
Figure 1
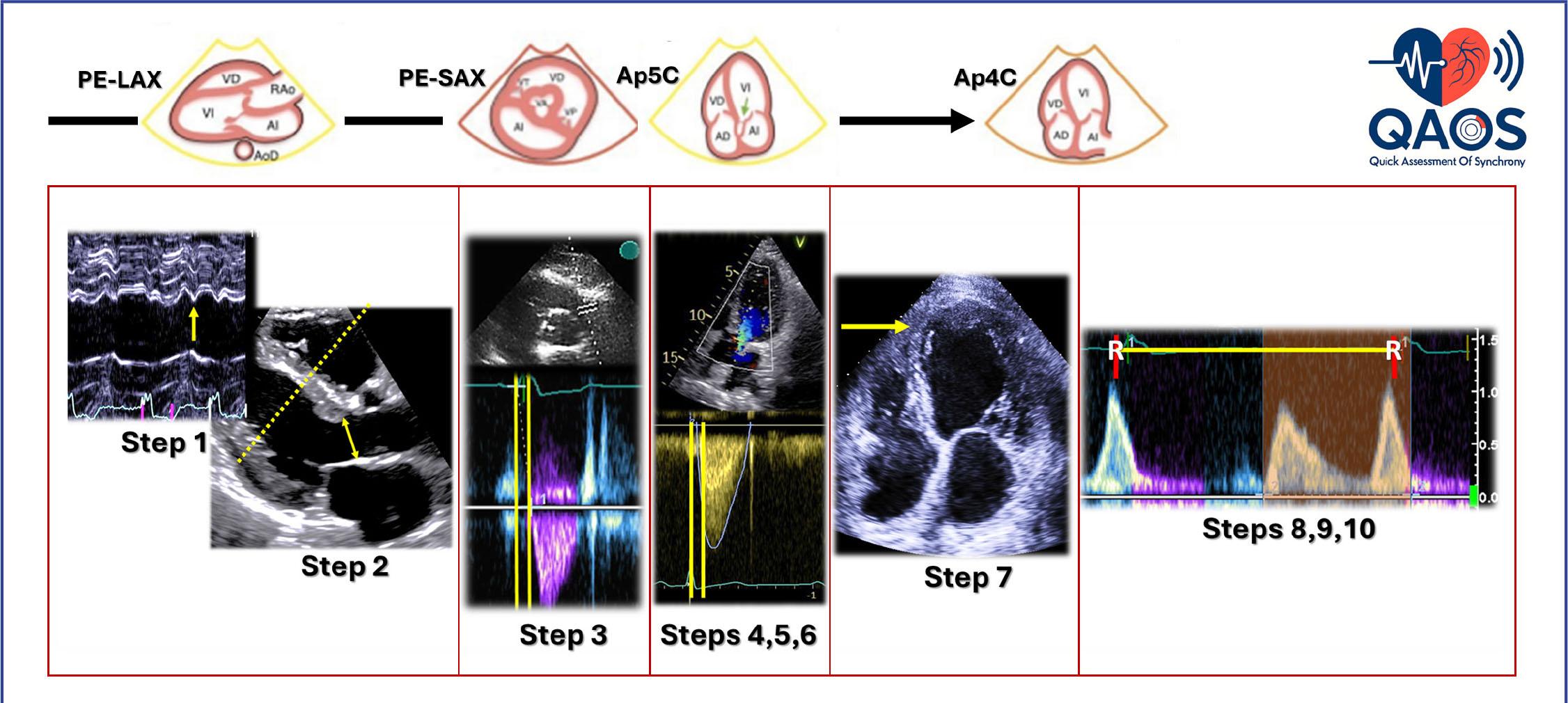
Figure 2
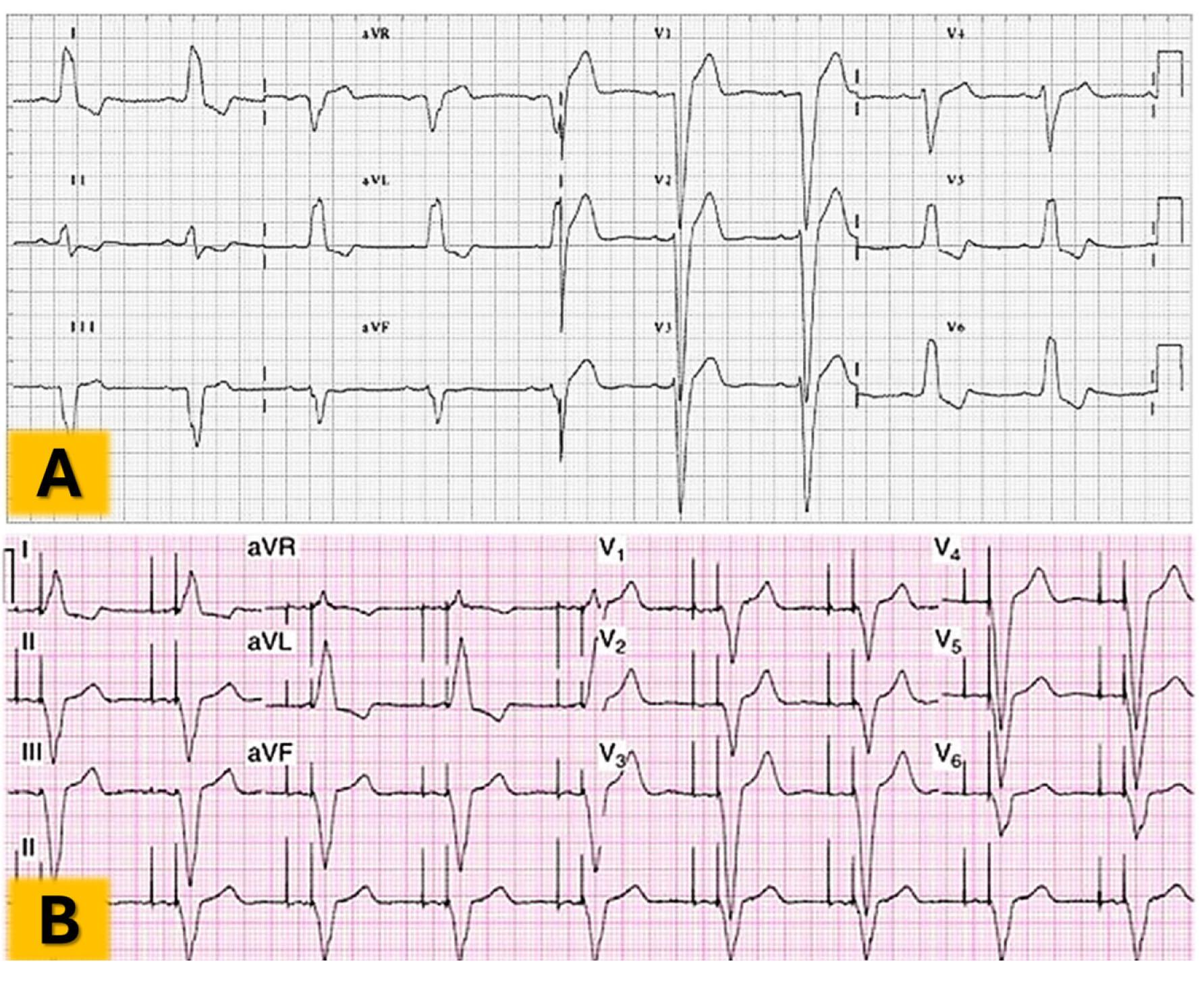
Figure 3
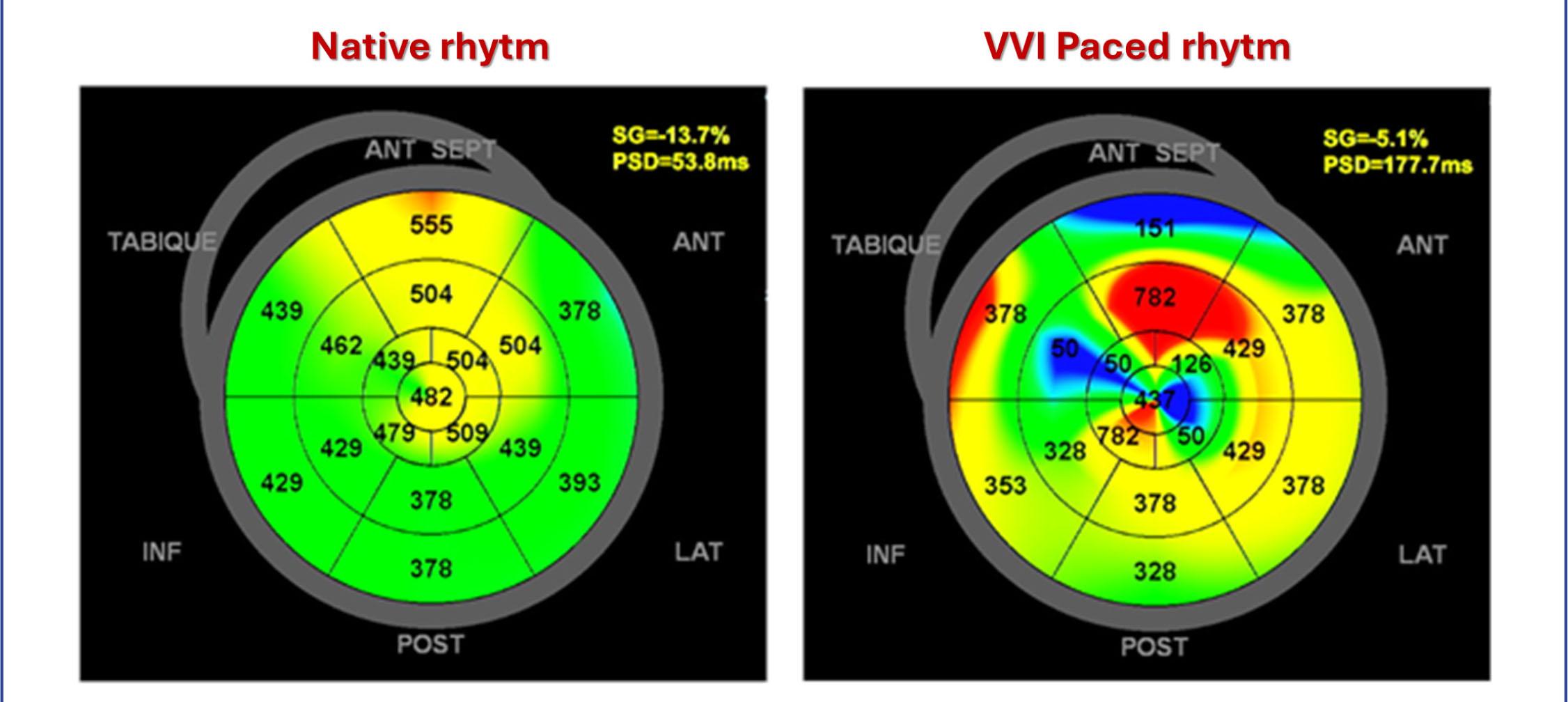
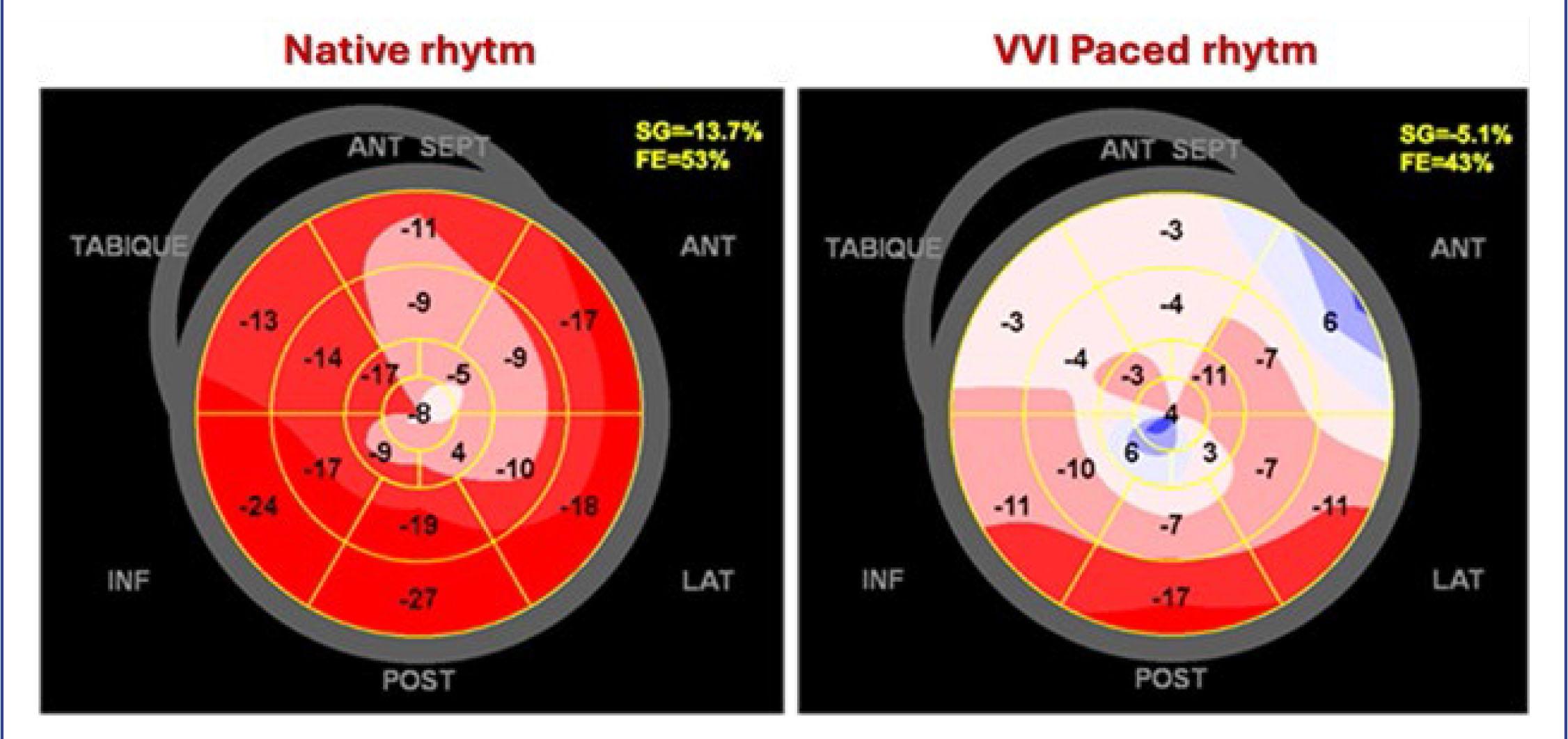
Figure 4
Comparative Analysis with QAOS Protocol: two cases of patients with pacemakers_
| Case A Male, 85 years old Ischaemic heart disease | Case B Male, 68 years old Non-ischaemic heart disease | |||
|---|---|---|---|---|
| Heart failure symptoms? | NYHA Class II | NYHA Class II | ||
| RV pacing % | 62.3% | 55% | ||
| Heart Rythm | Native Sinus | VVI | Native Atrial Fib. | VVI |
| LVEF (%) | 58% | 56% | 48% | 37.9% |
| Global Longitudinal Strain (%) | -16.4% | -12.5% | -24.2% | -15.5% |
| QAOS Step 1: Septal flash? (Yes/No/Not evaluable) | No | Yes | No | Yes |
| QAOS Step 2: LVOT area (cm2) | 2.27 cm2 | 3.14 cm2 | ||
| QAOS Step 3: VD pre-expulsive period (ms) | 55 ms | 116 ms | 88 ms | 94 ms |
| QAOS Step 4: LV pre-expulsive period (ms) | 87 ms | 176 ms | 88 ms | 138 ms |
| QAOS Step 5: Interventricular delay (ms) | 32 ms | 60 ms | 0 | 44 ms |
| Interventricular synchrony? (Y/N) | Yes | No | YES | No |
| QAOS Step 6: LVOT VTI (cm) | 25.2 cm | 14.5 cm | 17 cm | 14 cm |
| LV stroke volume (ml) | 56 ml | 32 ml | 51.5 ml | 44 ml |
| QAOS Step 7: Rocking apex: (Yes/No/Not evaluable) | No | Yes | NO | Yes |
| Intraventricular synchrony? (Y/N) | YES | No | YES | NO |
| QAOS Step 8: R–R interval (ms) | 1005 ms | 1000 ms | 822 | 740 ms |
| QAOS Step 9: Mitral diastolic flow duration (ms) | 614 ms | 382 ms | 391 | 254 ms |
| QAOS Step 10: Mitral diastolic flow duration ÷ R–R: (%) | 61.1% | 38.2% | 47.6% | 34.3% |
| A-V Synchrony? (Yes/No) | Yes | No | Yes | No |
| Can PIC be diagnosed? | NO | YES | ||
| Is there a need for a pacemaker upgrade? | NO | YES | ||