
Arterial hypertension (HTN) is the most common modifiable preventable risk factor for cardiovascular, cerebrovascular, and renal disease and their associated morbidity and mortality rates worldwide. [1,2,3,4,5,6] According to recently published guidelines, the treatment and control of arterial HTN are mainly based on office blood pressure measurement (OBPM), requiring confirmation on at least one additional subsequent office visit, or out-of-office evaluation.[6,7] Therefore, OBPM remains an essential tool for BP evaluation, either for treatment recommendations or research purposes.[2,8] However, the recommended OBPM procedures in these guidelines differ widely.[9,10,11]
The proper technique for measuring BP detailed in International Guidelines for Arterial Hypertension is to record at least three BP measurements, discarding the first measurement and averaging the last two readings.[12] The latest European Society of Cardiology guidelines for the management of arterial hypertension, and the 2020 International Society of Hypertension Global Hypertension Practice Guidelines define the diagnosis of arterial hypertension based on the mean of the second and third readings after five minutes of rest, with additional blood pressure measurement if the first two measurements vary by more than 10 mmHg, known as the gold standard of BP evaluation in Europe.[13,14] However, multiple studies have not applied these recommendations, and instead of discarding the first reading and taking the mean of the last two measurements, they calculated the mean of the three readings without discarding the first one.[15,16,17]
This non-adhesion to recommended guidelines of OBPM procedures has led to widespread criticism regarding its reproducibility in clinical practice and its potential repercussions on the management of arterial hypertension.[18] Given that evidence-based medicine recommendations are founded based on these studies, it is essential to acknowledge that different BP measurement procedures can lead to different BP values and, consequently, different arterial HTN classifications.[8]
In this regard, the aim of the present study was to compare three BP measurement procedures, namely single reading without rest (P-5), first single reading after 5 minutes of rest (P1) and the mean of all three readings at rest (P123), each of the three above to the mean of the last two readings (P23).
During May 2024, volunteer adults (≥18 years) were recruited via a blood pressure screening campaign in the context of the international initiative of May Measurement Month in Morocco.
Screenings occurred at various locations: down town, park and gardens. This campaign has also determined the prevalence of arterial HTN in Morocco.[19]
The study protocol was approved by the Research Ethics Committee of the University Hospital of Tangier (AC68FV/2024).
All blood pressure readings were performed in a seated position. The first blood pressure reading was recorded without rest, and then, after five minutes of rest, three consecutive blood pressure readings were recorded at one-minute intervals. All BP measurements were recorded in a seated position with back and arm supported and legs uncrossed, using an adequate upper arm cuff of a validated automated blood pressure monitor OMRON HEM9200T (Omron Healthcare, Kyoto, Japan).[20,21]
In total, four BP readings from each participant were used (one reading without five minutes of rest and three consecutive BP readings with one-minute intervals) to calculate systolic and diastolic BP values:
- -
First method (P-5): the first reading without five minutes of rest.
- -
Second method (P1): the first reading after five minutes of rest.
- -
Third method (P123): the mean of the three BP readings after five minutes of rest.
- -
Fourth method (P23): the mean of the last two readings after five minutes of rest.
For analysis, the fourth method (P23) was considered as the gold standard (GS) for arterial hypertension diagnosis. The first comparison consists of comparing (P-5) with the GS, the second comparison consists of comparing (P1) with the GS, and the third comparison consists of comparing (P123) with the GS.
All calculated BP values were classified as non-hypertensive/hypertensive for participants without a previous diagnosis of hypertension based on the up-to-date European Society of Cardiology guidelines for arterial hypertension.[14] When exploring the repercussions of different BP values on the diagnosis of HTN, the study population was stratified into two categories: patients with a previous diagnosis of HTN, and subjects without a previous diagnosis of arterial HTN. For a clear interpretation each category was classified into a dichotomous group: controlled/uncontrolled hypertensive and non-hypertensive/hypertensive. Therefore, individuals without a previous diagnosis of hypertension with a systolic BP≥140 mmHg or diastolic BP≥90 mmHg were classified as hypertensive. Participants with an established diagnosis of arterial hypertension were classified as controlled hypertensive if their systolic BP<140 mmHg and diastolic BP<90 mmHg, and uncontrolled hypertensive if their systolic BP≥140 mmHg or diastolic BP≥90 mmHg.
The data were collected and transposed on an Excel spreadsheet and then analyzed using the Statistical Package for Social Sciences SPSS software version 26.0. The description of study variables was carried out using measures of central tendency and dispersion; continuous data were reported as mean ± standard deviation (SD), and categorical variables were described as effective and percentage N (%). A t-test for paired data was used to compare BP values obtained with the three methods. The effect size of the difference of the means of BP values was assessed using Cohen’s D (classifying the effect size as a small, medium, and large effect for D 0.20–0.49, D 0.50–0.79, and D≥0.80 respectively). McNemar’s test on paired proportions and Cohen’s Kappa coefficient were used to evaluate the level of agreement between the different BP methods when classifying subjects as non-hypertensive/hypertensive for participants without previous diagnosis of hypertension, and as controlled/uncontrolled hypertension for patients with established diagnosis of hypertension.
A total of 1,421 subjects participated in our study. The mean age of the study participants was 47.98 ± 16.09 years, of whom 51.2% were women. Moreover, 247 participants had previous diagnoses of hypertension, accounting for 17.4% of the study population. The main characteristics of the analyzed sample are summarized in Table 1.
Differences in systolic blood pressure values using three methods.
| Methods of measurements | Mean systolic BP of alternative measurement method Mean ± SD | Mean systolic BP of the mean of the last 2 readings (GS) Mean ± SD | Difference in systolic BP between both methods Mean ± SD | p value | Cohen’s D |
|---|---|---|---|---|---|
| P-5 vs GSa | 130.63±20.27 | 125.94±18.76 | 4.68±9.26 | <0.001* | 0.239 |
| P1 vs GSb | 128.19±19.92 | 125.94±18.76 | 2.25±7.90 | <0.001* | 0.116 |
| P123 vs GSc | 126.69±18.79 | 125.94±18.76 | 0.75±2.63 | <0.001* | 0.039 |
BP, Blood Pressure; SD, Standard Deviation,
First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS)
Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS)
Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
The comparison between systolic blood pressures of each of the first three measurement modalities and the systolic BP of the GS showed a statically significant difference (p<0.001) (Table 1). The comparison between the diastolic blood pressures of each of the first two measurements modalities (P-5 and P1) and the diastolic BP of the GS has also shown a statistically significant difference. However, there was no statistically significant difference between the diastolic BP of the mean of the three readings (P123) and the mean of the second and third readings (Table 2). Figure 1 represents Bland-Altman plots comparing the mean difference between systolic and diastolic BP of all study participants.
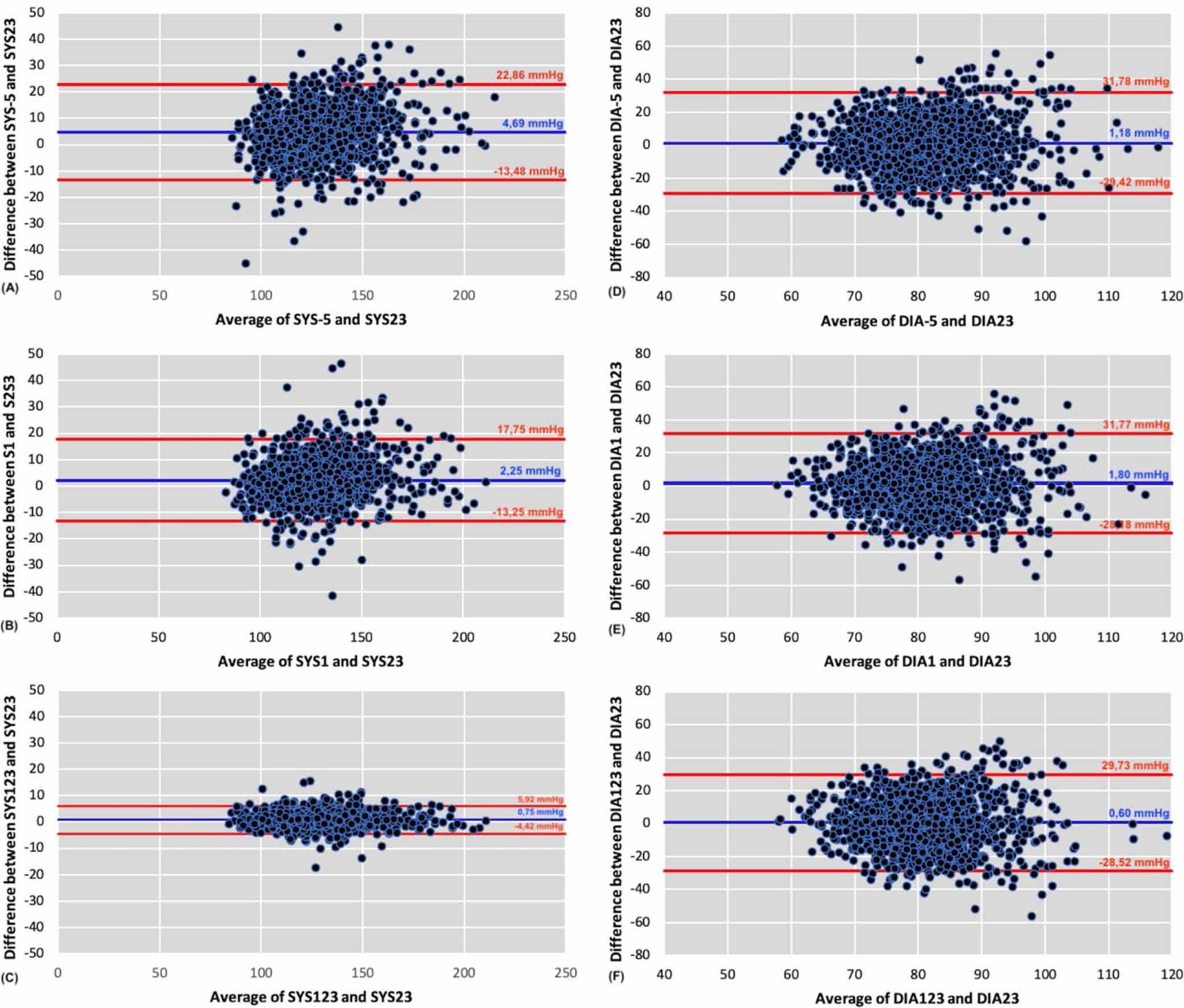
Bland-Altman plots comparing the difference between SYS-5, SYS1, SYS123 and SYS23 (panels A-B-C) and DIA-5, DIA1, DIA123 and DIA23 (panels D-E-F) of all participants of our study.
SYS, Systolic; DIA, Diastolic
Differences in diastolic blood pressure values using three methods.
| Methods of measurements | Mean diastolic BP of alternative measurement method Mean ± SD | Mean diastolic BP of the mean of the last 2 readings (GS) Mean ± SD | Difference in diastolic BP between both methods Mean ± SD | p value | Cohen’s D |
|---|---|---|---|---|---|
| P-5 vs GSa | 81.67±11.68 | 80.48±10.90 | 1.22±9.71 | 0.004* | 0.104 |
| P1 vs GSb | 82.30±11.23 | 80.48±10.90 | 1.81±15.29 | <0.001* | 0.163 |
| P123 vs GSc | 81.08±10.59 | 80.48±10.90 | 0.60±14.85 | 0.126 | 0.056 |
BP, Blood Pressure; GS, Gold standard; SD, Standard Deviation; a: First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS); b: Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS); C: Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS)
Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS)
Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
The mean systolic BP with the first reading without five minutes rest was 130.63 ± 20.27 mmHg, versus 125.94 ± 18.76 mmHg with the GS (mean difference 4.68 ± 9.26; Cohen’s D=0.239; p<0.001). The mean diastolic BP was 81.67±11,68 versus 80.48 ± 10.9 mmHg (mean difference of 12.28 ± 9.71; Cohen’s D = 0.104; p=0.004).
The mean systolic BP with the first reading after five minutes rest was 128.19 ± 19.92 mmHg, versus 125.94 ± 18.76 mmHg with the mean of the GS (mean difference 2.25 ± 7.9; Cohen’s D=0.116; p<0.001). The mean diastolic BP was 82.30 ± 11.23 versus 80.48 ± 10.9 mmHg (mean difference 1.81 ± 15.29; Cohen’s D=0.163; p<0.001).
The mean systolic BP with the mean of P123 was 126.69 ± 18.79 mmHg, versus 125.94 ± 18.76 mmHg with the mean of the GS (mean difference 0.75 ± 2.63; Cohen’s D=0.039; p<0.001). Whereas, no statistically significant difference (p>0.05) was found between the mean difference (0.60 ± 14.85 mmHg) between diastolic BP of P123 and P23.
Diagnosis of arterial hypertension for patients without previous diagnosis of hypertension.
| Blood pressure measurement methods | Normal N (%) | Hypertension N (%) | p value | Kappa | |
|---|---|---|---|---|---|
| P-5 vs GSa | First reading without 5 min rest | 807 (68.7) | 367 (31.3) | < 0.001* | 0.333 |
| Mean of the 2nd and 3rd readings | 814 (69.3) | 360 (30.7) | |||
| P1 vs GSb | First reading after 5 min rest | 699 (59.5) | 475 (40.5) | < 0.001* | 0.270 |
| Mean of the 2nd and 3rd readings | 814 (69.3) | 360 (30.7) | |||
| P123 vs GSc | Mean of the 3 readings | 894 (76.1) | 280 (23.9) | < 0.001* | 0.436 |
| Mean of the 2nd and 3rd readings | 814 (69.3) | 360 (30.7) | |||
GS, Gold standard; a: First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS); b: Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS); C: Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS)
Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS)
Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
Diagnosis of arterial hypertension for patients with previous diagnosis of hypertension.
| Blood pressure measurement methods | Controlled HTN N (%) | Uncontrolled HTN N (%) | p value | Kappa | |
|---|---|---|---|---|---|
| P-5 vs GSa | First reading without 5 min rest | 82 (33.2) | 165 (66.8) | < 0.001* | 0.456 |
| Mean of the 2nd and 3rd readings | 106 (42.9) | 141 (57.1) | |||
| P1 vs GSb | First reading after 5 min rest | 99 (39.7) | 148 (60.3) | < 0.001* | 0.500 |
| Mean of the 2nd and 3rd readings | 106 (42.9) | 141 (57.1) | |||
| P123 vs GSc | Mean of the 3 readings | 118 (47.8) | 129 (52.2) | < 0.001* | 0.756 |
| Mean of the 2nd and 3rd readings | 106 (42.9) | 141 (57.1) | |||
GS, Gold standard; HTN, hypertension; SD, Standard Deviation, a: First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS); b: Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS); C: Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
First method: First reading without 5 minutes of rest (P-5) versus the mean of the second and third readings (GS)
Second method: First reading after 5 minutes of rest (P1) versus the mean of the second and third readings (GS)
Third method: Mean of three readings after five minutes of rest (P123) the mean of the second and third readings (GS)
The agreement between the first reading without 5 min rest and the gold standard for classifying participants without an established diagnosis of hypertension as non-hypertensive/hypertensive
showed a Kappa value = 0.333 (McNemar’s test p<0.001). A percentage of 46.6% (171/367) of participants classified as nonhypertensive with the GS would have been considered hypertensive based on the first reading without 5 minutes of rest (P-5). On the contrary, 45.6% (164/360) of subjects classified as non-hypertensive based on the first reading without 5 minutes rest (P-5) are considered hypertensive with the GS.
The first reading after 5 min rest (P1) and the GS objectify a fair level of agreement (Kappa value = 0.270), a percentage of 53.9% (256/475) of participants considered non-hypertensive based on the gold standard would have been classified as hypertensive based on the first reading after 5 minutes of rest. On the contrary, 39.2% (141/360) of the participants classified as non-hypertensive based on the first reading after 5 minutes of rest (P1) are considered hypertensive with the GS.
Moreover, the level of agreement between the mean of P123 and the GS showed a Kappa value of 0.436. Only 32.9% (92/280) of participants classified as non-hypertensive based on the GS would have been considered hypertensive with the mean of the P123. On the contrary, 47.8% (172/360) of participants classified nonhypertensive with the mean of P123 are considered hypertensive with the GS (Table 3).
The level of agreement between the first reading without 5 min of rest (P-5) versus the GS for participants with previous diagnoses of HTN was 0.456 (McNemar’s test p<0.001). 26.7% (44/165) of the individuals classified as controlled hypertensive with the GS would have been classified as uncontrolled based on the first reading without 5 minutes of rest (P-5). On the other hand, 14.2% (20/141) of the individuals classified as controlled hypertensive based on the first reading without 5 minutes rest are considered uncontrolled with the GS. A Kappa value of the agreement between the first reading after 5 min of rest (P1) and the GS was 0.5. A percentage of 22.8% (34/149) of controlled hypertensives classified based on the GS are considered uncontrolled hypertensives based on the first reading after 5 minutes of rest (P1). On the other hand, 18.4% (26/141) of the individuals classified as controlled based on the first reading after 5 minutes rest (P1) would have been considered not controlled with the mean of P23, and the Kappa value of the agreement between the mean of P123 versus the GS was 0.756 (Table 4).
The diagnosis and control of arterial hypertension is based on office blood pressure measurement. Adopting a technically correct BP measurement is mandatory to minimize errors and discrepancies resulting from different BP measurement procedures. This issue would eventually impair hypertension management, either for its first diagnosis for patients without a previous diagnosis of hypertension, or for therapeutic purposes for patients with an established diagnosis of hypertension.
There is significant alignment on the fact that the more BP readings performed, the more precise the BP values obtained and less white coat effects occur.[8,22,23,24] The International Society of Hypertension and the European Society of Cardiology guidelines suggest taking three BP measurements and discarding the first BP reading.[13,8] On the other hand, Korean and Chinese guidelines require discarding the first reading only if BP values obtained differ by more than 10 mmHg compared to the first reading.[25,26] Japanese and South African recommendations suggest discarding the first reading if the BP of the two readings differs by just 5 mmHg or more. [27,28] In contrast, the Canadian guidelines require discarding the first reading only while using manual devices and suggest keeping the first BP if an automated device is used, while the 2025 American Heart Association and American College of Cardiology (AHA / ACC) guideline for the prevention, detection, evaluation and management of High Blood Pressure in Adults recommends averaging at least two consecutive BP readings at rest, without specifying discarding anyone of them or not. [29,30]
Our finding shows a statically significance difference between systolic blood pressure (SBP) values obtained with each procedure and the GS (p<0.001). A small effect size of the mean difference of SBP values was found in the three comparisons.
These findings support the fact that this divergence in BP evaluation procedures demonstrated in our study by the three comparisons can ultimately lead to different BP results, either in systolic or diastolic BP values, and consequently lead to improper diagnoses and treatment of arterial HTN including overdiagnosis or underdiagnosis, and overtreatment or undertreatment of arterial HTN.
When classifying hypertensive patients as controlled or uncontrolled hypertensive, a good measure of reliability can be inferred from the high level of agreement found in our study between the mean of P123 versus the GS (kappa=0.756) (Table 3). These findings are consistent with those assessed by cardiovascular risk and cardiovascular events in the general population from the Health Area of Toledo study (RICARTO) (kappa=0.788); a study that assessed BP values obtained by averaging three BP readings (P123) and the mean of the second and third readings after discarding the first one (P23). On the other hand, a moderate level of agreement was found while comparing the first reading without five minutes of rest with the GS, and the first reading with five minutes of rest (Kappa=0.456 and Kappa=0.5 respectively)[18] In contrast, a discordance was found between our findings and the RICARTO study, when classifying participants without previous diagnosis of HTN as non-hypertensive/hypertensive. The three methods of measurements of our study showed a fair and moderate level of agreement compared to the GS. While a high level of agreement was found in the RICARTO study (kappa = 0.847).[18] In the same context, Alireza et al. compared the difference between the first BP reading (P1), the second (P2), the mean of the first and second readings (P12), and then, the mean of the three readings (P123) with the mean of the gold standard (P23). In alignment with our findings, Alizera et al showed statistically significant differences between various blood pressure values obtained by each BP measurement procedures and the GS, for both systolic and diastolic BP values.[31]
These results confirm the previously mentioned problem of improper diagnosis and control of arterial hypertension, that arise from different blood pressure values resulting from different blood pressure evaluation procedures. Supporting the fact, that different methods of BP evaluation do not only affect systolic BP and diastolic BP values, but also has significant impacts on both the diagnosis and management of arterial hypertension.
Therefore, searching for an optimal method for BP evaluation based on office blood pressure measurement remains a topical issue. This underscores the necessity of developing a standardized method of OBPM worldwide, enhancing the precision of the results obtained.
Due to the high variability of different BP measurement procedures, studies have been conducted to defend the usefulness of out-of-office BP assessments, namely home blood pressure measurement (HBPM), and 24-hour ambulatory blood pressure monitoring (24-hour ABPM) (based on more than 50 readings per 24 hours) in building an accurate diagnosis. Indeed recent recommendations require the need to adopt HBPM and 24-hour ABPM as a complementary method to validate the diagnosis of arterial HTN, to prevent white-coat effect and masked hypertension, enabling a proper diagnosis of arterial HTN and avoiding unnecessary or insufficient treatment. [32,33] However, despite this growing scientific interest, OBPM remains the standard in clinical practice because it occurs in standardized conditions, uses consistent and cost-effective methodology, and allows reliable comparison with established diagnostic BP thresholds and treatment guidelines.[34,35]
The main limitation of our study is that BP measurements were taken in an out-of-office setting. Nevertheless, this was addressed by performing the measurements in a calm and well-organized tent designed to stimulate office conditions. However, this was compensated for by the fact that all blood pressure measurements were taken by trained volunteers from the physiology department of the faculty of medicine to ensure standardized measurements across all the screening sites. On the other hand, the great strengths of our study include the large sample size of participants, representing a random sample of the Moroccan general population studied in this project.
In conclusion, standardized office blood pressure measurement remains the reference method for hypertension diagnosis and treatment, which is recommended by the International Guidelines for Arterial Hypertension. The difference in blood pressure values obtained with different blood pressure evaluation methods used in our study confirms the necessity of adopting a unique and validated method according to the International Recommendations for Arterial Hypertension.
Our study shows that any change in blood pressure measurement procedure can significantly influence both systolic and diastolic blood pressure values, thereby affecting their interpretation, and arterial hypertension diagnosis and control. These findings underscore the need to standardize blood pressure measurement procedures according to evidence-based medicine to ensure the accuracy of arterial HTN diagnosis.