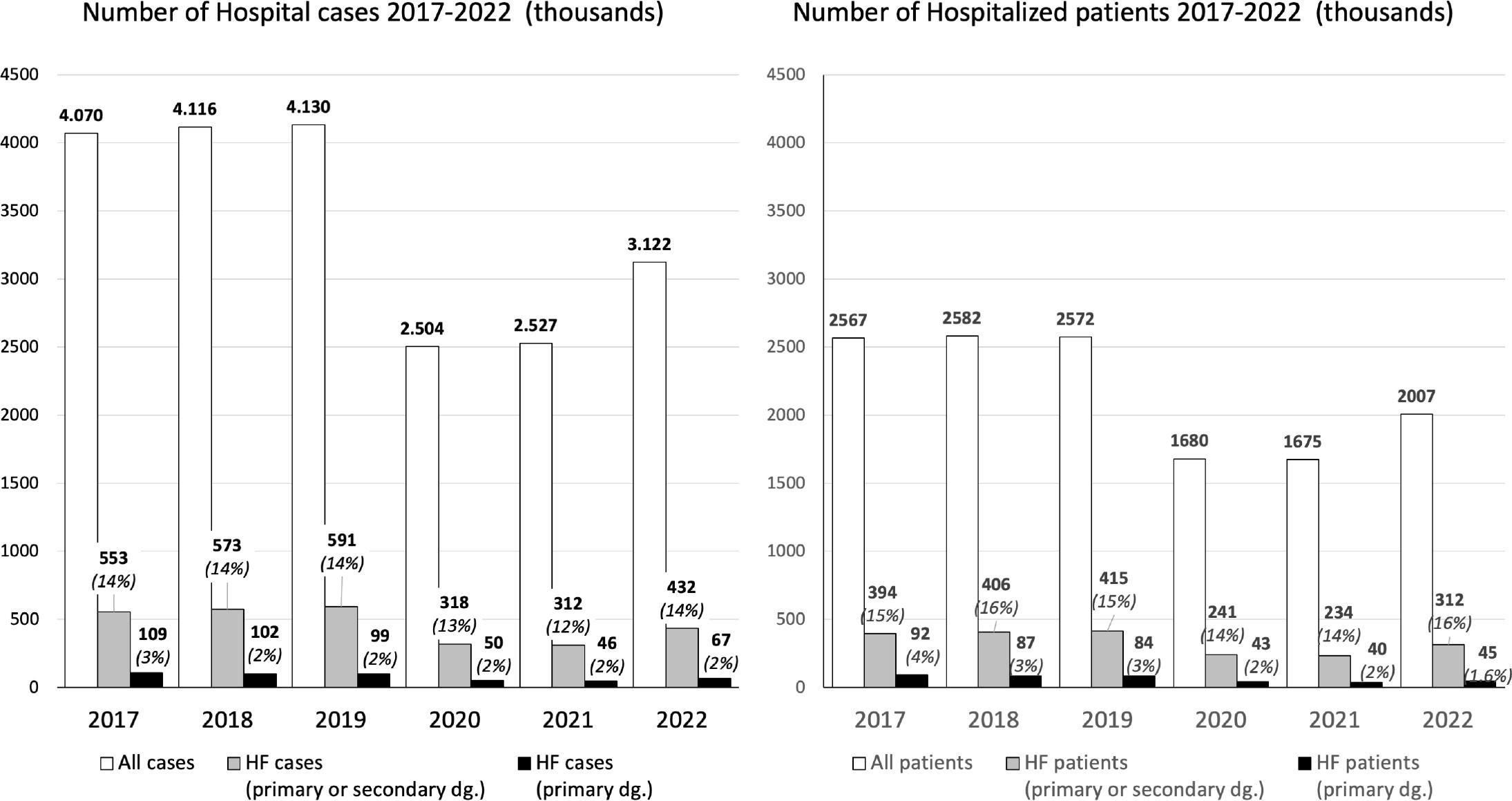
A. Hospital cases, all cases, and HF* cases, time period 2017–2022 (thousands); B. Unique patients, all patients, and HF* patients, time period 2017–2022 (thousands).
*ICD-10 code for Heart Failure diagnosis I50.0, I50.1, I50.9, I11.0.
Proportions represent percentages out of all cases or all patients.
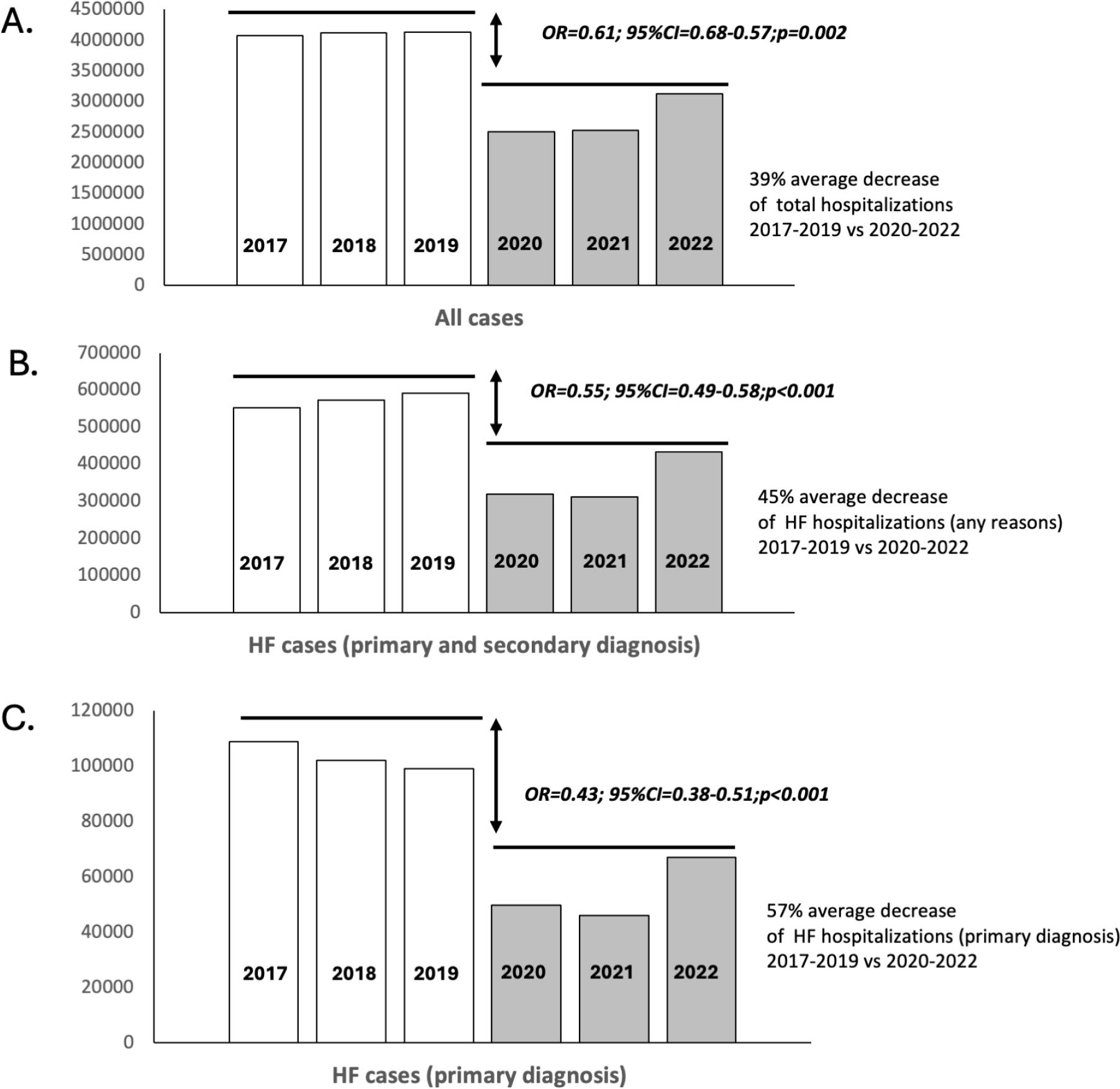
A. Comparison between 2017–2019 vs. 2020 for total hospitalizations; B. HF hospitalization (any cause); C. HF hospitalizations with HF as primary diagnosis.
“For each panel (A, B, and C) in Figure 2, odds ratios (ORs) were calculated to compare hospitalization volumes during the pre-pandemic period (2017–2019) with those during the pandemic period (2020–2022). ORs <1 indicate a reduction in hospitalizations during 2020–2022 compared with the 2017–2019 reference period.”
Abbreviations: OR=odd ratio; CI =confidence interval
Trends in hospitalized patients mirrored those observed for cases (Figure 1). The number of HF patients decreased from approximately 394,000–415,000 annually before the pandemic to 234,529–240,710 during 2020–2021, with an increase to 312,095 in 2022 (Table S3). HF patients consistently represented 14.0–16.1% of all hospitalized patients. Pediatric HF patients accounted for a very small fraction of the total (<0.5% annually). Among adults hospitalized with a primary HF diagnosis, both cases and patients declined sharply during the pandemic, from 108,726 cases and 92,155 patients in 2017 to 49,869 cases and 43,717 patients in 2020, followed by partial recovery in 2022 (Figure 1). When accounting for both indicators, “HF cases” and “HF patients”, the annual reports show an average rate of 1.4 hospital episodes per HF patient.
Mean age was 70.1 (+/- 10.4) years. Analysis of age distribution for the entire 6-year period (n=1,658,600) demonstrated that hospitalizations for HF predominantly affected older adults (Figure 3). Throughout the period 2017–2022, 69.4% of patients with HF were aged ≥65 years, with the largest groups being 65–74 years (32.1%) and 75–84 years (28.5%). Nevertheless, 30% of hospitalized HF patients were younger than 65 years, while pediatric patients accounted for only 0.4%.
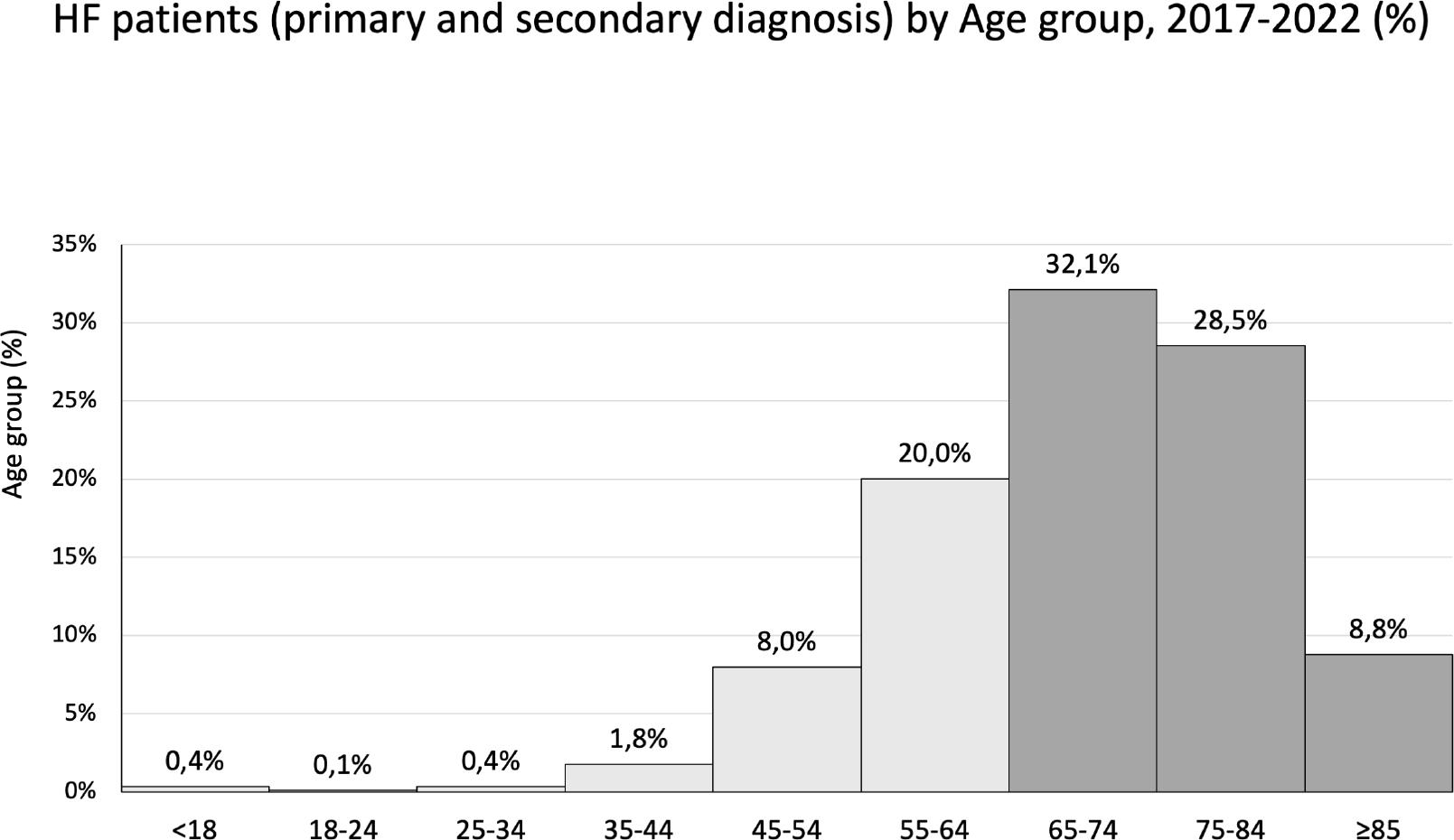
HF patients by age group, period 2017–2022.
In-hospital mortality was significantly higher for “HF cases” than for “all hospital cases” for each year (Figure 4A). Before the pandemic, in-hospital mortality for patients hospitalized for HF ranged between 4.0% and 4.3%, about double that of all cases (1.9–2.0%). During the pandemic, HF mortality increased markedly to 8.1% in 2020 and 9.8% in 2021, remaining elevated at 6.8% in 2022. Mortality increased steeply with age, with the highest number of HF-related in-hospital deaths occurring in patients aged ≥75 years (10% in group 75–84 years and 17% in group >85 years) (Figure 4B). Except for the 18–24 age group, in-hospital mortality for HF cases was significantly higher during the pandemic than before, for every decade.
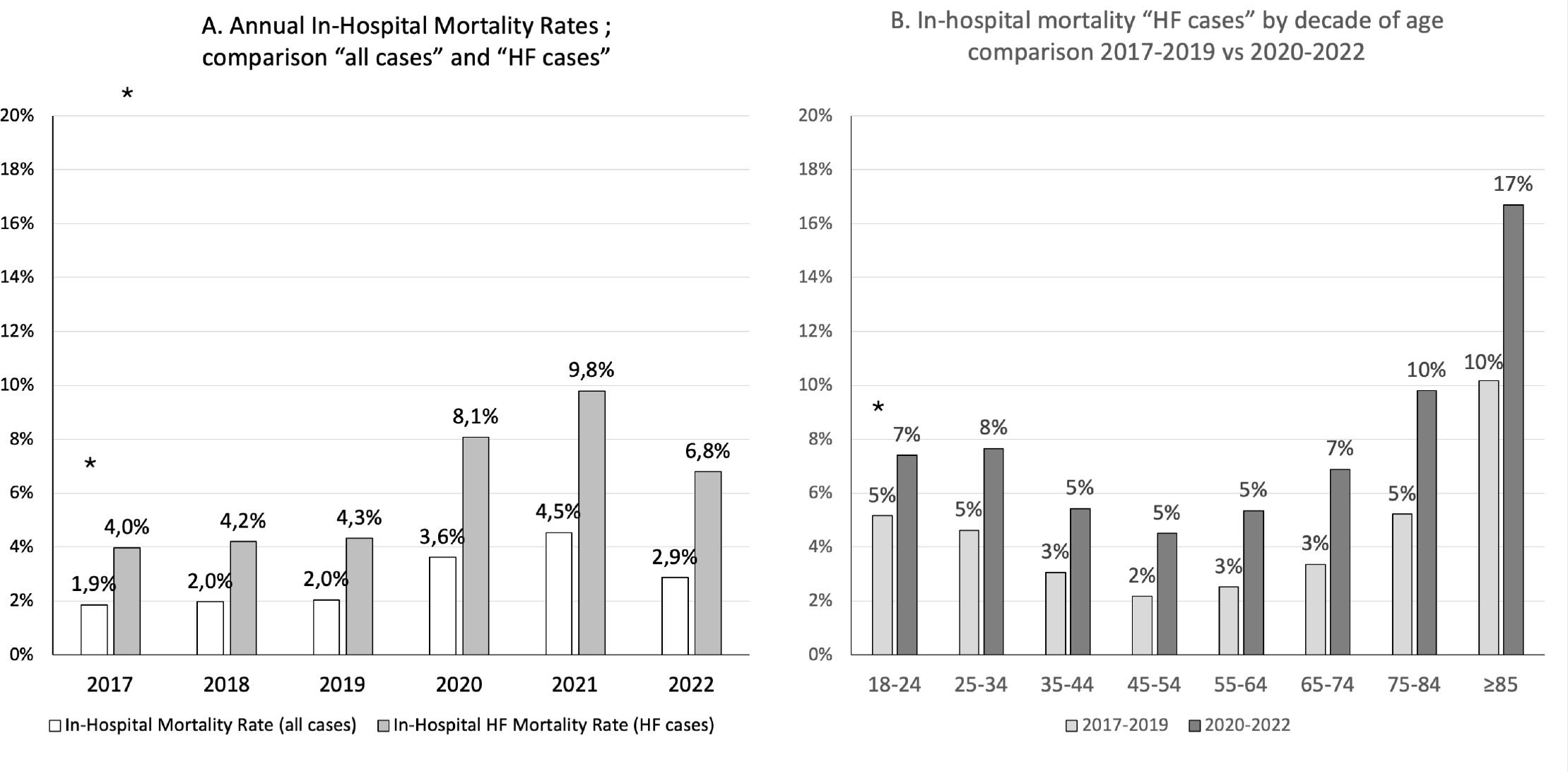
A. Annual in-hospital mortality rates; comparison of “all cases” vs. “HF cases” (p<0.001 for each year); B. In-hospital mortality HF cases by decade of age; comparison of 2017–2019 vs. 2020–2022 (p<0.001 for age category >25 years).
The mean and median length of hospitalization for patients with HF was 6.7 days and 6 days, respectively.
Among cohorts hospitalized with HF as the primary diagnosis, analyses of subsequent admissions demonstrated a substantial burden of rehospitalizations during follow-up (Figure 5; Supplementary Tables). However, the majority of these events were due to causes other than HF. Within the first year after index hospitalization, nearly all patients in the 2017 cohort experienced at least one all-cause readmission, whereas only 22% were hospitalized with HF as the primary diagnosis. A similar pattern was observed in the 2018 cohort, with 94% of patients having at least one all-cause readmission and 20% attributable to HF. In later cohorts, both all-cause and HF-specific readmissions declined markedly: in 2019, 51% of patients were readmitted for any cause and 10% for HF; in 2020, corresponding figures were 28% and 6%; and in 2021, 35% and 7%, respectively. Overall, HF readmissions with HF as the primary diagnosis accounted for approximately 5–22% of one-year all-cause readmissions, underscoring the predominance of non-HF causes in post-discharge hospital utilization among HF patients. Although the frequency of readmissions for any-cause and HF decreased in subsequent years of follow-up and during the pandemic cohorts, it remained substantial, highlighting the chronic and recurrent nature of hospital care associated with HF.
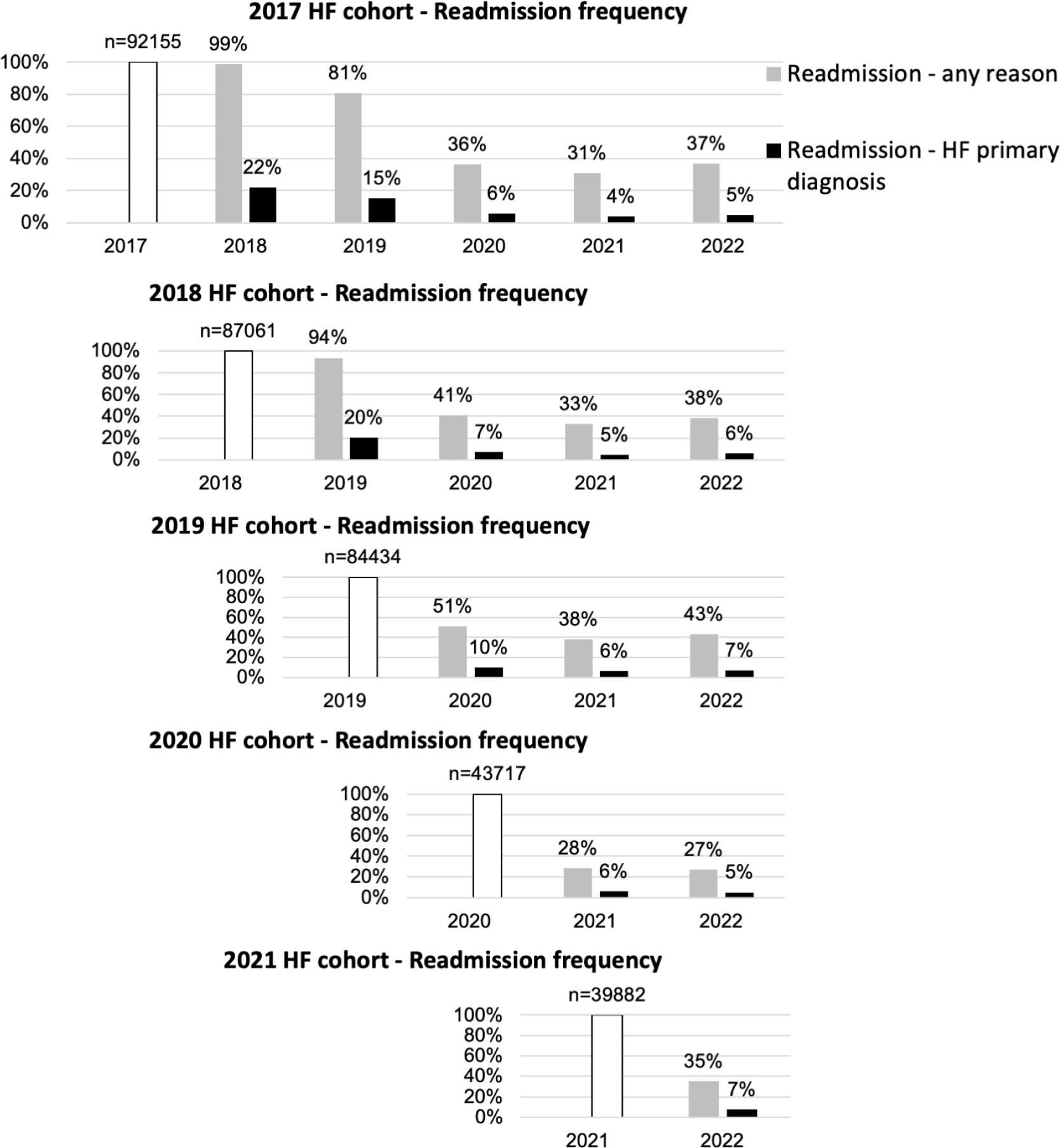
Frequency of readmissions for each annual cohort of patients admitted with a primary diagnosis of HF for 2017–2021; HF readmission frequency for any reason; and for HF primary diagnosis.
This national, multi-year analysis provides a comprehensive, real-world assessment of hospitalization patterns for HF in Romania and confirms that HF is a major and persistent driver of hospital utilization, mortality, and readmissions. By leveraging mandatory DRG-based reporting from >95% of Romanian hospitals over a six-year period, the study provides robust population-level evidence in a healthcare setting.
Several key findings emerge from this analysis. Firstly, HF represents a substantial proportion of hospital activity in Romania (at a general population of 19 million) [15], accounting for up to 14% of all inpatient cases and affecting on average 400,000 patients annually. Primary HF diagnosis accounted for 15–20% of total HF hospitalized cases (HF primary and secondary diagnosis), and 1.8–2.7% (mean 2.3%) of total hospital cases, with a decreasing trend over the last six years. Secondly, hospital care for HF is characterized by frequent recurrent admissions, with an average of 1.4 hospitalization episodes per patient per year, and very high rates of readmission after discharge. Over 20% of hospital readmissions after one year were related to HF as the primary diagnosis. Thirdly, outcomes remain poor, as in-hospital mortality for HF is consistently double that of the general hospitalized population. Finally, although HF predominantly affects older adults, nearly a third of hospitalized patients were under 65 years of age, highlighting a significant burden on the working-age population.
The COVID-19 pandemic had a profound impact on HF hospital care in Romania. HF hospitalizations declined by approximately 45% during 2020–2021, a more pronounced reduction than that observed for the total number of hospital admissions. This likely reflects a combination of restricted access to care, patients’ reluctance to seek medical attention, and reallocation of hospital resources to COVID-19 services [16]. It is important to note that this reduction in hospitalizations was accompanied by a significant increase in in-hospital HF mortality, which doubled during the pandemic years (8–10% during the pandemic compared to 4% in the pre-pandemic years) and remained high thereafter. These findings suggest delayed presentation, higher clinical severity at admission, and possible direct or indirect effects of SARS-CoV-2 infection on cardiovascular outcomes [16]. Similar trends have been reported across Europe, supporting the concept that HF patients were highly vulnerable during the pandemic.
The Romanian findings are largely consistent with international data, while also revealing distinct national patterns. HF hospitalization rates in Romania are among the highest reported in Europe, comparable to Germany and Norway and higher than those observed in Denmark or France. Country specific rates of hospitalization for HF, as percentage of general population, have been previously reported in Germany (4600–6000 per million) [17, 18], in Denmark (1000 per million) [19], and France (2500 per million) [20].
The proportion of HF cases (as primary diagnosis) among total hospitalizations (2.3% in Romania) aligns with data from Germany (1.4–2.3%) [15], but lower than in Slovenia (6.5%) [21]. When both primary and secondary HF diagnoses were considered, HF accounted for 14% of all hospital cases. A similar research analysis, coming from the Czech Republic in 2000, reported 25% for the ratio between HF cases and total hospital cases [22]. When considering the hospitalization rate per HF patient, the ratio observed in the current analysis (1.4) was comparable to that reported in Germany during 2009–2013 (1.8 hospitalizations/patient over two years) [23].
Romanian HF patients appear younger than those in Western European cohorts, where mean ages often exceed 75–80 years. In Germany in 2017, three-quarters of HF patients were >75 years. The mean age of HF patients was 80.1 years in Spain for 2011–2015 [24]; 78 years in France in 2012 [17]; 76.6 years in Sweden for 2010–2015 [25]; and 77.8 years in Norway for 2000–2014 [26].
Hospital stay was shorter than in several other countries, possibly reflecting differences in care pathways, bed availability, or different thresholds for hospital admission. The length of hospital stay for HF cases in this study (7 days) is similar with the one reported in Spain for 2013–2015 [27], and shorter than in Germany (10.2 days in 2017) [14], France (10 days in 2012) [17], Poland (9.6 days in 2016) [28], and Slovakia (9.4 days in 2015) [24].
In-hospital mortality for HF cases (fatality rate) varies largely among European countries: from 3.9% in Hungary in 2017 [29], 6.2% in Slovakia in 2015 [30], and 9.5% in Germany for 2005–2016 [15], to 11.5% in Poland in 2016 [31], and 12–13% in Spain for 2001–2015 [21].
One-year hospital readmission frequencies were extremely high and comparable to those reported in Spain (>96%) [17], Sweden (65%) [32], and Italy (57%) [33], underscoring the chronic and relapsing nature of HF across healthcare systems.
The combination of high admission volumes, recurrent hospitalizations, and elevated mortality translates into a major and sustained burden on the Romanian healthcare system. HF consumes substantial hospital capacity and financial resources. The financial burden of chronic HF in Romania was recently explored. In 2019, the weighted average cost per HF inpatient was EUR 1002, with a national budget impact was EUR 376 million, representing 4.4% of the total NHIH budget [34]. In working-active categories, the societal cost associated with duration of hospital stay and medical leave was EUR 122 million.
The extremely high frequency of post-discharge readmissions, including a significant proportion directly attributable to HF, underscores persistent gaps in continuity of care, outpatient management, and HF prevention. Limited access to multidisciplinary outpatient HF programs, lack of the structured post-discharge follow-up, and fragmentation between hospital-based and ambulatory care, likely contribute to recurrent admissions. Health system characteristics, including low thresholds for hospitalization and reliance mainly on inpatient care, may also explain these findings. Close post-discharge follow-up and treatment optimization represent a window of opportunity in HF management [35]. Also, reducing avoidable HF hospitalizations via primary and secondary prevention measures should be a national priority [36]. To note, none of the IV therapies used to treat congestion during HF have been associated with reducing number of hospitalizations [37–39]. Earlier diagnosis, coupled with etiological-based treatment of HF, including medical, interventional, and surgical therapies, have been shown to reduce HF hospitalizations and CV mortality [40–46]. Broader implementation of guideline-directed medical therapy [47], identification and treatment of non-cardiac comorbidities [3], structured discharge planning, and closer post-discharge follow-up [35] represent evidence-based strategies to decrease hospitalization rates. Although these could be achieved by integration of HF patients in multidisciplinary programs, improved coordination between hospital and primary care may help to prevent recurrent admissions. The development of HF multidisciplinary programs based on the most common comorbidities is ly important, considering higher proportion of non-HF-related hospitalizations reported in this study. Similarly, evidence from both European [48] and US [49] administrative datasets demonstrates that HF is coded as a secondary diagnosis in the majority of hospitalizations involving HF patients, accounting for approximately 58–72% of all HF-related hospital admissions. In these cases, HF most often represents a major comorbidity or precipitating condition rather than the primary reason for admission. The most frequent principal causes of hospitalization when HF is coded as a secondary diagnosis include respiratory diseases, infections, oncology-related admissions, and non-cardiac surgery [48, 49]. Targeting younger HF patients may also yield substantial socioeconomic benefits.
Notably, in July 2025, the Romanian Government adopted “The National Strategy for Management of Cardiovascular and Cerebrovascular Diseases” [50], aiming to combat rising deaths and disabilities from heart diseases by focusing on integrated data systems, improved diagnostics, rehabilitation, workforce development, and research. This strategy involves multiple domains, prevention, early detection, and treatment, with a key goal to reduce avoidable mortality by 5% by 2030.
While administrative DRG data provide valuable epidemiological insights, future research should focus on establishing longitudinal national HF registries capturing clinical characteristics, treatments, and long-term outcomes. Such registries would enable evaluation of quality of care, adherence to guidelines, and effectiveness of integrated HF management strategies. In the context of Central and Eastern Europe, combining administrative data with prospective observational studies based on consecutive enrolment [51] represent a critical step toward improving HF outcomes and health system performance.
The current analysis is based on a national administrative database which collects discharge reports. Consequently, it lacks granularity of in-hospital clinical data (e.g., HF etiology, phenotype, disease severity, or treatment). Overall, in administrative datasets, the validity for HF diagnosis varies, with high specificity—most recorded cases represent true HF—but low sensitivity, as many true cases are missed or underreported. Also, it has restricted ability to assess long-term outcomes beyond hospital readmissions. However, the general in-hospital admissions and in-hospital death figures are in line with a recent report in the context of COVID-19 pandemic [52].
The accuracy of the reports relies on the data entered by the contributing hospitals, and although all hospitals are using a standard DRG system, coding accuracy has not been centrally validated. The data are limited to in-hospital “HF cases” and “HF patients”, and cannot provide information for HF patients with a hospital stay of less than 24 hours or for HF patients who present in ambulatory offices for worsening HF.
The readmission figures for HF patient cohorts were reported as frequency instead of rate, possibly overestimating any-cause readmissions. Also, the current analysis is based on aggregated administrative data, and we were unable to calculate patient-level readmission rates or time-to-event outcomes.
No statistical inferences can be drawn from this study, since methodology involved only data collected at discharge.
Additional meaningful clinical indicators for HF patients could be collected only by longitudinal cohort studies and reliable HF registries.
This national, multiannual analysis demonstrates that HF represents a major and sustained burden on the Romanian hospital system, both before and after the COVID-19 pandemic. HF accounted for a substantial proportion of total hospitalizations, affecting predominantly older adults but also a considerable working-age population, and was associated with prolonged hospital stays, high in-hospital mortality, and very frequent readmissions. Although overall hospital admissions declined markedly during the pandemic, HF-related mortality increased and remained elevated thereafter, highlighting the vulnerability of this population and potential delays or barriers in access to care. In the absence of comprehensive national HF registries, routinely collected DRG data provide valuable real-world insights into disease burden and outcomes at the population level. These findings support the urgent need for coordinated national strategies focused on early diagnosis, guideline-directed therapy, and integrated follow-up programs to reduce preventable hospitalizations and mitigate the long-term clinical and economic impact of HF in Romania.