Kawasaki disease (KD) is an acute, idiopathic, systemic vasculitis affecting predominantly children under 5 years of age with an annual incidence of 9-25 per 100,000 in developed countries and is the leading cause of acquired heart disease in children [1]. Without treatment, there is a significant risk of coronary artery involvement, which can lead to coronary artery aneurysms in up to 25% of untreated patients [1]. Risk factors for coronary artery lesions include high C-reactive protein (CRP), low albumin levels, and refractory KD [2,3]. Furthermore, large coronary aneurysms, occurring in only 1-2% of treated cases, significantly increase mortality risk and may persist into adulthood, potentially leading to thrombosis, stenosis, and myocardial infarction despite appropriate initial therapy [1,2]. However, predicting coronary artery involvement remains challenging, and novel biomarkers may help personalize therapy. We present a clinical case of rapidly progressing coronary aneurysms that developed despite timely treatment with intravenous immunoglobulin (IVIG), highlighting a typical and severe course of KD.
A 3-year-old child with a recent KD diagnosis was referred to a tertiary hospital for suspected coronary artery dilatation, requiring further evaluation and management. The child had been in his usual state of health until 15 days prior to the current admission, when he developed a persistent, remittent fever lasting 5 days, followed by the onset of a widespread maculopapular rash on the trunk, palms, and groin. On physical examination, the child weighed 16 kg, had a height of 98 cm, and had a calculated body surface area of 0.62. The oropharynx was hyperemic, with slightly hypertrophic, symmetrical tonsils. Unilateral submandibular lymph nodes (approximately 18 mm in diameter) were noticed, with bilateral, hyperemic, non-exudative conjunctival injection. Therefore, the patient fulfilled the complete diagnostic criteria for Kawasaki disease, exhibiting fever persisting beyond 4 days, accompanied by polymorphous exanthem, non-exudative bulbar conjunctival injection, erythematous changes of the oral and pharyngeal mucosa, and cervical lymphadenopathy. Heart sounds were rhythmic, with no abnormalities. The child was breathing normally, with an increased respiratory rate due to fever, but without signs of respiratory distress. Pulmonary auscultation revealed normal breath sounds in all areas without additional pathological sounds. Blood tests revealed lymphocytosis, a mild degree of anemia (hemoglobin 11.9 g/dL), and a normal biochemical profile, except for aspartate aminotransferase (AST) 215 U/L, alanine aminotransferase (ALT) 110 U/L, albumin 2.8 g/dL, and altered inflammatory markers (CRP 16.5 mg/dL, procalcitonin of 10.7 μg/L). Coagulation tests revealed an altered INR of 1.44, fibrinogen 886 mg/dL, and an erythrocyte sedimentation rate (ESR) of 120 mm/h. Troponin and B-type natriuretic peptide were within normal values. Transthoracic echocardiography (TTE) showed normal left ventricular function and non-dilated coronary arteries (right coronary artery [RCA] of 1.5 mm, left main coronary artery [LMCA] of 1.8 mm). Initial treatment included intravenous hydration and ceftriaxone after blood cultures were taken. Chest X-ray and abdominal ultrasound ruled out infectious foci. Viral serologies were unremarkable. The SARS-CoV-2 polymerase chain reaction test was negative, and negative anti-spike IgG excluded prior SARS-CoV-2 infection. Given persistent fever spikes, worsening inflammatory markers, and clinical criteria consistent with KD, treatment with IVIG (2 g/kg/day) and antiinflammatory doses of aspirin (30 mg/kg/day) was initiated. These findings were consistent with a high Kobayashi score, indicating an increased risk of IVIG resistance (Na 133 mmol/L, ALT 110 U/L, neutrophil percentage >80%, CRP 16.5 mg/dl, disease onset at 4 days), and corticosteroid therapy with methylprednisolone (0.8 mg/kg twice daily) was added as adjunctive therapy. Within hours, clinical improvement was observed. In the following days, the child’s clinical status improved steadily, with a reduction in inflammatory markers, and the child was discharged with a treatment plan including prednisone, an antiplatelet dose of aspirin, and lansoprazole. On the 15th follow-up day, blood tests revealed leukocytes 23.110/mm3, hemoglobin 11.8 g/dL, platelets 736.000/mm3, CRP < 0.3 mg/dL, and ESR 111 mm/h. The TTE revealed coronary artery dilation and, consequently, the child was transferred to the Pediatric Cardiology
Unit for further evaluation and management.
On arrival, ECG demonstrated sinus tachycardia with a normal repolarization pattern (Figure 1). The TTE revealed a medium aneurysm of the RCA (Figure 2, Panel A-C), with a diameter of 5 mm (Z-score +7.8). The LMCA origin measured 3 mm (Z-score +1.6), and the proximal trunk of the LMCA (Figure 2, Panel D-E) measured 4 mm (Z-score +4.5). At the bifurcation of LMCA, a large aneurysm with a maximum diameter of approximately 8 mm (Z-score +10) was identified, with suspected thrombotic material observed within its lumen. The anterior descending artery (LAD) demonstrated a maximum diameter of 4 mm (Z-score +9). Given this suspicion of intracoronary thrombus, IV heparin was started, together with the overlapping of warfarin therapy until the INR was within the therapeutical range. Cardiac computed tomography (CCT) confirmed the coronary aneurysms, without evidence of intraluminal thrombi (Figure 3, Panel A-D).
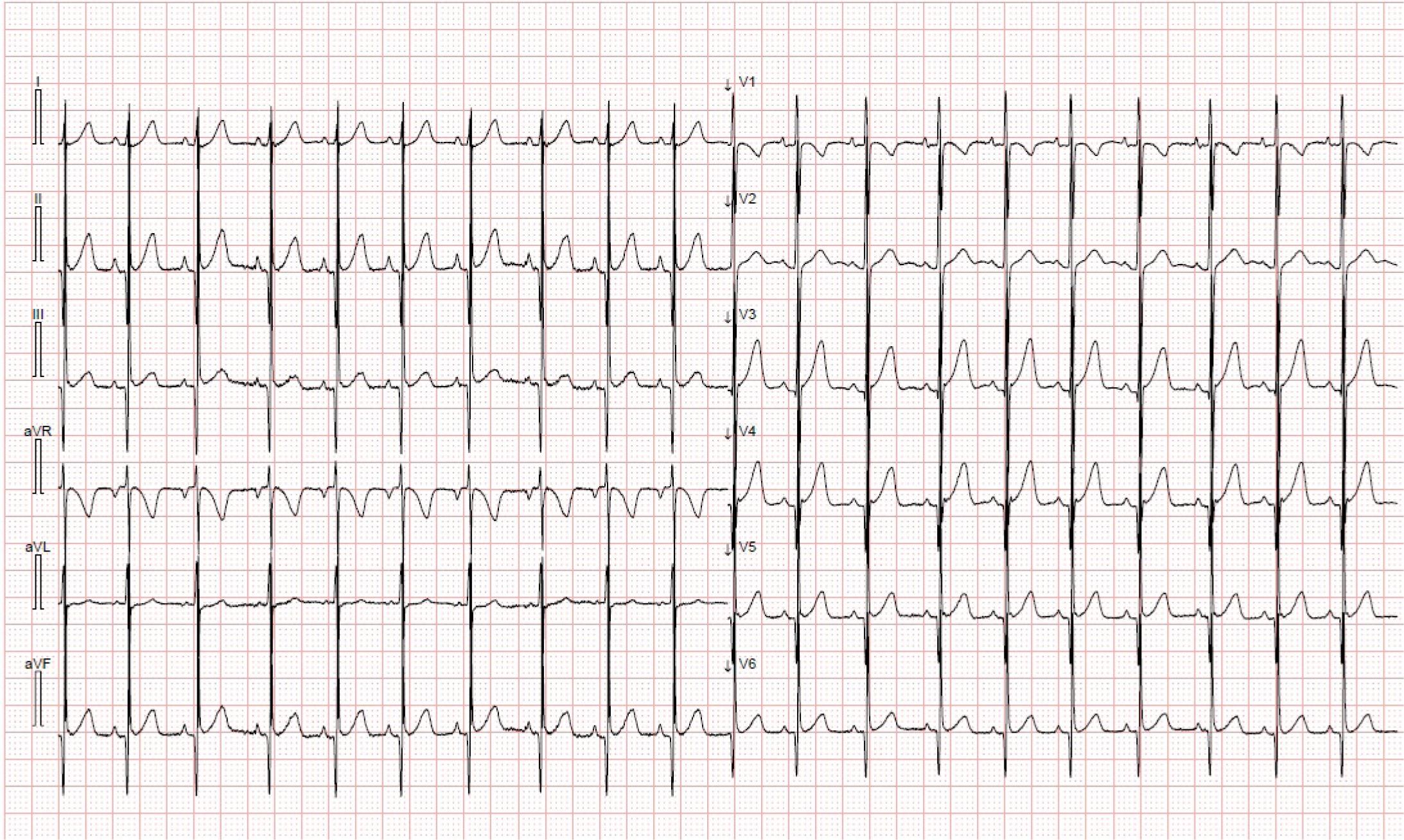
Surface 12-lead ECG depicting sinus tachycardia, with a normal repolarization pattern.
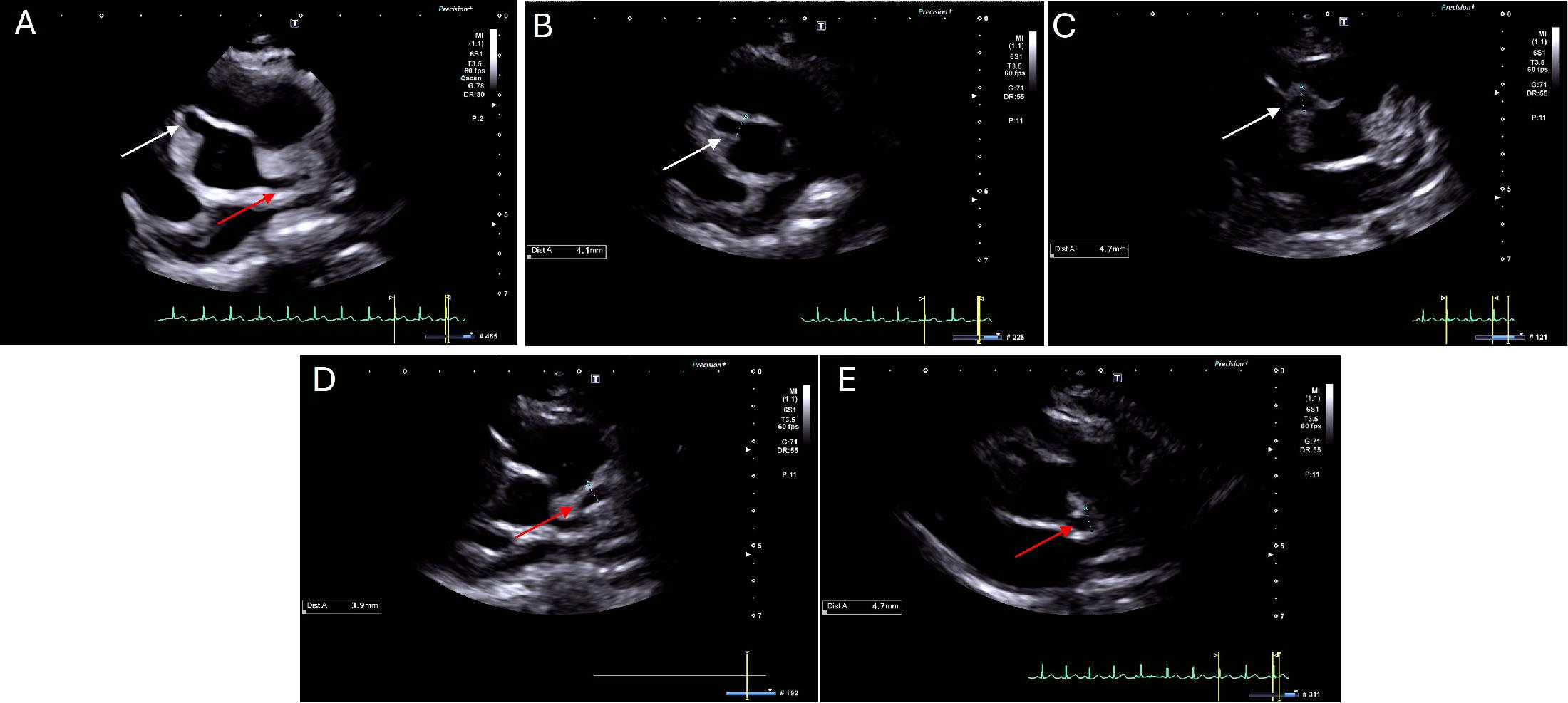
Transthoracic echocardiography in the parasternal short-axis view showing a right coronary artery aneurysm (Panel A, white arrow) and a left main coronary artery aneurysm (Panel A, red arrow). The proximal portion of the right coronary artery (Panel B, white arrow) has a diameter of 4.1 mm (Z-score +7.4), while the distal portion of the right coronary artery (Panel C, white arrow) has a diameter of 4.7 mm (Z-score +7.8). The left main coronary artery bifurcation (Panel D, red arrow) measured 3.9 mm (Z-score +4.9), while the proximal left anterior descending artery (Panel E, red arrow) measured 4.7 mm (Z-score +8.1).
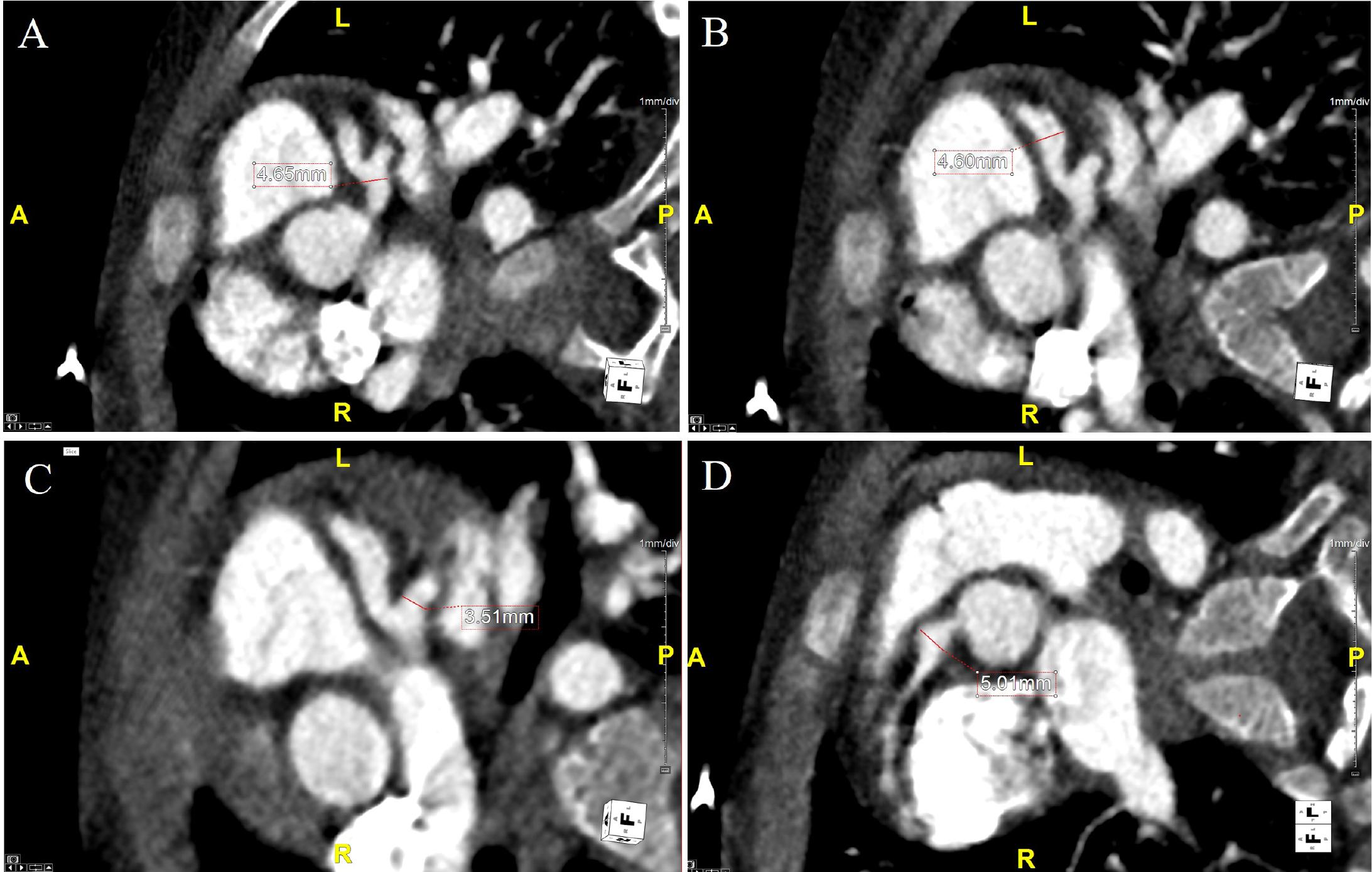
Cardiac computed tomography showing axial plane after multiplanar reconstruction of the left main coronary artery (Panel A) with a maximum diameter of 4.6 mm (Z-score +5.3); the left anterior descending artery (Panel B) with a diameter of 4.6 mm (Z-score +10.0); the circumflex artery with a diameter of 3.5 mm; The right coronary artery in axial reconstruction (Panel D) depicts a proximal diameter of 5 mm (Z-score +9.0).
Double antiplatelet therapy (DAPT) with aspirin (50 mg/day) and clopidogrel (3 mg/day followed by 6 mg/day) was also started due to the high risk of coronary thrombosis. Interleukin-1 receptor antagonist (anakinra, administered subcutaneously at a dose of 2 mg/kg/day, with subsequent dose escalation to 4 mg/kg/day) therapy was initiated to promote vascular remodeling and steroid therapy was discontinued, according to pedriatic rheumatology consultation. During the hospital stay, serial echocardiographic assessments were conducted to monitor the coronary aneurysms, which remained stable in size. The child did not experience precordial pain, and no electrocardiographic abnormalities were detected during the repeated evaluations. The patient was discharged with DAPT, warfarin, and anakinra. The first follow-up visit, performed six weeks after discharge, showed the LMCA measuring 3.8–4.0 mm, the LAD 4.1 mm, and the RCA 4.4 mm, leading to the discontinuation of anakinra. During the second follow-up, performed six weeks later, a minimal aneurysm was noted in the LMCA (3.4 mm, Z-score +2.4), with the RCA measuring 2.7 mm (Z-score +2.3) and the LAD 2.6 mm (Z-score +2.5), leading to the discontinuation of warfarin. The third follow-up, performed eight weeks later, revealed normalized coronary artery dimensions: LMCA 2.8 mm (Z-score +0.97), LAD 2.1 mm (Z-score +0.67), and RCA 2.1 mm (Z-score +0.56), at which point clopidogrel was stopped. The most recent TTE, performed 15 months after the initial diagnosis, showed normal coronary artery dimensions, and aspirin was discontinued. At two years of follow-up, the patient remained in good health status, with normal dimensions of the coronary arteries (Table 1).
Overview of the clinical course and ongoing management of Kawasaki disease in a young patient.
| Symptoms | Left main coronary artery | Left anterior descending artery | Right coronary artery | Treatment | |
|---|---|---|---|---|---|
| Diagnosis | Fever, maculopapular rash | 1.8 mm (Z-score -0.23) | - | 1.5 mm (Z-score -0.49) | IVIG, aspirin, corticosteroids |
| Follow-up 1 (15 days) | Asymptomatic | 3 mm (Z-score +1.6) | 4 mm (Z-score +9.0) | 5 mm (Z-score +7.8) | Aspirin, clopidogrel, heparin, warfarin, anakinra |
| Follow-up 2 (64 days) | Asymptomatic | 3.8 mm (Z-score +2.1) | 4.1 mm (Z-score +9.0) | 4.4 mm (Z-score +7.2) | Aspirin, clopidogrel, warfarin, anakinra |
| Follow-up 3 (145 days) | Asymptomatic | 3.4 mm (Z-score +2.4) | 2.6 mm (Z-score +2.5) | 2.7 mm (Z-score +2.3) | Aspirin, clopidogrel |
| Follow-up 4 (163 days) | Asymptomatic | 2.8 mm (Z-score +0.9) | 2.1 mm (Z-score +0.67) | 2.1 mm (Z-score +0.56) | Aspirin |
| Follow-up 5 (462 days) | Asymptomatic | 2.4 mm (Z-score -0.11) | 2.2 mm (Z-score +0.55) | 2.0 mm (Z-score -0.11) | Stop aspirin |
IVIG – Intravenous immunoglobulin
Despite important advancements in the last three decades, knowledge gaps still exist regarding the pathogenesis of KD and targeted therapies. KD reflects a balance between excessive immune cell activation, cytokine production, and its resolution.
The present case report presents a rare clinical scenario of rapidly evolving coronary artery aneurysms in a young patient with KD, despite prompt administration of IVIG and corticosteroids. Remarkably, regression of coronary abnormalities was observed during treatment with interleukin-1 inhibitors. Furthermore, this clinical case presents the atypical and severe nature of the disease, emphasizing the critical role of the immune system in its pathogenesis.
As described above, treatment with IVIG and anti-inflammatory doses of aspirin was initiated early after the KD diagnosis. Moreover, due to the presence of Na 133 mmol/L, ALT of 110 U/L, neutrophil percentage >80%, CRP 16.5 mg/dl, disease onset at 4 days, low albumin concentration, and skin rash, which are high-risk features for IVIG resistance, corticosteroid treatment was also started. Despite the implementation of IVIG, high-dose aspirin, and intravenous corticosteroids, 15 days later, the patient developed coronary aneurysms. Failure of standard treatment in this case suggested the involvement of refractory mechanisms, potentially mediated by cytokines not directly targeted by the initial therapies.
The immune system plays a crucial role in KD pathogenesis, characterized by increased cytokine production and immune cell activation [4]. The most prominent immunological abnormalities in KD patients include activation of T cells, B cells, and monocytes, with a deficiency in suppressor T cells [4]. Cytokine production is a key contributor to the pathogenesis of coronary aneurysms in these populations. Among them, tumor necrosis factor-α (TNF-α) is essential for coronary artery inflammation and aneurysm formation. Experimental studies have shown that mice treated with the TNF-α inhibitor etanercept, as well as TNF receptor 1-deficient mice, exhibit resistance to both coronary inflammation and the formation of coronary aneurysms [5].
The fragile link between IL-1, extracellular matrix (ECM) abnormalities, and the development of coronary aneurysms emphasizes the essential role of vascular remodeling in KD pathogenesis. In addition to its pleiotropic pro-inflammatory effects, IL-1 is a key cytokine that drives inflammatory responses within the vascular wall, promoting degradation of the ECM, especially through the upregulation of matrix metalloproteinases and inhibition of ECM repair processes. This imbalance between ECM degradation and synthesis contributes to the weakening of the vascular structure, facilitating aneurysm formation. Moreover, multiple studies have indicated compromised endothelial function in patients with KD, and recent data suggest that the severity of endothelial dysfunction appears to correlate with the duration of fever during the acute phase of KD [7]. As mentioned above, our patient experienced persistent, remittent fever at the onset of KD, a clinical characteristic that aligns with reports linking the duration of fever during the acute phase of KD with the severity of endothelial dysfunction [7]. This prolonged febrile status may have contributed to the pronounced vascular inflammation and to the subsequent development of coronary artery aneurysms observed in this case.
Understanding the complex relationship between IL-1 signaling, ECM alterations, and vascular remodeling is essential for elucidating the mechanisms underlying coronary artery complications in KD and for identifying novel therapeutic targets to reduce disease severity.
Interleukin-1 receptor blockers have been used in patients with KD, particularly in cases resistant to standard therapies, and the tolerability and safety of anakinra were demonstrated in a phase II open-label study [1,8]. Anakinra inhibits both the action of IL-1α and IL-1β, decreasing systemic inflammation and protecting the vascular endothelium from additional damage. Dosing regimens of anakinra vary, and both subcutaneous and intravenous administrations are being used. However, some studies suggested that intravenous use may be associated with higher sustained concentrations compared with subcutaneous administration [9]. Alternative biologic agents, including etanercept and infliximab, were considered in our therapeutic approach. However, anakinra was ultimately selected due to its superior efficacy in IL-1-mediated autoinflammatory conditions, favorable safety profile in pediatric patients, and emerging evidence supporting its use in IVIG-resistant Kawasaki disease with coronary complications. Anakinra’s shorter half-life also allows for more rapid dose adjustments and treatment cessation if necessary [1, 8, 9]. Due to personal preferences, a subcutaneous regimen was started, with our patient receiving 2 mg/kg/day for two consecutive days, followed by an increase to 4 mg/kg/day with periodical echocardiographic monitoring. In this case, the use of anakinra resulted in a significant improvement in the echocardiographic appearance of the coronary aneurysm, suggesting that the refractory inflammation was at least partially caused by IL-1. Bossi et al. reported anakinra administration in a pediatric patient with severe KD featuring large coronary aneurysms refractory to IVIG and corticosteroid treatment. The documented clinical stabilization and coronary aneurysm regression parallel our case’s response, further supporting IL-1 pathway inhibition as a targeted therapeutic approach in managing severe coronary complications of KD [10]. Also, Gambacorta et al. documented anakinra administration in patients with coronary aneurysms despite standard IVIG, steroid therapy, and infliximab. Their findings demonstrated significant inflammatory marker reduction and coronary aneurysm stabilization following anakinra initiation, supporting our therapeutic decision in a clinical scenario with persistent inflammation despite conventional treatment [11]. These observations suggest that patients with KD and coronary involvement may benefit from targeted therapies.
The implementation of triple antithrombotic therapy in this case (DAPT and oral anticoagulation), despite its Class IIb recommendation, was based on the patient’s substantiated prothrombotic risk profile. Therefore, given the patient’s presentation with a large coronary aneurysm, a condition associated with significantly elevated thrombotic risk, and the hypercoagulable state from KD (as evidenced by high levels of fibrinogen), our clinical team implemented triple antithrombotic therapy after comprehensive discussion of available treatment option with the parents during the shared decision-making process. Evidence supports this approach in KD with coronary aneurysms: Manlhiot et al. demonstrated a 4.2-fold increase in thrombotic risk in these patients [12]. The hypercoagulable state in KD is well-documented, with Yokoyama et al. reporting significantly elevated fibrinogen and D-dimer levels [13]. In untreated large aneurysms, Tsuda et al. reported a 31.8% cumulative incidence of thrombosis over 10 years versus 2.8% in anticoagulated patients [14]. Moreover, the relationship between sequelae of coronary aneurysm and atherosclerosis is well-defined since the vascular remodeling continues within the coronary arteries even after the KD regression [15,16, 17].
Beyond the pathophysiological mechanism and the treatment of KD, TTE remains the primary imaging modality for the acute and long-term evaluation of these patients, but CCT is essential for comprehensive coronary evaluation, allowing the visualization of both the proximal and distal segments of the coronary arteries. Also, CCT can help identify coronary artery stenoses and thrombosis in certain populations [18,19]. The involvement of the proximal segments of LMCA and RCA in this clinical case aligns with findings reported in the literature, emphasizing the importance of serial echocardiographic assessment, which allows detailed visualization of the proximal coronary artery segments [20].
The present case depicts a challenging and severe course of KD, with rapidly progressing large coronary aneurysms despite early standard treatment, in a young patient, but with a favorable response to interleukin-1 inhibitors. The complete resolution of large coronary aneurysms in this case is particularly significant, as such extensive lesions typically show limited regression with conventional therapy alone. This experience suggests that early implementation of anakinra in young, IVIG-resistant patients with coronary complications may offer an opportunity for substantial vascular recovery. Therefore, this case emphasizes the importance of the molecular pathways that influence the severity of KD and the need for tailored therapies, based on the patient inflammatory profile.