
Transcatheter aortic valve replacement (TAVR) and endovascular aneurysm repair (EVAR) have emerged as attractive less invasive procedures in high surgical risk patients for symptomatic severe aortic stenosis and abdominal aortic aneurysm, respectively. TAVR can be performed using various approaches like transfemoral, transapical, trans-subclavian and transaortic. The transfemoral approach represents the preferred and less invasive alternative, and it also allows the abdominal aortic aneurysm repair using the same access site during the same procedure. There are various challenges that need to be addressed with the sequential treatment strategy. According to the European guidelines [1], patients with symptomatic severe aortic valve stenosis are at increased risk of peri-operative cardiovascular complications during non-cardiac surgery, and aortic valve replacement should be performed before the elective procedure, but there are no clear recommendations, and several factors need to be taken into consideration. Therefore, we aimed to present two cases of high-risk patients with symptomatic severe AS and concomitant large AAAs successfully treated by combined TAVR and EVAR procedures.
A 78-year-old male was admitted to our cardiology department for worsening heart failure symptoms, fatigue, dyspnea at mild exertion (NYHA III functional class), angina and abdominal pain.
The patient had a history of coronary artery disease with a percutaneous coronary intervention (PCI) of the right coronary artery 10 years ago, hypertension, paroxysmal atrial fibrillation, carotid artery atherosclerosis, and an ischemic stroke. A few months ago, he was diagnosed with severe aortic stenosis. In the past few months, he has had multiple hospitalizations for worsening heart failure symptoms.
Physical examination revealed a hemodynamically stable patient, with a blood pressure of 100/70 mmHg, heart rate of 70 beats per minute, respiratory rate of 20 breaths per minute, and oxygen saturation of 97%. Heart sounds were regular, and a systolic aortic murmur grade 3/6 was detected. Lung auscultation revealed bilateral basal moist rales. Abdominal examination showed a pulsating mass.
Blood work was unremarkable. The electrocardiography (ECG) showed signs of left ventricular hypertrophy. Transthoracic echocardiogram (TTE) revealed left ventricular hypertrophy, a left ventricular ejection fraction of 57%, severe aortic stenosis with a mean gradient of 52 mmHg, peak systolic velocity 4.7 m/s, and an indexed aortic valve area of 0.4 cm2/m2.
Considering the abdominal pulsatile mass, a Duplex vascular abdominal ultrasound was performed, followed by a computed tomography angiography (CTA), which showed a saccular infrarenal abdominal aneurysm (AAA) measuring 76 x 86 mm (AP x LL) with parietal thrombosis, extending towards the aortic bifurcation.
As part of the periprocedural evaluation, a coronary angiography was performed, which revealed a significant stenosis of the proximal right coronary artery, adjacent to a previously implanted stent. This lesion was successfully treated with percutaneous coronary intervention (PCI) and stent implantation. The presence of a large, symptomatic abdominal aortic aneurysm (AAA) further complicated the patient’s management. But performing TAVR first can lead to a sudden increase in systemic blood pressure due to the removal of the aortic valve pressure gradient. This hemodynamic shift may impose additional stress on the AAA, potentially increasing the risk of rupture [2]. To mitigate this risk, the management strategy was to perform both TAVR and EVAR in a single procedural session, allowing for immediate exclusion of the aneurysm from circulation and avoiding the vulnerable post-TAVR period. Given the patient’s high-risk status, primarily due to severe symptomatic AS, and the favorable anatomy confirmed by preprocedural CTA, EVAR was deemed feasible and appropriately executed.
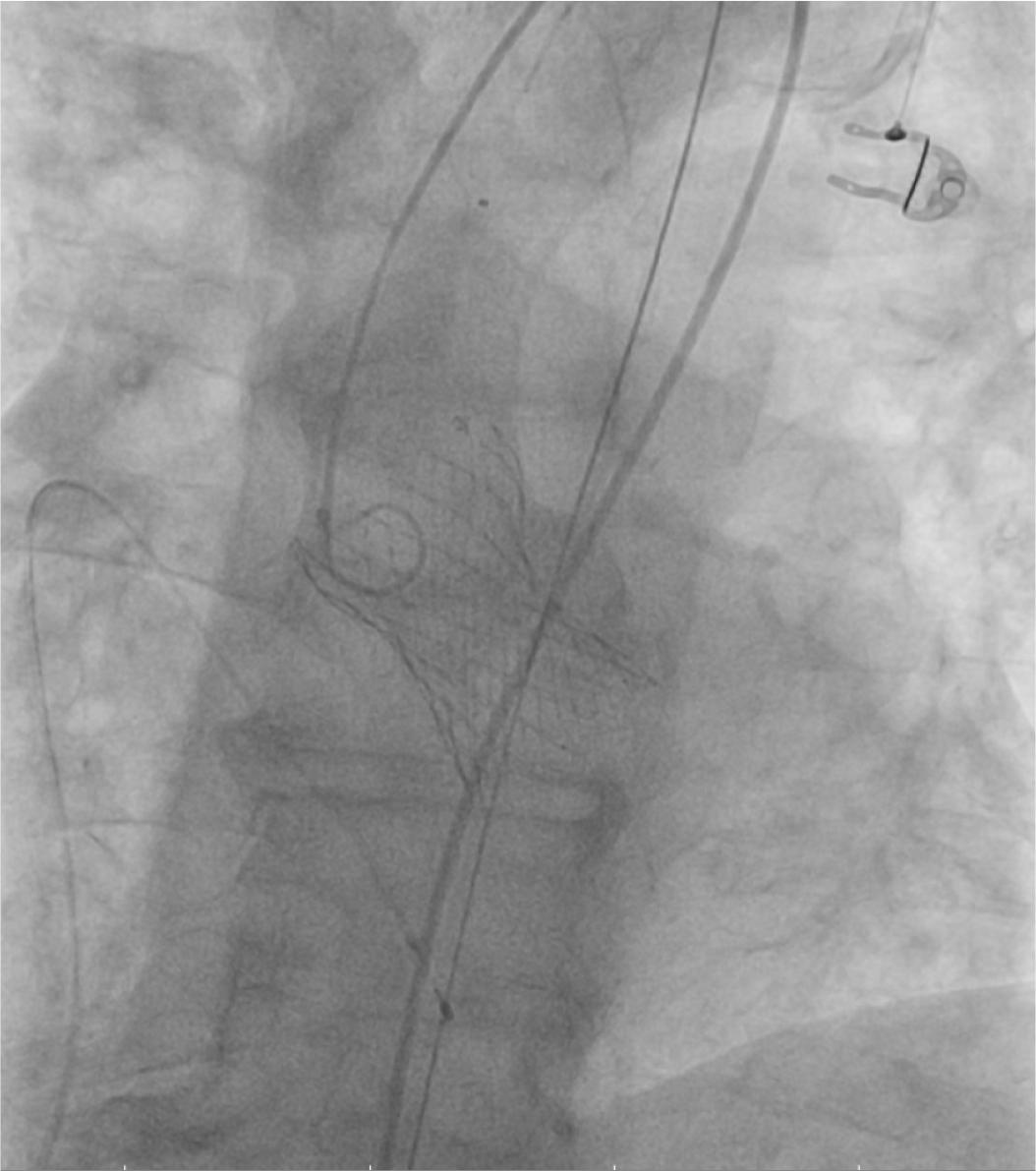
According to the European guidelines, aortic valve replacement should be considered before the the aortic aneurysmal repair. The patient was considered to be an intermediate risk candidate for surgical aortic valve replacement according to the EuroSCORE II (7%) and STS (8.2%) scoring systems, but given the association of patient’s frailty, advanced age (> 75 years), restricted mobility due to osteoporotic joint disease and the presence of a large abdominal aortic aneurysm, the Heart Team decided that the optimal treatment strategy for this patient is the transcatheter approach, TAVR followed by EVAR. The procedure was performed under spontaneous ventilation, with conscious sedation. A temporary pacing wire was inserted in the right ventricle, through the left common femoral vein to provide backup pacing in case of atrioventricular block development and rapid pacing for correct valve positioning. Bilateral percutaneous femoral access was obtained using the Seldinger technique, followed by pre-closure on both sides with two Proglide 6 Fr devices placed in a standard way. A 29 mm Medtronic Evolut R valve was inserted by an 18-French Sentrant Metronic sheath through the right femoral artery. After the direct deployment of the valve and balloon post-dilation under rapid pacing, the valve was correctly positioned and expanded (Figure 1), with a minor aortic insufficiency due to a paravalvular leak.

Fluoroscopic image: deployment of the Medtronic valve.
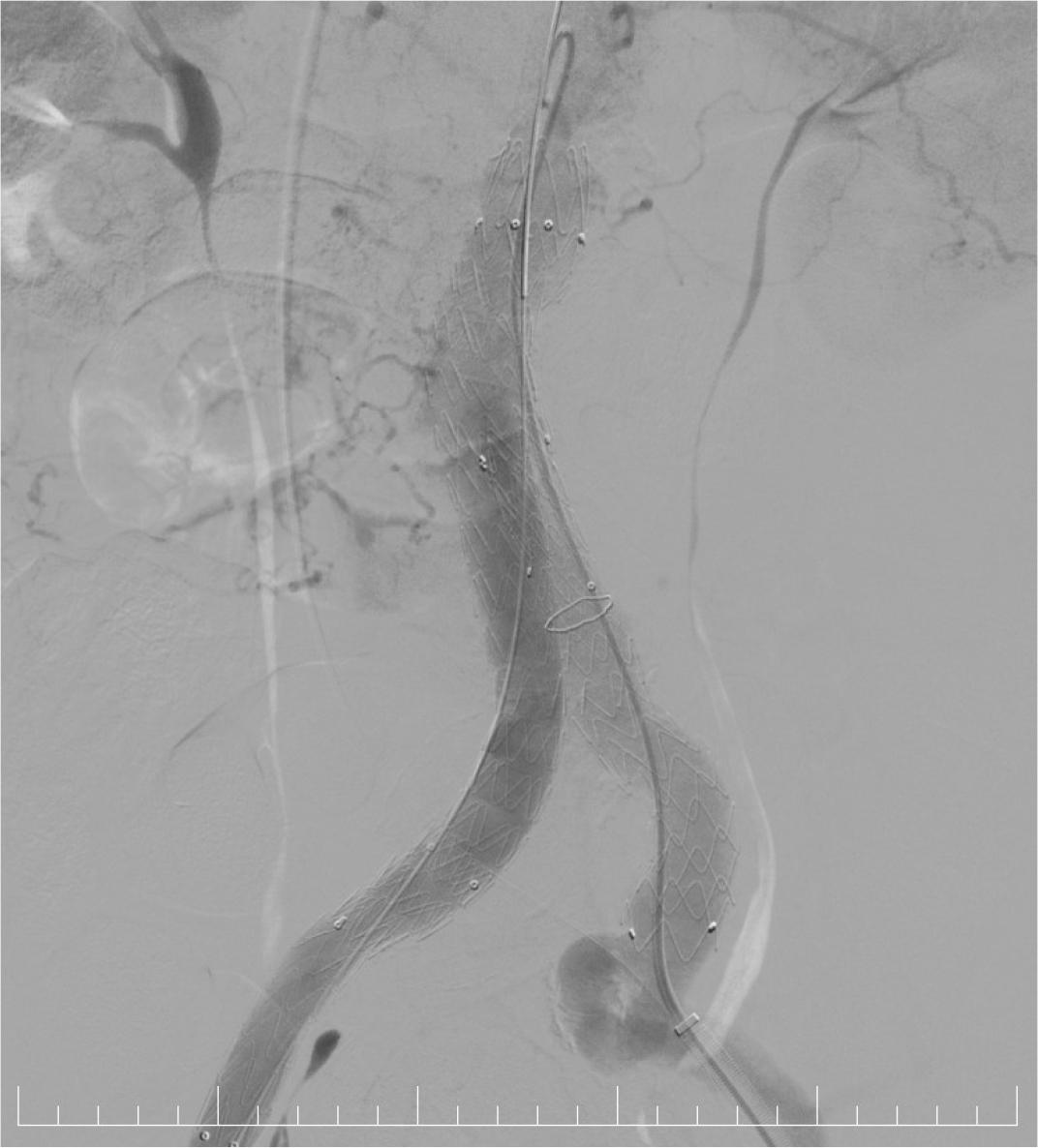
Using the same vascular access site, an Endurant II 25-13-166 mm endo-prosthesis was carefully deployed just distal to the right renal artery, extending through the right common iliac artery down to the iliac bifurcation. The device was precisely positioned to ensure an adequate proximal and distal sealing zone, considering the length and diameter of the infrarenal neck and iliac vessels. From the contralateral femoral access, a 14-French Sentrant Medtronic sheath was introduced, through which an additional contralateral extension with an Endurant II 16-13-124 mm endoprosthesis was advanced and deployed, covering the terminal abdominal aorta and extending into the left common iliac artery. The use of a large-bore sheath facilitated smooth delivery and deployment of the devices. Post-deployment balloon angioplasty was performed to optimize endoprosthesis apposition and expansion, reducing the risk of endoleaks and ensuring secure fixation. Completion angiography demonstrated correct positioning with full expansion of the stent graft components, achieving complete exclusion of the aneurysmal sac. A minimal type II endoleak was observed, originating from lumbar artery collaterals, which was hemodynamically insignificant and expected to resolve spontaneously.
The right common femoral artery was closed with two Proglide 6F devices, completed with one Angioseal 8F. Through the contralateral sheath, the completion angiography of the right puncture site showed an efficient closure of the artery. The hemostasis of the left common femoral artery was achieved using the two previously deployed Proglide devices, with no need for additional angiography.

Fluoroscopy: deployment of the aortic endograft.
The TTE, performed after the procedure, revealed a mean transprothetic gradient of 13 mmHG, a minor paraprothetic leak with an approximate circumferential extent of 10% (Figure 3).
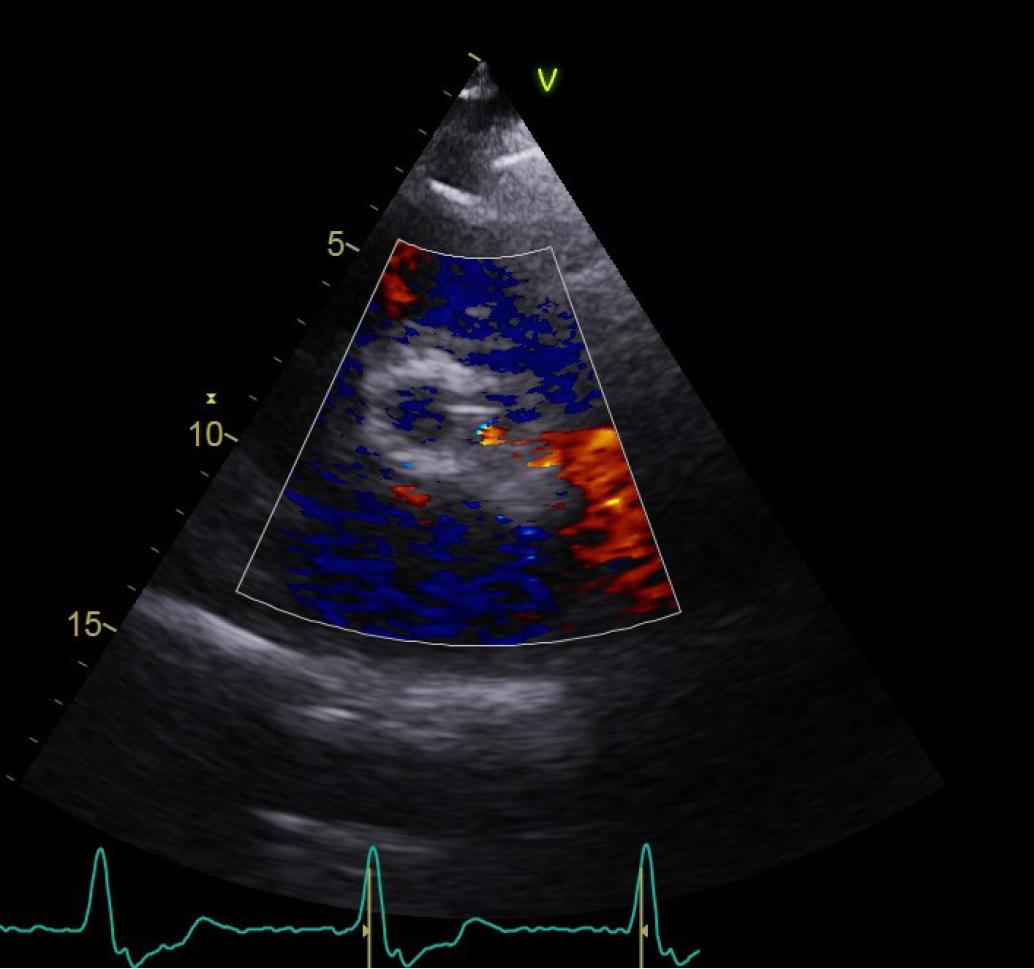
Transthoracic echocardiogram, parasternal short axis view of the paravalvular leak.
For a complete evaluation of the aneurysm, we performed a CTA of the aorta a few days after the procedure, that showed a type II endoleak, without evidence of aneurysm enlargement (Figure 4).
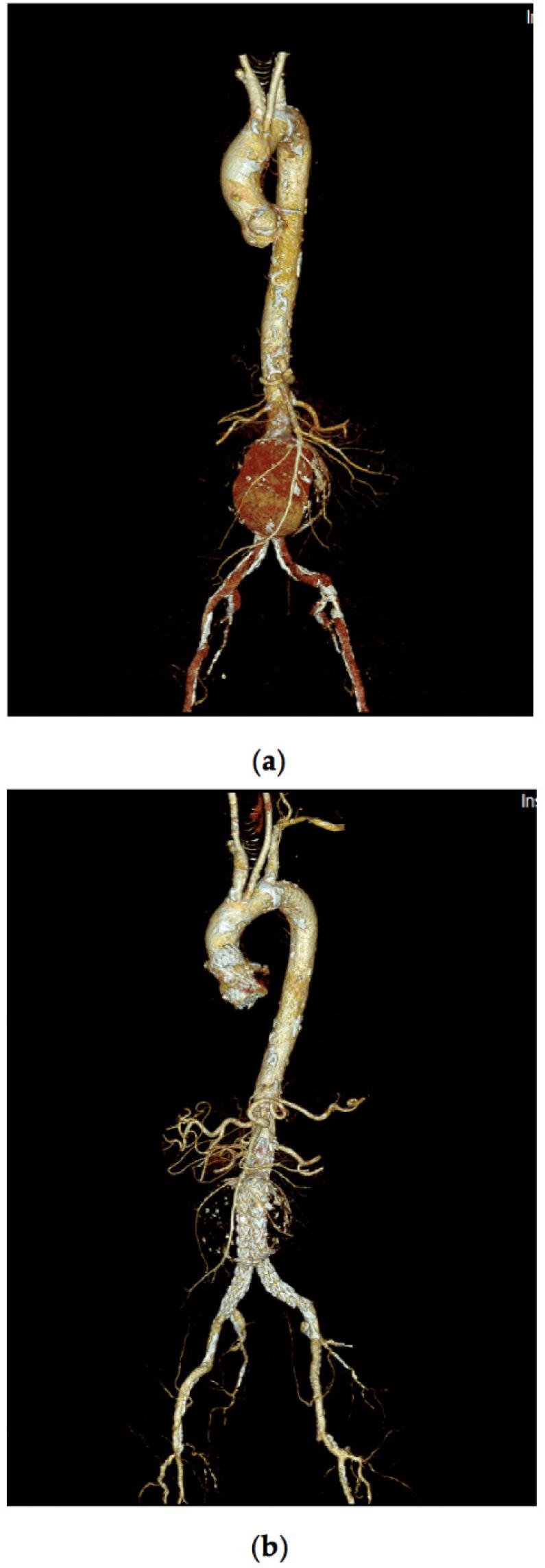
Computed Tomography Angiography – 3D reconstruction of the aorta (a) before, and (b) after aortic endo-graft implant.
The patient was discharged at day 7 after the procedure. The first follow-up visit was established at one month after the procedure and afterwards every 6 months depending on the evolution. At the 6-month follow-up visit, we noticed an improvement in the clinical status and the patient reported an alleviation of symptoms. The aortic bioprosthesis (TAVR) was normofunctional and the CTA showed an almost complete thrombosis of the aneurysm with stable dimensions of the aneurysmal sac despite the persistence of the type II endoleak due to lumbar collaterals (Figure 5). Unfortunately, after the 6-month evaluation, the patient was lost to follow-up, and no further medical evaluations could have been performed.
Computed Tomography Angiography at 6 months follow-up.
A 74-year-old male was admitted to our emergency department with the diagnosis of acute heart failure and severe aortic stenosis.
Physical examination revealed a hemodynamically stable patient, with a blood pressure of 100/60 mmHg, heart rate of 100 bpm, oxygen saturation of 90%, respiratory frequency of 30 rpm. Heart sounds were regular, and a systolic aortic murmur grade 4/6 was detected. Lung auscultation revealed bilateral moist rales.
Blood work showed elevated NT-proBNP (3560 pg/ml), moderate hyponatremia (128 mmol/l), and hyperglycemia (230 mg/dl), ECG showed atrial fibrillation and right bundle branch block.
The TTE revealed a dilated left ventricle, with a severely reduced left ventricular ejection fraction of 25%, and a low-flow low-gradient severe aortic stenosis with a transaortic mean gradient of 30 mmHg, peak systolic velocity of 3 m/s, and an aortic valve area of 0.9 cm2.
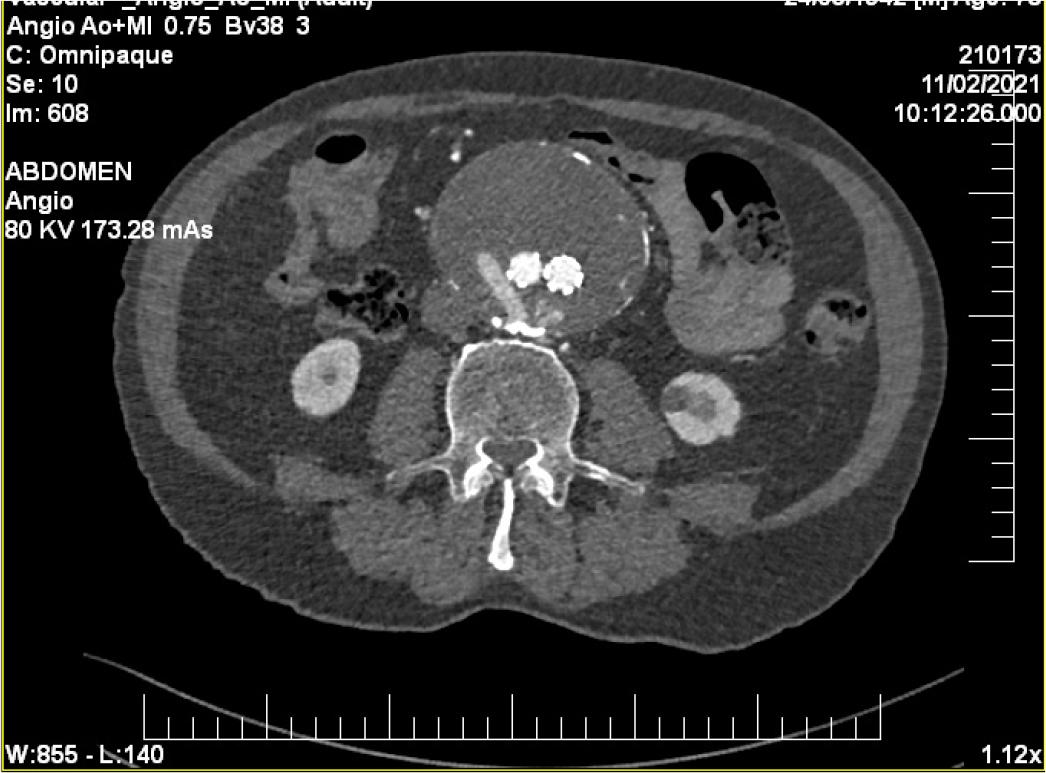
Given the patient’s high surgical risk, the Heart Team decided that TAVR was the most appropriate management strategy. As part of the pre-procedural workup, a computed tomography angiography (CTA) was performed, which revealed a 55/60 mm infrarenal AAA characterized by a long infrarenal neck with mural thrombus and limited calcification. Additionally, the CTA identified a 4 cm aneurysm involving the right common iliac artery (RCIA), with parietal thrombosis, significant calcifications, and a residual lumen measuring 18 mm (Figure 6).
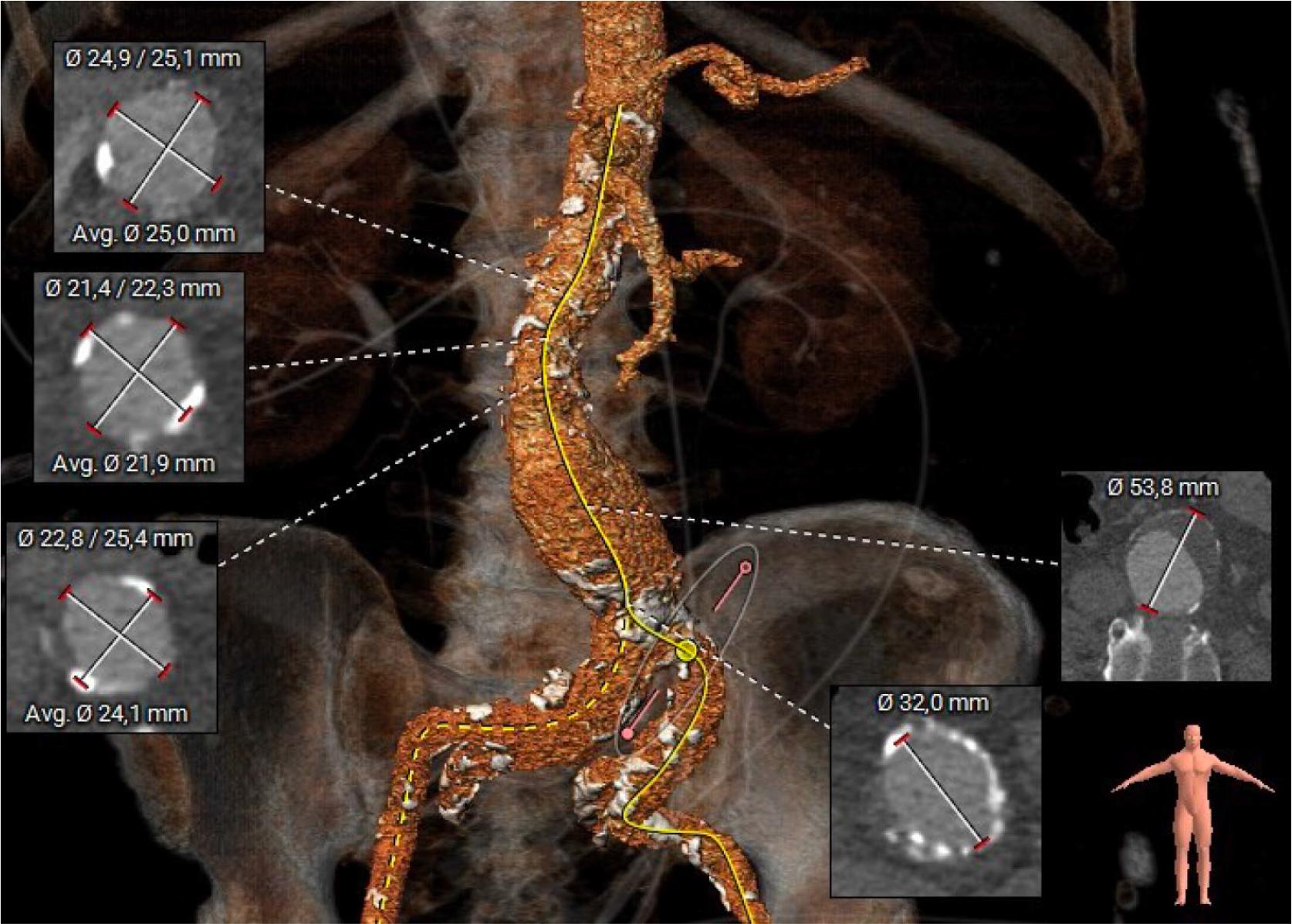
Computed Tomography Angiography showing the AAA and the RCIA aneurysm. An accessory right renal artery is also described.
Because of the high surgical risk profile of the patient, the transcatheter approach, TAVR followed by EVAR for both AAA and RCIA aneurysm during the same procedure was decided by the Heart Team. Initially, the intervention was performed under spontaneous ventilation, with conscious sedation. A self-expanding percutaneous transcatheter FX-34 mm Medtronic Evolut aortic valve was inserted through right femoral artery initially under conscious sedation, later the procedure required general anesthesia with endotracheal intubation and mechanical ventilation. A temporary pacemaker electrode with balloon was placed in the apex of the right ventricle through the left common femoral vein with effective temporary pacing at 4V. Using the left common femoral arterial access, a 6F pigtail catheter was placed in the non-coronary aortic sinus. The pre-closure of the right common femoral arterial access was performed with two Proglide 6F devices, followed by sheath exchange to 10F and finally to Sentrant 18F. A 0.035” x 300cm Confida guidewire was placed in the left ventricle using a 6F AL1 catheter, after crossing the aortic valve with a 0.035” straight wire. IV heparin was administered under strict ACT control. Partial implantation of a 34mm Medtronic Evolut FX aortic valve prosthesis under rapid pacing at 120 bpm using a standard height positioning related to the aortic annulus was performed, but unfortunately with a significant under-expansion of the aortic prothesis and secondary hemodynamic collapse of the patient. Hence, a rapid valve removal was necessary, followed by the pre-dilatation of the stenotic native valve with a 24/40 NC balloon under temporary pacing at 180 bpm. Afterwards, the aortic prothesis was implanted with a slight protrusion into LVOT, and secondary eccentric leak between the coronary sinus and non-coronary sinus (Figure 7). A post-dilation with 26/40 balloon under pacing at 200 bpm, then with a 28/40 balloon was performed. The angiographic result was good, the valve was properly positioned and expanded, and the coronary ostia was unobstructed.
Fluoroscopic image: deployment of the pre-dilated Medtronic valve.
Afterwards, the procedure continued with the percutaneous implantation of an Endurant II 32-16-166 mm endograft from the origin of the right renal artery to the terminal abdominal aorta using a 18F Sentrant sheath. Completion with a left iliac extension was performed using an Endurant II 16-13-124 mm endograft from the terminal aorta to the proximal left ex-ternal iliac artery (EIA) – Figure 8.
Fluoroscopic image: EVAR successfully performed.
The graft was properly positioned and expanded with complete aneurysm exclusion and no visible leak. The right distal radial artery (5F sheath) was left in place for invasive blood pressure monitoring. Because the proper hemostasis was impossible to achieve at the femoral vascular access site, surgical hemostasis was necessary.
Also, a pacemaker was implanted 48 hours after the procedure due to complete atrio ventricular block.
Due to clinical signs of acute right lower limb ischemia, a peripheral angiography was performed, and severe delayed flow was observed at common femoral artery (CFA), superficial femoral artery (SFA), and popliteal artery level. Also, the popliteal artery presented an aneurysmal dilation with mural thrombus and the anterior tibial artery was occluded immediately after origin and the posterior tibial artery (PTA) was occluded distally, likely due to popliteal aneurysm emboli. So, percutaneous balloon angioplasty of the distal PTA was performed, using an Asahi Gladius 0.014” x 300 cm guidewire which was advanced into the distal PTA, crossing the occlusion up to the medial plantar artery. The full-length lesion was dilated with a SC Polux 3.0 x 150 mm balloon, with repeated inflations at 6–8 atm, 2x2 minutes each. The flow was finally restored through PTA and distally to interphalangeal arteries. The patient’s evolution was slowly favorable, with a superinfection of the femoral wound which required reintervention. The echocardiographic exam revealed a significantly improved left ventricle ejection fraction of 43%. Also, the NT-proBNP value was significantly lower (1670 pg/l). The patient was discharged after 40 days of hospitalization. At 3-month follow-up, the patient had a good clinical status and reported improvement in symptoms and quality of life.
Degenerative aortic stenosis has a major epidemiological impact as life expectancy increases. Since 2002, when Alain Cribier performed the first implantation of a transcatheter aortic valve in a patient with severe, in-operable aortic stenosis, the number of patients who have benefited from this procedure has increased considerably [3]. Afterwards, TAVR has expanded its addressability also in patients with moderate or even low cardiovascular risk due to increasing operators’ experience, improvement of the technique and several advances in this field [4].
Several transcatheter heart valve systems with established safety and efficacy profiles are currently available, with the most widely utilized being the self-expanding CoreValve Evolut (Medtronic) and the balloon-expandable SAPIEN valve (Edwards Lifesciences) [5]. Each valve type exhibits distinct advantages and limitations. Self-expanding transcatheter valves are generally associated with superior hemodynamic performance, characterized by larger effective orifice areas and lower transvalvular mean gradients, attributable to the supra-annular positioning of the prosthetic leaflets [5]. In contrast, balloon-expandable valves typically provide greater procedural accuracy and a lower incidence of paravalvular regurgitation, although they may demonstrate slightly higher transvalvular gradients when compared with self-expanding systems [5]. As life expectancy increases, the association of degenerative aortic stenosis and aortic aneurysms is more frequent [6]. Surgical AAA repair is considered to be a high-risk intervention for patients with comorbidities. For high-surgical risk patients with favorable anatomy, EVAR has emerged as a less invasive alternative to open AAA repair and is associated with a reduction in perioperative mortality compared to an open AAA repair, even though EVAR patients are mostly older and with major comorbidities [7].
A simultaneous approach, TAVR and EVAR, could be feasible is some patients. To our knowledge there are only a few cases of simultaneous aortic valve repair and EVAR presented in the literature, each with a different approach and different devices depending on patient characteristics [2,8].
To date, there have been no trials investigating whether simultaneous TAVR and EVAR improves outcomes compared to a two-step approach [9].
The European Guidelines on non-cardiac surgery [10] and the Guidelines on Valvular Heart Disease [1] suggest that in symptomatic patients, aortic valve replacement should be considered before the elective surgery. The fluid shifts, possible blood loss in the perioperative period and the possible complications that may occur with the procedure may lead to significant hemodynamic instability, fluctuations in systolic and diastolic pressures, that can cause severe complications like myocardial ischemia and acute heart failure, in a patient with a severely stenotic valve. Another aspect that should be taken into consideration is the possibility of displacement of the aortic endoprosthesis when advancing with the valve.
The transfemoral approach in the TAVR procedure is the preferred, less invasive alternative, and it also allows the abdominal aortic aneurysm to repair using the same access site.
Performing TAVR and EVAR as a combined procedure offers several advantages over a sequential approach. First, it may reduce the risk of aneurysm rupture. Following TAVR, the elimination of the aortic valve pressure gradient often leads to an increase in systemic blood pressure. If EVAR is delayed, this rise in pressure may stress the AAA, potentially increasing the risk of rupture. By performing both procedures during the same session, the AAA is promptly excluded from circulation, avoiding this period of heightened vulnerability. On the other hand, the combined procedure minimizes invasiveness and associated complications. Using a single vascular access site for both procedures reduces the cumulative risk of vascular complications, such as bleeding or access-site trauma. These complications are not uncommon after EVAR, with reported complication rates in the specialized literature around 8% [11]. For comparison, the CoreValve US Pivotal Trial reported major vascular complications in 5.9% and life-threatening/disabling bleeding in 13.6% of patients undergoing TAVR [11]. Performing both procedures together also avoids the need for repeated general anesthesia, further lowering procedural risk.
Also, combining the procedures leads to a shorter hospital stay, which is particularly beneficial for elderly patients with multiple comorbidities—such as those typically referred for TAVR—who are at increased risk for complications during prolonged admissions [8-11]. But the second patient presented vascular complications which required prolonged hospitalization.So, the two clinical cases presented in this manuscript highlight the importance of patient individualized management decision, considering their comorbidities, frailty and particularities. In both cases, TAVR was performed first, followed by EVAR in the same procedure. This decision was based on the clinical status due to severe aortic stenosis, being hemodynamically fragile. Performing non-cardiac surgery such as EVAR under these conditions could have resulted in hemodynamic collapse or cardiogenic shock, from which recovery would be extremely difficult without prior valve stabilization. Although performing TAVR first poses associated risks too, such as potential AAA rupture, distal embolism, or aortic dissection due to the traversal of large delivery systems through the aneurysmal segment. In both cases the device delivery was uneventful. These two cases demonstrate that a combined TAVR and EVAR approach in high-risk patients is feasible and relatively safe. Performing both procedures in a single session can reduce perioperative risks, minimize anesthesia exposure, and shorten recovery time. However, the risk of complications including hemodynamic instability— vascular complications requiring surgical intervention, and prolonged hospitalization—may also occur in a combined single procedure in these elderly high-risk patients. Concomitant TAVR and EVAR requires favorable vascular anatomy, including adequate landing zones for the abdominal endograft, as well as femoral access sites. However, even when these anatomical criteria are met, synchronous repair may still carry a risk of vascular complications. Until now the management of these patients is debatable and there is no clear consensus or guideline of which procedure should be performed first.
There are some concerns when the aortic valve replacement is performed first during the combined procedure mainly due to the risk of vascular injury during the advancement of the valve. But a staged intervention may increase the strain and pressure within the walls of the aneurysm and can lead to distension and rupture because one of the short-term effects of TAVR is the rise of the systolic arterial blood pressure [12].
The right sequence of TAVR and EVAR in the combined procedure in these situations should be individualized to each patient, and decision needs to be made by a multidisciplinary team of experts, a group composed of vascular surgeon, interventional cardiologist, anesthesiologist and interventional radiologist. In our cases we decided to perform TAVR and improve the hemodynamic status of the patients first. We considered the risk of distension and rupture of the aneurysm smaller than the cardiac adverse outcomes associated with performing the EVAR first.
The assessment of the presence and severity of the aortic regurgitation after TAVR is extremely important because of the increased morbidity and mortality associated with a more than mild paravalvular aortic regurgitation [13]. The main causes of paravalvular regurgitation are the discordance in the diameters of the oval-shaped aortic annulus with the circular prosthetic valve, that can lead to prosthetic under sizing or oversizing and the presence of degenerative calcification of the native aortic valve, that can then cause prosthetic valve malpositioning [14]. In our cases the paravalvular leaks seemed to be mild and with no hemodynamic effect.
Regarding the aortic endograft, there is still no consensus about the optimal management of the type II endoleak due to lumbar branches that allow retrograde flow into the aneurysm. Given their benign course and the frequent spontaneous resolution, usually close follow-up rather than any form of intervention is recommended [13].
A potential concern with the simultaneous approach can be the greater risk of contrast-induced nephropathy (CIN) development, mainly because of the higher dose of radiocontrastused. Nevertheless, there is data suggesting that the risk of CIN is modest and may be overestimated, especially among patients who are not considered at risk (particularly no chronic kidney disease or diabetes) [15,16]. In our two cases, the patients tolerated the combined procedures well, with no occurrences of CIN following the interventions, as evidenced by stable renal function parameters. Serial measurements of serum creatinine and estimated glomerular filtration rate (eGFR) demonstrated no significant decline post-procedure. Even though, the second patient presented vascular access-related complications, they were successfully managed. The simultaneous approach contributed to an early postoperative recovery in the first case, where the evolution was uneventful with available follow-up, although longer-term follow-up data remain limited. In the second case, the postprocedural course was complicated by embolic vascular events re-quiring peripheral angioplasty and surgical intervention for superinfection at the femoral access site. However, the patient was eventually dis-charged in a hemodynamically stable condition with significantly im-proved cardiac status. At the 3-month followup, the patient demonstrated near-normal clinical and laboratory parameters, reporting a significantly improved quality of life and marked relief of symptoms.
A simultaneous TAVR and EVAR may be performed in highly selected patients with concomitant aortic valve stenosis and AAA. With growing clinical experience, this combined approach may evolve into a standard of care for carefully selected high-risk individuals.