
The primary goals of permanent cardiac pacemaker implantation have traditionally been, first and foremost, to save lives, and in less critical cases, to improve quality of life. More recently, there has been growing consensus around a third, equally important objective: to preserve cardiac synchrony — or, alternatively stated, to prevent or treat established dyssynchrony — in order to avoid left ventricular dysfunction, which can lead to heart failure. Optimal mechanical performance of the heart requires an intact impulse generation and conduction system, both structurally and functionally. Any pathological condition affecting this system results in non-physiological cardiac activation, thereby reducing global mechanical efficiency [1].
Chronic artificial stimulation of the right ventricle has been a common practice since the earliest intracavitary electrode implants. This is for several reasons: it offers direct and safe venous access (via the subclavian vein); the implantation procedure is relatively simple; and essential ventricular stimulation is guaranteed in single-lead systems. However, this approach comes at a cost — especially when the lead is positioned at the right ventricular apex. The ventricular activation front generated by a pacemaker resembles that of advanced left bundle branch block, with delayed electromechanical activation of the left ventricular free wall. This dyssynchronous contraction ultimately leads to heart failure[2] through various mechanisms — even in dual-chamber pacing modes [3].
Several studies have addressed this issue. The first study specifically designed to demonstrate it dates back to the HOBIPACE trial[4] in 2006, which focused on ventricular function, exercise tolerance, and quality of life. The BLOCK-HF study, involving patients with a baseline left ventricular ejection fraction (LVEF) below 50%, showed that biventricular pacing led to reduced cardiac remodeling, heart failure, and overall morbidity and mortality compared to exclusive right ventricular pacing [5]. Gage, Burns, and Bank reached similar conclusions in a 2014 publication [6].
The cited evidence supports the existence of a distinct clinical entity: Paced-Induced Cardiomyopathy (PIC), defined by the 2023 HRS/APHRS/LAHRS guidelines as a reduction in left ventricular ejection fraction (LVEF) to below 50%, with an absolute decrease in LVEF greater than 10%, a ventricular pacing burden of at least 20%, and no other identifiable causes of heart failure following device implantation. [7] Kim et al. argue that while the drop in LVEF is a key criterion, the emergence of new heart failure symptoms, hospitalization, and/or new-onset atrial fibrillation should also be incorporated into the PIC concept, even though PIC may occur in the absence of overt left-ventricular failure symptoms[8].
Regarding its incidence, a recent multicenter study by Somma et al. — a meta-analysis of 26 studies including approximately 57,993 patients — reported a 12% incidence of new PIC cases (range: 6–39%) over a follow-up period ranging from 0.7 to 16 years [9. Reported incidence rates are expected to vary depending on the criteria used to define PIC and the duration of follow-up. [8]
Several risk factors have been studied in relation to PIC development [8]:
- -
Advanced age.
- -
Male gender. [10]
- -
Pre-implantation atrial fibrillation. [11]
- -
Reduced LVEF.
- -
Prolonged QRS duration [10].
- -
Diastolic dysfunction.
- -
Abnormal global longitudinal strain.
- -
Complete AV block as the indication for pacemaker implantation [11].
- -
Ventricular pacing burden greater than 40%.
Chronic kidney disease and myocardial infarction have also been proposed as contributing risk factors [12].
Regarding pacing burden, Kiehl et al. suggest that heart failure risk increases once pacing burden reaches 40%, showing a linear correlation between pacing percentage and the onset of atrial fibrillation, even when AV synchrony is preserved with DDD pacing[13]. Sweeney et al. also propose 40% as a threshold for increased heart failure risk (OR: 2.5).[3
Relative risks of all-cause mortality and new-onset heart failure in PIC patients have been compared to those in pacemaker recipients without PIC (Cho et al. [14]). Auger et al. [15] conducted a similar analysis using a dyssynchrony index. Both studies independently demonstrated significant increases in all-cause mortality and heart failure. The DAVID trial [16] also showed that unnecessary DDD pacing led to higher morbidity and mortality compared to backup-only pacing.
Although conduction system pacing has emerged as a physiological strategy aimed at preserving normal ventricular activation through left bundle branch capture (left bundle branch pacing, or LBBP), recent studies warn that this modality is not exempt from the risk of inducing ventricular dyssynchrony. In a contemporary cohort, a 3.75% incidence of newly-developed left ventricular dysfunction following LBBP was reported (Ponnusamy et al. [17). Moreover, the distinction between left ventricular septal pacing (LVSP) and LBBP — in terms of synchrony — is not always clinically evident, although some parameters, such as QRS area reduction, suggest a slight superiority of LBBP in achieving more physiological ventricular activation (Heckman et al. [18]).
Accumulated evidence on pacing-induced cardiomyopathy (PIC) reveals that electrical and mechanical dyssynchrony — typically associated with “conventional” right ventricular pacing — can trigger ventricular remodeling, fibrosis, and progressive deterioration of left ventricular ejection fraction, even in patients without preexisting structural heart disease (Mizner J[19], Ferrari ADL[20]). Therefore, given the diversity of techniques and outcomes within conduction system pacing — particularly in the left bundle branch region — it is essential not to assume that physiological pacing guarantees complete synchrony.
In the present study, beginning in January 2024, 24 patients of both sexes in El Salvador (ten female, mean age 74.9 + 10.9 years, seven with cardiac resynchronization devices, and two with left bundle branch pacing) were selected for a prospective pilot study on the incidence of PIC. The protocol has been carried out during device follow-up visits, scheduled at least annually, except in cases of heart failure symptoms. Follow-up is expected to continue at least through January 2026; however, two patients have already been diagnosed with PIC, with one of them requiring an upgrade from DDDR to left bundle branch pacing, and the other is still awaiting upgrade. We have registered one death that was not related to cardiac disease. The implementation of the study, under the author’s supervision, has proceeded efficiently and without significant obstacles.
Based on these considerations, the author proposes a protocol for all patients who already have an implanted device, regardless of modality, with the aim of identifying criteria for lost and / or restored synchrony, as well as documenting potential impairment and / or recovery of clinical markers and left ventricular function. This protocol has been named QAOS (Quick Assessment Of Synchrony), and the primary objective of this paper is to make it available to physicians involved in the care of patients with pacemakers. Initially, the goal is to design and carry out local pilot projects based on this protocol. Subsequently, if future clinical trials demonstrate this protocol to be an effective and efficient procedure for widespread clinical use, its definitive implementation will be pursued.
To implement the protocol, a data collection instrument (see Table 1) was designed to capture demographic information; clinical, pacing burden; left ventricular function parameters; hemodynamic data; and atrioventricular, interventricular, and left intraventricular synchrony metrics. All measurements and calculations have been reported as useful tools for dyssynchrony evaluation (see specific references). This instrument may be applied prospectively as needed, and should be included in each patient’s medical record. The minimum required data fields are:
Healthcare facility.
Evaluation date.
Patient identification.
Sex.
Date of birth / age.
Blood pressure (mmHg).
Indication for implantation.
Pacemaker implantation date.
Pacemaker brand and model, as well as pacing modality.
Right ventricular pacing burden.
Comparative Analysis with QAOS Protocol: two cases of patients with pacemakers.
| Case A Male, 85 years old Ischaemic heart disease | Case B Male, 68 years old Non-ischaemic heart disease | |||
|---|---|---|---|---|
| Heart failure symptoms? | NYHA Class II | NYHA Class II | ||
| RV pacing % | 62.3% | 55% | ||
| Heart Rythm | Native Sinus | VVI | Native Atrial Fib. | VVI |
| LVEF (%) | 58% | 56% | 48% | 37.9% |
| Global Longitudinal Strain (%) | -16.4% | -12.5% | -24.2% | -15.5% |
| QAOS Step 1: Septal flash? (Yes/No/Not evaluable) | No | Yes | No | Yes |
| QAOS Step 2: LVOT area (cm2) | 2.27 cm2 | 3.14 cm2 | ||
| QAOS Step 3: VD pre-expulsive period (ms) | 55 ms | 116 ms | 88 ms | 94 ms |
| QAOS Step 4: LV pre-expulsive period (ms) | 87 ms | 176 ms | 88 ms | 138 ms |
| QAOS Step 5: Interventricular delay (ms) | 32 ms | 60 ms | 0 | 44 ms |
| Interventricular synchrony? (Y/N) | Yes | No | YES | No |
| QAOS Step 6: LVOT VTI (cm) | 25.2 cm | 14.5 cm | 17 cm | 14 cm |
| LV stroke volume (ml) | 56 ml | 32 ml | 51.5 ml | 44 ml |
| QAOS Step 7: Rocking apex: (Yes/No/Not evaluable) | No | Yes | NO | Yes |
| Intraventricular synchrony? (Y/N) | YES | No | YES | NO |
| QAOS Step 8: R–R interval (ms) | 1005 ms | 1000 ms | 822 | 740 ms |
| QAOS Step 9: Mitral diastolic flow duration (ms) | 614 ms | 382 ms | 391 | 254 ms |
| QAOS Step 10: Mitral diastolic flow duration ÷ R–R: (%) | 61.1% | 38.2% | 47.6% | 34.3% |
| A-V Synchrony? (Yes/No) | Yes | No | Yes | No |
| Can PIC be diagnosed? | NO | YES | ||
| Is there a need for a pacemaker upgrade? | NO | YES | ||
Subsequently, echocardiographic data will be documented. If left ventricular function indices are normal during pacing, it is not necessary to repeat the measurements in native rhythm. However, if there is any evidence of left ventricular dysfunction in patients who are not fully pacemaker-dependent, measurements and calculations should be performed — both during pacing and in native rhythm — in order to confirm whether the pacing itself is responsible for the dysfunction. Technical support from the device manufacturer may be requested to assist with programmer use.
MAPSE (Mitral Annular Plane Systolic Excursion): This parameter correlates strongly with global longitudinal strain [21], especially when speckle tracking is unavailable. It is measured in the apical four-chamber view (Ap4C) using M-mode.
Left Ventricular Ejection Fraction (LVEF): Ideally assessed using biplane apical or three-dimensional (3D) echocardiography. Automated methods allow averaging over three consecutive cardiac cycles.
Global Longitudinal Strain (GLS): If speckle tracking is available, both average strain and mechanical dispersion should be recorded. If not, the validated HUNT method [22] may be used, with a lower cutoff value (-16%).
The protocol consists of ten steps:
- -
Step 1 - Septal flash detection: Septal flash is a brief septal movement during isovolumetric contraction that is characteristic of left bundle branch block dyssynchrony, but is also observed in patients with right ventricular pacing. It is documented using the M-mode of the anterior septum in the parasternal long-axis view (PLAX), and serves as a reliable dyssynchrony marker[23].
- -
Step 2 - Measurement of Left Ventricular Outflow Tract (LVOT) and calculation of LVOT Area (A-LVOT): These measurements (also in PLAX) are needed to calculate stroke distance and volume.
- -
Step 3 - Right ventricular pre-ejection period: Using pulsed-wave Doppler in the right ventricular outflow tract (RVOT) in the parasternal short-axis view of the great vessels (PSAX), the interval from QRS onset to the start of systolic flow is measured in milliseconds (ms).
- -
Step 4 - Left ventricular pre-ejection period: Using pulsed-wave Doppler in the LVOT, the interval from QRS onset to the start of systolic flow is measured in ms.
- -
Step 5 - Calculation of interventricular delay. To diagnose interventricular dyssynchrony, the right and left pre-ejection periods are subtracted — ideally in both native and paced rhythm. A difference > 40 ms confirms dyssynchrony[24].
- -
Step 6 - LVOT stroke distance (time-velocity integral): The stroke distance is obtained by tracing the systolic jet contour in the LVOT. Stroke volume is calculated by multiplying this distance by the LVOT area.
- -
Step 7 - Apical rocking - Apical rocking is often associated with septal flash. It is a well-recognized sign of left intraventricular dyssynchrony, especially in patients with advanced left bundle branch block or right ventricular pacing [25], and is best assessed in the Ap4C view. In the PREDICT-CRT study, apical rocking and septal flash added predictive power, beyond clinical variables and QRS duration, for identifying responders to cardiac resynchronization therapy. The absence of apical rocking, or failed reversal, have been linked to poor survival outcomes [26].
- -
Step 8 - Cardiac cycle duration: This is measured as the R-R interval using the time caliper and recorded in ms.
- -
Step 9 - Diastolic flow duration: This is measured to confirm or exclude atrioventricular (AV) dyssynchrony. In the apical view, using pulsed Doppler, mitral inflow is traced from the onset of the E wave to mitral valve closure, regardless of A wave presence.
- -
Step 10 - Diastolic flow / R-R ratio: The diastolic flow duration (in ms) is divided by the R-R interval, yielding a value < 1, and multiplied by 100 to obtain a percentage. A normal value is > 40%; any percentage below this threshold confirms AV dyssynchrony[27].
The entire image acquisition process is graphically depicted in Figure 1.
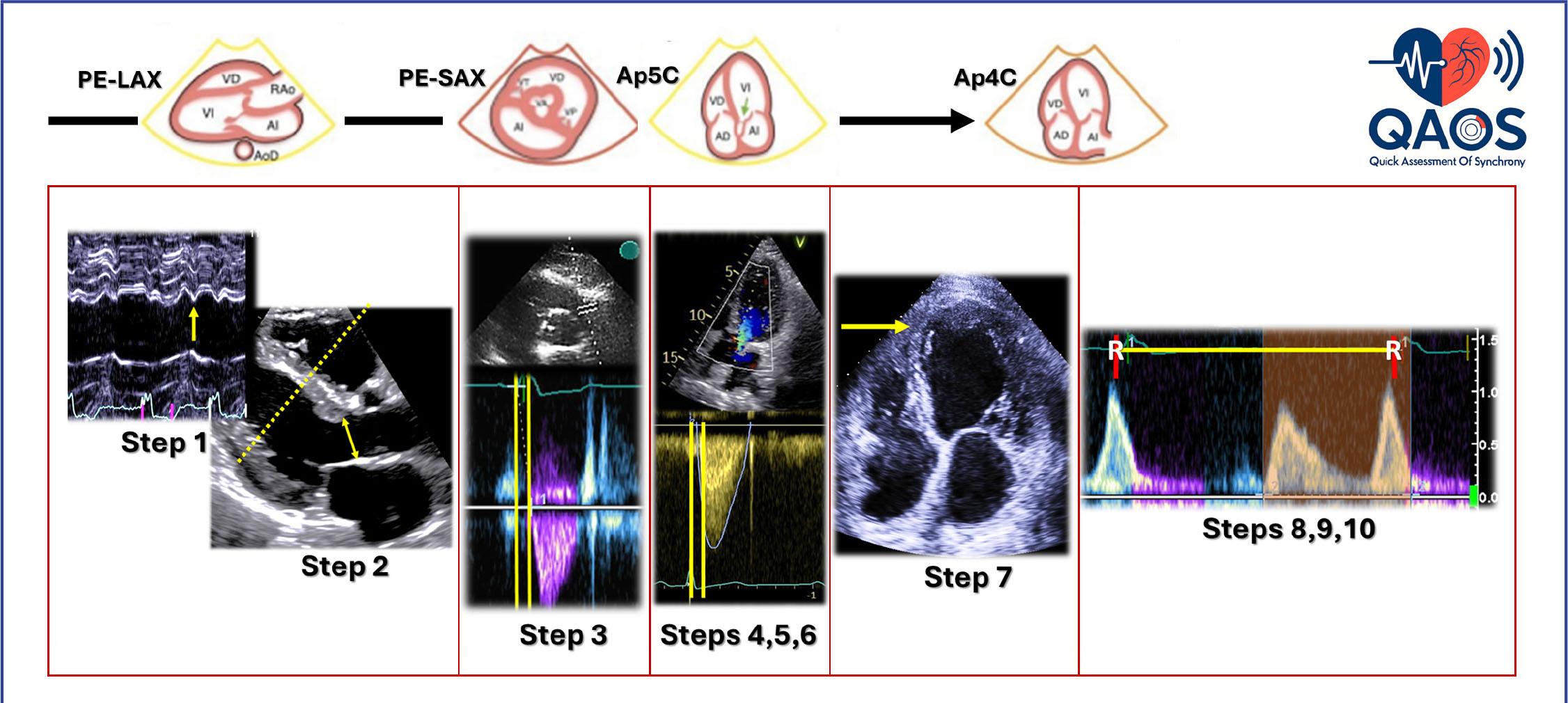
The image acquisition process adheres to the conventional sequence of standard echocardiography. The QAOS steps are illustrated in the parasternal long-axis (PE-LAX); short-axis views (PE-SAX, at the level of the great vessels); and apical five-(Ap5C) and four-chamber (Ap4C) views.
Once all data are collected, they are entered into a specific instrument (see Table 1), providing specific answers to the following questions — both in native rhythm and under artificial pacing, if necessary:
- -
Is there interventricular dyssynchrony?
- -
Is there left intraventricular dyssynchrony?
- -
Is there AV dyssynchrony?
- -
Can PIC be diagnosed?
- -
Are there criteria for pacemaker upgrade to cardiac resynchronization therapy or physiological pacing?
To provide practical examples of the implementation of QAOS protocol, Table 1 presents a side-by-side comparison between two clinical cases of symptomatic patients with pacemakers.
In Case A, the patient presents with ischemic structural heart disease and non-transmural scarring following a myocardial infarction. Eventually the patient developed a complete A-V block and a unicameral pacemaker was implanted. To date, the patient’s left ventricular ejection fraction (LVEF) is normal. The patient is in NYHA Functional Class II, with high-demand ventricular pacing and a markedly deleterious effect on synchrony and myocardial strain, but no effect in LVEF — which is why a pacing upgrade is not currently indicated.
In Case B, the patient presents without structural ventricular damage but remains symptomatic. Pacing-induced dyssynchrony develops, with a device dependency of 55%, accompanied by a 10% reduction in LVEF. In this context, PIC can be diagnosed, and an upgrade to physiological pacing is recommended.
In our ECHO Lab, after MAPSE and LVEF measurement, execution times for the ten protocol steps were timed; after 24 procedures, their average duration was four minutes and six seconds ± 22 seconds.
The ventricular activation front generated by a pacemaker resembles that of advanced left bundle branch block (as seen on surface electrocardiograms; see Figure 2), with delayed electromechanical activation of the left ventricular free wall.
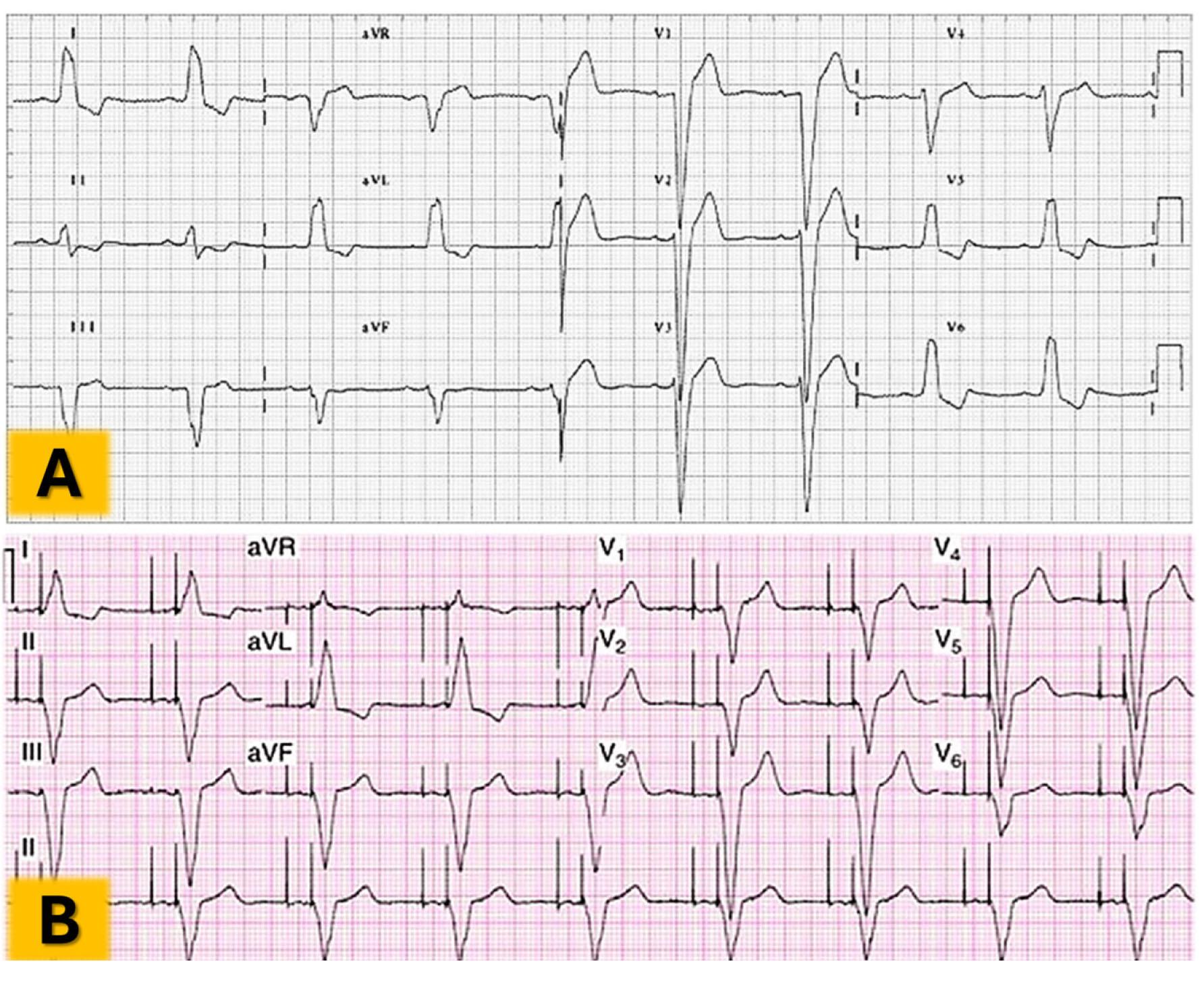
Comparison of the electrocardiogram from a patient with left bundle branch block (Panel A) and the tracing from a patient with a pacemaker showing right apical stimulation (Panel B).
This dyssynchronous contraction ultimately leads to heart failure[2] through various mechanisms — even in dual-chamber pacing modes [3]. Advanced imaging techniques, such as speckle-tracking echocardiography, have been useful in depicting the extent of such dyssynchrony (see Figures 3 and 4), but these applications demand expensive equipment that is not widely available, particularly in developing countries.
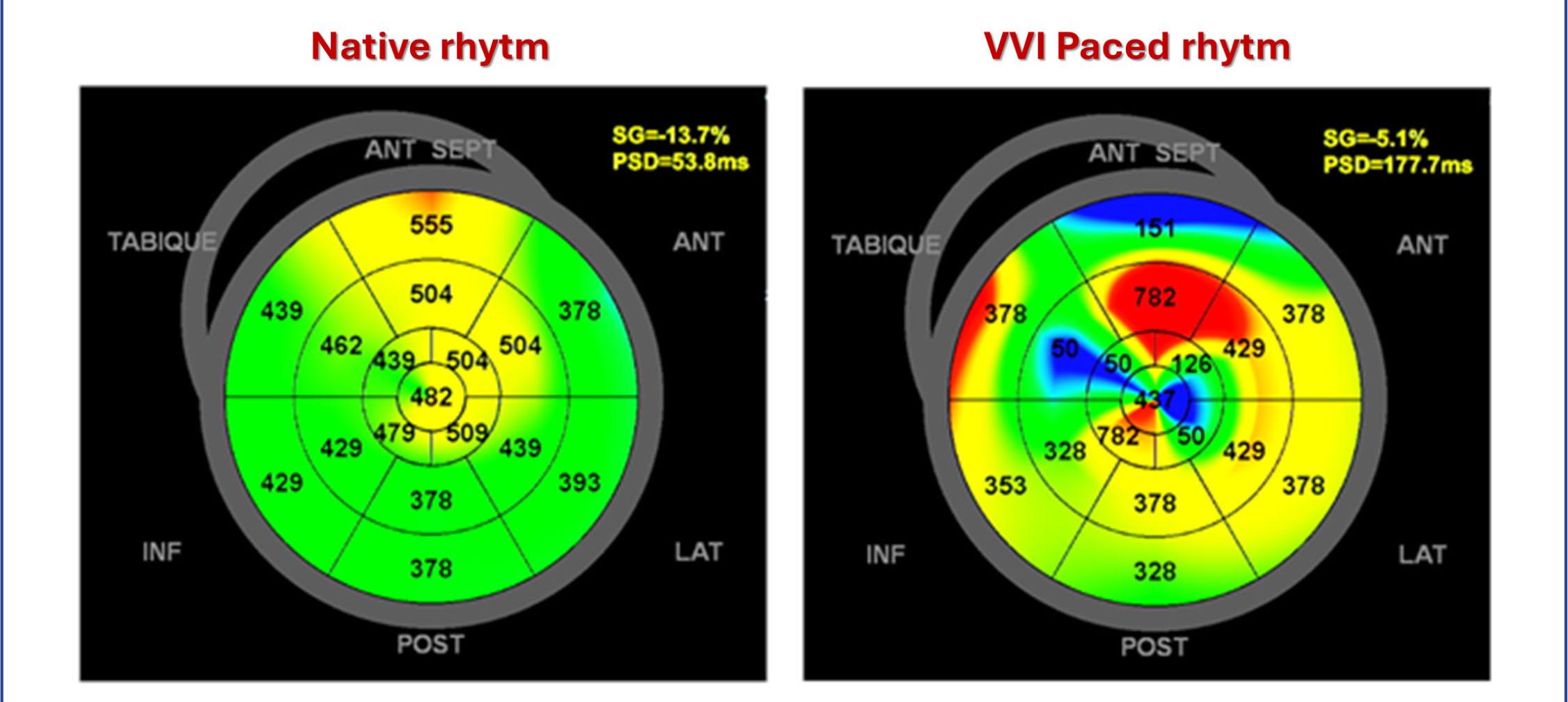
Polar maps of the left ventricle with pacemaker-induced left intraventricular dyssynchrony. Acute changes are shown in a female patient studied with speckle-tracking strain echocardiography, both in native rhythm (left) and during pacing from a right ventricular apical lead (right). Left ventricular mechanical dispersion (peak strain deviation, or PSD) increased from 53 ms (normal) to 177.7 ms (severely abnormal), confirming new dyssynchrony caused by pacing.
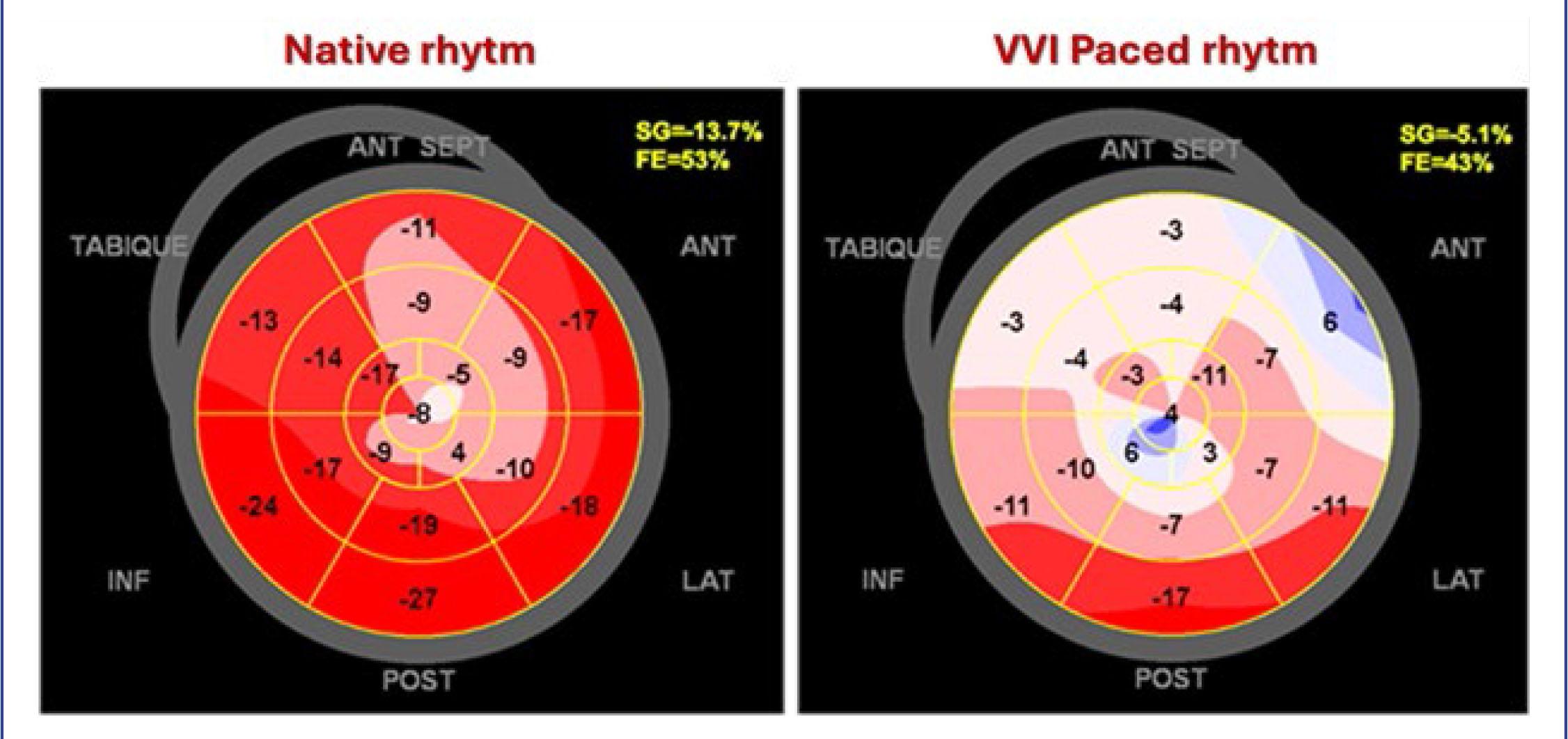
Polar maps of the left ventricle with pacemaker-induced ventricular dysfunction. Acute changes are shown in the same patient from Figure 3, assessed with speckle-tracking strain echocardiography. Left ventricular function in native rhythm (left) and during pacing from a right ventricular apical lead (right) are compared. Left ventricular ejection fraction (EF) decreases from 53% to 43%, and global longitudinal strain (SG) drops dramatically, from -13.7% to -5.1%.
The following tools are recommended for risk estimation, prevention, and detection of early, subclinical, or latent forms of dyssynchrony and / or PIC, both before and after device implantation:
- -
Serial electrocardiographic analysis (QRS morphology and duration).
- -
Monitoring of electrical parameters, such as left ventricular activation time.
- -
Active surveillance in patients with high pacing burden (> 20%), even with left bundle branch pacing,
- -
Imaging-based strategies to assess ventricular function and mechanical synchrony or dyssynchrony
With respect to imaging strategies, in patients with permanent pacemakers, echocardiography is indicated based on specific clinical criteria. QAOS protocol (outside of a complete echocardiographic study) could be implemented in the follow-up if a high burden of ventricular pacing (> 40%) is associated with an increased risk of PIC, which would justify echocardiographic evaluations every 6 to 12 months. Likewise, the emergence of new or progressive symptoms of heart failure constitutes an immediate indication for echocardiographic assessment. In patients undergoing cardiac resynchronization therapy (CRT) and conduction system pacing, echocardiography is also recommended three to six months after implantation to assess clinical response [27]. QAOS can be a useful tool in these instances because all the measurements and calculations have already been validated.
In conclusion, there are clinical scenarios in which the QAOS protocol may have practical application:
In patients with right ventricular pacing, QAOS may be used to detect pacing-induced dyssynchrony and / or ventricular dysfunction. These should both raise concern, given the natural history of such dyssynchrony often progresses toward heart failure [12], driven by a well-recognized cascade of functional deterioration. Periodic QAOS evaluations are thus needed in dyssynchronous patients to identify the optimal timing for cardiac resynchronization therapy or conduction system pacing beyond optimal medical management. The simplicity of this protocol allows for rapid assessment in both paced and native rhythm (when feasible), with a recommended interval of one to two minutes between evaluations.
QAOS may be a valuable tool — alongside clinical assessment — for verifying the effectiveness of cardiac resynchronization therapy or conduction system pacing, confirming whether the patient is a responder with improvement in symptoms and markers of synchrony and systolic function.
This protocol has been published to authorize its free use in both routine clinical practice and research settings. Users are encouraged to adhere faithfully to the protocol while remaining open to suggestions that may enhance its design. The development of a digital application for use on electronic devices is envisioned as a next step, should field results prove promising.