Bisphenol A (BPA) is a derivative of diphenylmethane with two hydroxyphenyl groups, used in the production of polycarbonate plastics and epoxy resins1,2. Nowadays, BPA-based products are utilized in the manufacturing of a wide range of consumer goods, from plastic food containers and plastic bottles to medical devices and stationery products3. With the widespread use of BPA-based products, this chemical has become ubiquitous. Human exposure to BPA is therefore continuous, most frequently occurring through ingestion, dermal/ocular contact, and/or inhalation4. Several studies assessing human exposure have shown that over 90% of the general population exhibits detectable levels of BPA in various biological products5. Analyzing over 80,000 urine samples from the general population, Wang et al. reported an average daily intake of BPA of approximately 2.53 μg/individual/day6.
Continuous exposure to BPA is concerning, given epidemiological studies that indicate an association between BPA and a large range of pathologies, including oncological diseases, diabetes mellitus, obesity, skin and respiratory tract irritations, autism, Alzheimer’s disease, cardiovascular pathologies, and others7–12.
Both in vitro and in vivo studies have demonstrated that BPA can bind to several nuclear receptors, such as estrogen receptors (ERα and β). BPA selectively binds to ERα and ERβ, with a higher affinity for ERβ13. Both ERα and ERβ have been identified in various cardiac cells, such as atrial and ventricular myocytes, endothelial cells, and fibroblasts14. Thus, chronic BPA exposure is expected to have relevant effects on the cardiovascular system.
Indeed, epidemiological studies have shown associations between BPA exposure and an increased prevalence of cardiovascular diseases, including atherosclerosis, stable coronary artery disease, myocardial infarction, peripheral arterial disease, dilated cardiomyopathy, heart failure, and arrhythmias. A recent meta-analysis published by Moon et al., which included over 22,000 patients, reported a 16% higher risk of developing cardiovascular diseases among BPA-exposed populations15.
In isolated ventricular cells from female rats exposed to acute BPA infusion at clinically relevant doses, an increase in the rate of spontaneous after depolarizations was observed16. In a recent study, exposure to supraphysiological doses of BPA resulted in a significant atrial proarrhythmic effect in female rats17. The mechanisms underlying the atrial and ventricular proarrhythmic effects of BPA are not yet fully understood. Furthermore, there exists a significant gap in our understanding of the direct influence of BPA on ECG parameters, particularly concerning the durations of various ECG elements that are critically important for predicting the occurrence of supraventricular and ventricular arrhythmias in clinical practice. A comprehensive understanding of these mechanisms is essential for advancing our knowledge of the impact of BPA on cardiac electrophysiology and for informing potential clinical assessments and interventions.
Accordingly, in the present study, we aimed to thoroughly evaluate the effects of chronic exposure to BPA at doses that are relevant to common human exposure, as well as at supraphysiological doses, on various ECG parameters in rats.
The experiments in the current study were conducted on adult female Wistar rats, in accordance with the International Council for Laboratory Animal Science Guidelines (Directive 2010/63/EU), with prior approval from the local Ethics Committee. All animals were housed individually, in a controlled environment, with a 12/12-hour light/dark cycle and free access to water and food. A total of 21 adult female Wistar rats were randomized into three groups: Control (n = 7), BPA (n = 7), and hBPA (n = 7). The animals in the BPA and hBPA groups were administered BPA (Sigma-Aldrich; St. Louis, MO) in the drinking water for 7 consecutive weeks: The BPA group received a dose of 50 μg/kg body weight/day, considered relevant for common human exposure based on previous studies18; and the hBPA group received 25 mg/kg body weight/day of BPA, considered a supraphysiological dose19. The rats in the Control group were provided with regular water, without any BPA addition, throughout the study.
After six weeks of BPA or vehicle administration, all animals were implanted (under inhalation anesthesia with 2.5% isoflurane, 4 L, 99.5% O2) with an ECG radiotelemetry device (Data Science International; St. Paul, MN), placed in a dorsal subcutaneous pocket. The two ECG electrodes were tunneled subcutaneously in a bipolar limb lead II configuration. The ECG signals were captured using receivers placed under each cage, converted into analog signals, and directed to a computer equipped with an acquisition board and a custom-designed acquisition program developed in the laboratory using LabVIEW 2009 software (National Instruments; Austin, TX.), as described previously20.
Following one-week of postoperative recovery, continuous 24-hour ECG recordings were performed on all animals. All recorded ECG traces were analyzed using a dedicated software developed with LabVIEW 2010 (National Instruments). For each animal, the mean heart rate/24 h (HR) and the durations of all ECG elements (i.e., the P wave, PQ segment, QRS complex, ST segment, T wave, and QT interval – Figure 1) were determined. The QT interval was measured from the beginning of the QRS complex to the end of the T wave, and the result was reported in ms. Based on previously published data in the literature, no correction formula for the QT interval in relation to HR was used21. Five consecutive cardiac cycles, obtained from ECG tracings recorded two hours after the start of the monitoring period, were evaluated for each animal. The study protocol is illustrated in Figure 2.
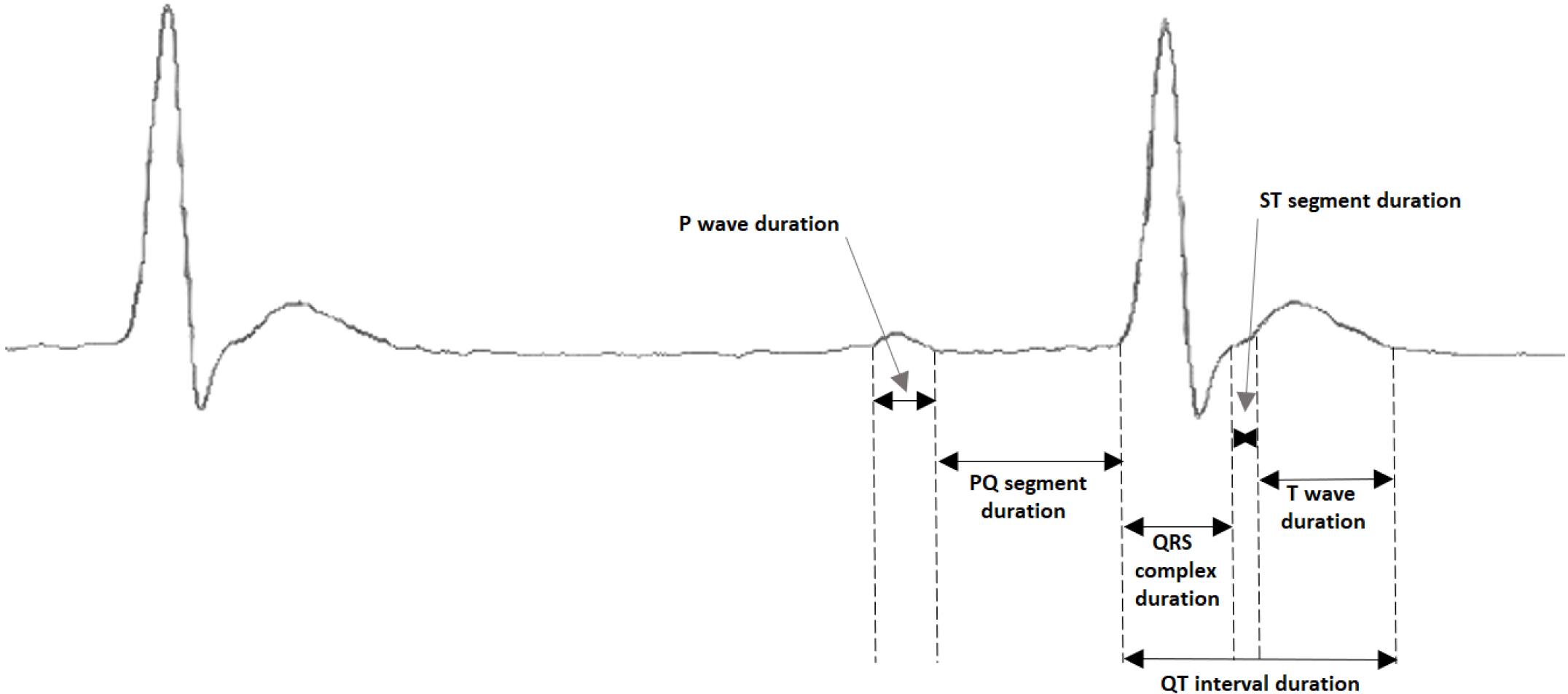
The ECG parameters measurement.
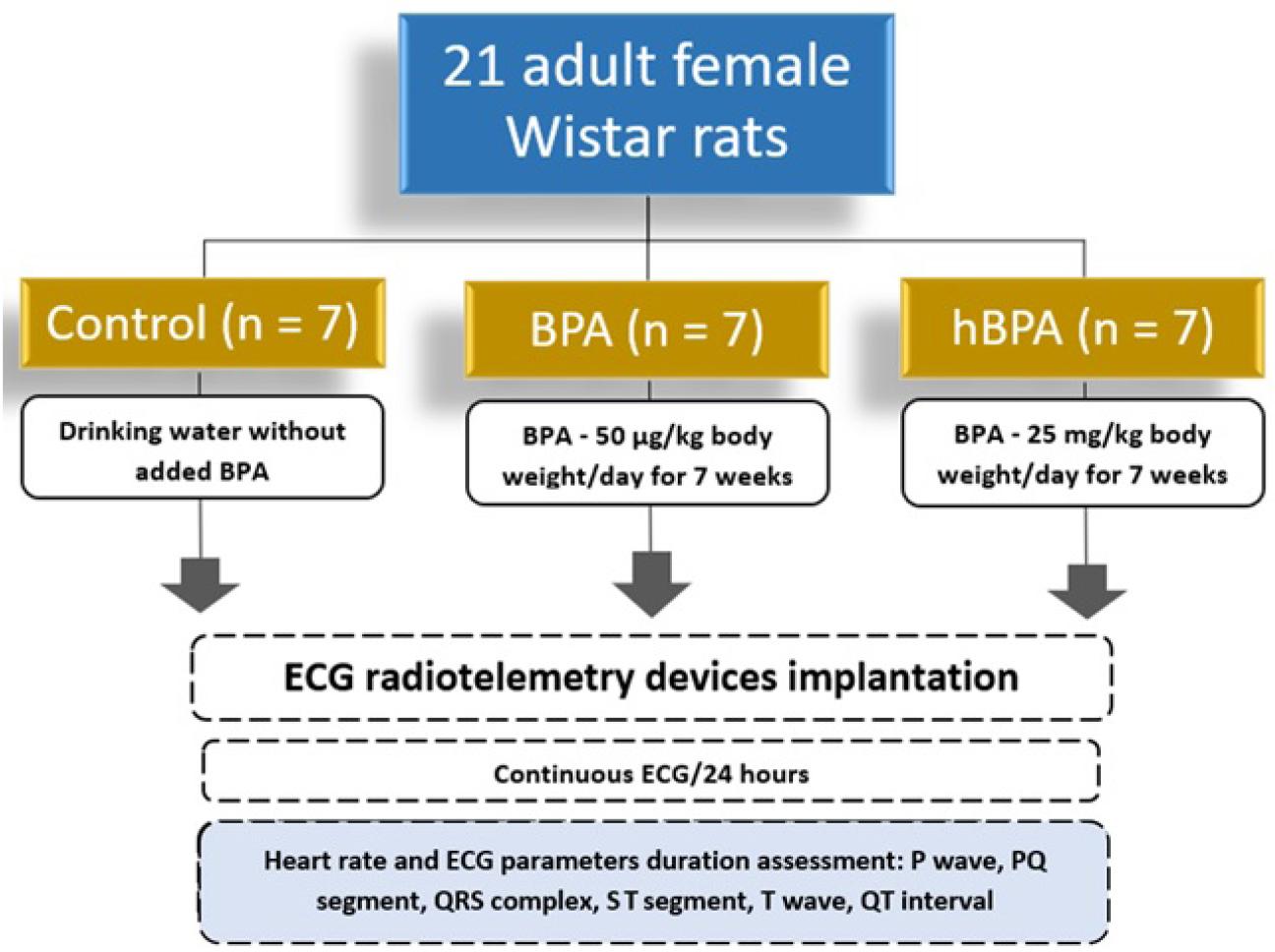
Schematic representation of the study protocol.
All statistical analyses were performed using GraphPad Prism version 8.0.2 (GraphPad Software; San Diego, CA). Given the small sample size, comparisons between groups for ordinal variables were conducted using the non-parametric Mann–Whitney U test. Multiple comparisons were performed using the Kruskal–Wallis test. Results are reported as median and interquartile ranges [25%; 75%]. A p-value of 0.05 was set as the threshold for statistical significance.
No significant differences were observed in the mean heart rate/24 h across the three groups, as all p-values exceeded 0.05. The Control group had a median heart rate of 312 bpm (303; 346), while the BPA group presented a median of 310 bpm (298; 347), and the hBPA group showed also a median of 310 bpm (304; 314). These findings indicate that heart rate measurements did not vary significantly between the Control and BPA or hBPA groups, as illustrated in Figure 3.
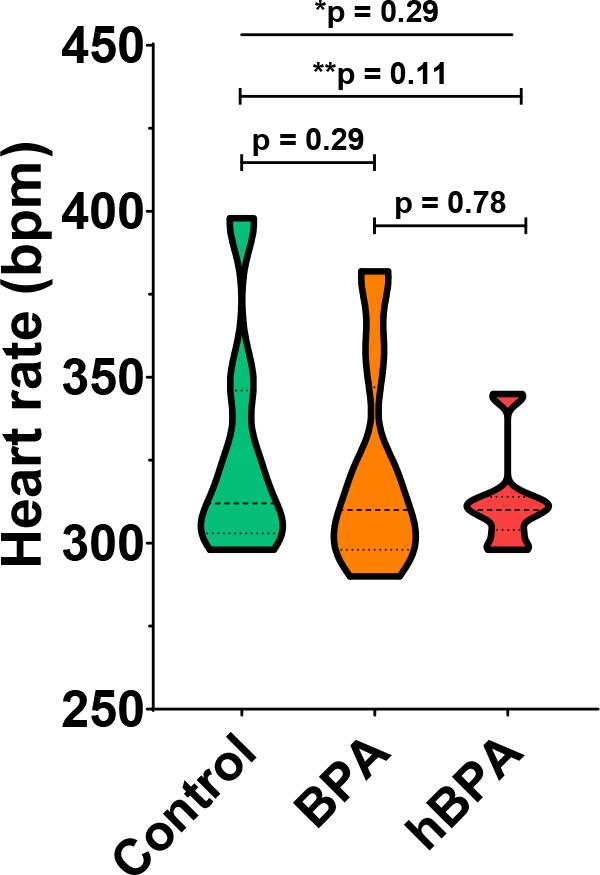
Heart rate in control rats and in rats exposed to human relevant (BPA) and supraphysiological (hBPA) bisphenol A doses for 7 consecutive weeks. Data are expressed as median and interquartile ranges; p-values were calculated using the Kruskal–Wallis and the Mann–Whitney U tests. * The p-value refers to the comparison between groups based on the Kruskal–Wallis test; ** the p-value refers to the comparison between the control and hBPA groups based on the Mann–Whitney test.
An analysis of P wave duration among the three groups revealed no statistically significant differences (all p> 0.05) - Figure 4A. The Control group exhibited a median P wave duration of 16.40 ms (16.10 - 16.90), while the BPA and hBPA groups presented median durations of 16.30 ms (16.10 - 16.60) and 16.30 ms (15.50 - 16.60), respectively. In contrast, the duration of the QRS complex was significantly longer in the BPA group (25.90 ms; 24.90 - 26.60) and the hBPA group (25.80 ms; 25.20 - 26.30) compared to the Control group (20.70 ms; 20.10 - 21.10; both p < 0.0001) – Figure 4B. However, no significant difference was observed between the BPA and hBPA groups (p = 0.62).
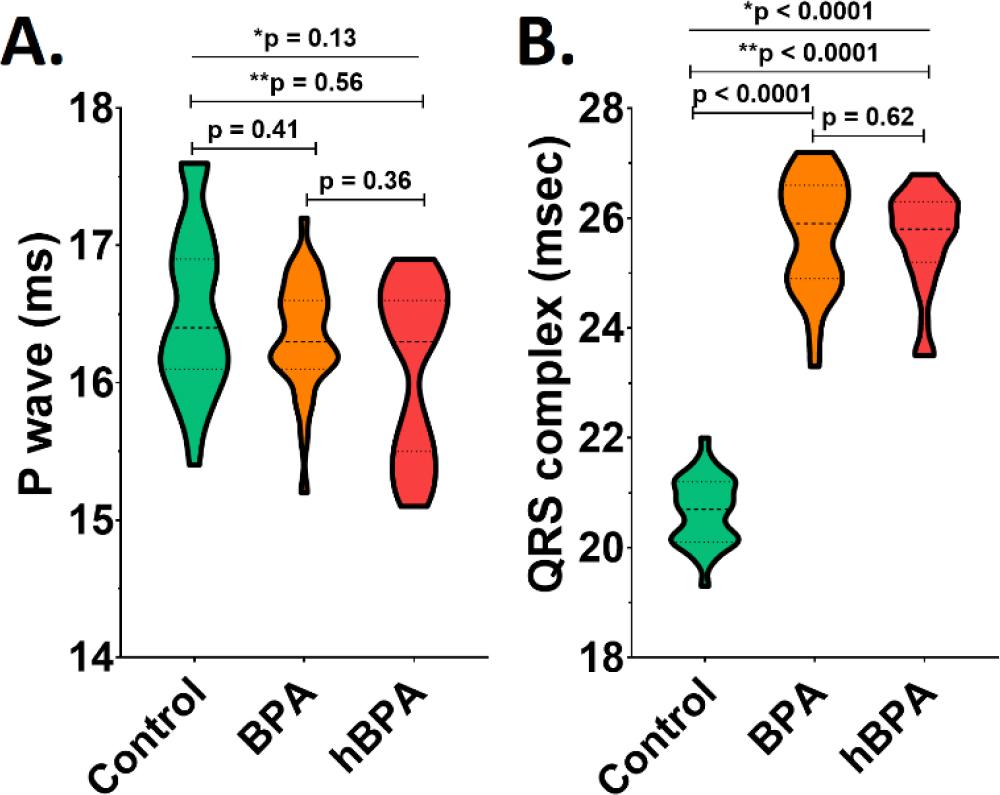
ECG parameters in control rats and in rats exposed to usual (BPA) and high (hBPA) bisphenol A doses for 7 weeks. The figure illustrates the duration of the P wave (A) and the QRS complex (B).Data are expressed as median and interquartile ranges; p-values were calculated using the Kruskal–Wallis and the Mann–Whitney U tests. * The p-value refers to the comparison between groups based on the Kruskal–Wallis test; ** the p-value refers to the comparison between the Control and hBPA groups based on the Mann–Whitney test.
Regarding PQ segment duration, significant differences were observed among the three groups (p< 0.0001) – Figure 5. Animals in the BPA (36.30 ms; 35.60 - 36.90) and hBPA (36.70 ms; 36.80 - 39.60) groups exhibited significantly longer PQ segment durations compared to those in the Control group (32.40 ms; 31.70 - 33.40; both p< 0.0001). However, no statistically significant difference was identified between the BPA and hBPA groups (p= 0.06).
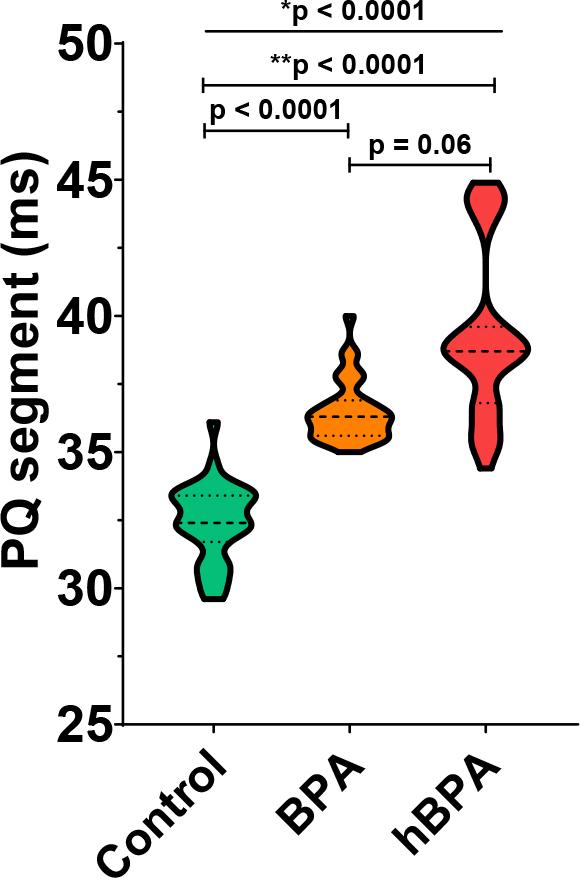
The duration of the PQ segment (ms). Data are expressed as median and interquartile ranges; p-values were calculated using the Kruskal–Wallis and the Mann–Whitney U tests. * The p-value refers to the comparison between groups based on the Kruskal–Wallis test; ** the p-value refers to the comparison between the Control and hBPA groups based on the Mann–Whitney test.
Significant differences were observed among the three groups in the ventricular repolarization phase, specifically in the duration of both the ST segment and the T wave (both p < 0.0001). The ST segment duration was significantly shorter in the BPA (4.60 ms; 4.10 - 5.20) and hBPA (4.80 ms; 4.40 - 5.20) groups compared to the Control group (6.30 ms; 6.10 - 6.80; both p < 0.0001), with no significant difference between the BPA and hBPA groups (p = 0.17) – Figure 6A. The animals in the Control (25.40 ms; 24.60 – 25.80; both p < 0.0001) group exhibited a significantly shorter T wave compared to the animals in the BPA (28.60 ms; 28.30 – 30.20) and hBPA (30.60 ms; 30.40 – 31.20) groups, with no significant difference between the BPA and hBPA groups (p = 0.09) – Figure 6B.
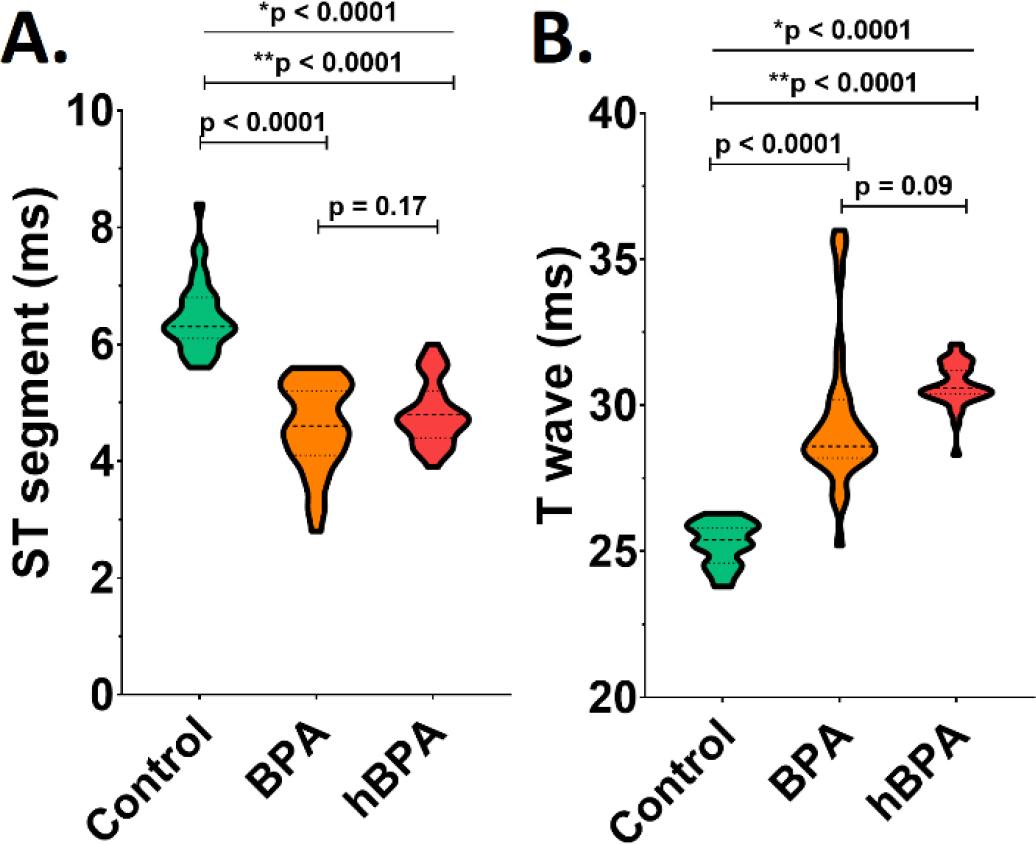
ECG parameters in control rats and in rats exposed to usual (BPA) and high (hBPA) bisphenol A doses for 7 weeks. The figure illustrates the duration of the ST segment (A) and the T wave (B). Data are expressed as median and interquartile ranges; p-values were calculated using the Kruskal–Wallis and the Mann–Whitney U tests. * The p-value refers to the comparison between groups based on the Kruskal–Wallis test; ** the p-value refers to the comparison between the Control and hBPA groups based on the Mann–Whitney test.
Significant differences were also observed among the three groups regarding the duration of ventricular electrical systole (p < 0.0001). The QT interval duration was significantly longer in the BPA (59.20 ms; 58.50 – 60.00) and hBPA (60.80 ms; 60.20 – 61.40) groups compared to the Control group (51.60 ms; 50.80 – 52.90; both p < 0.0001), with no significant differences between the BPA exposure doses (p = 0.11) – Figure 7.
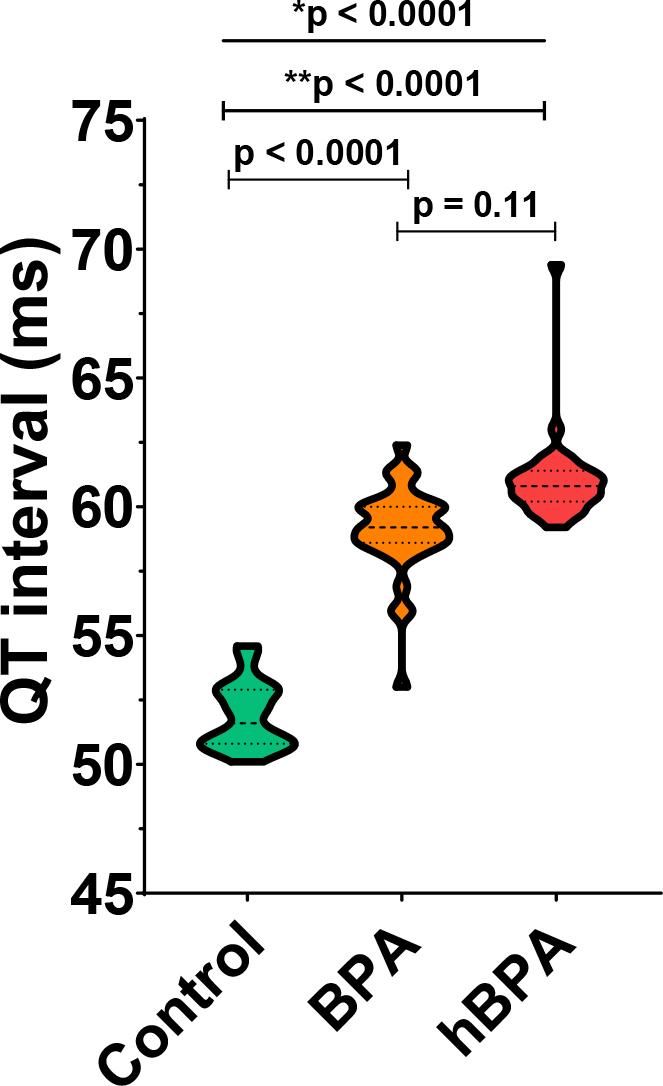
The duration of the QT interval (ms). Data are expressed as median and interquartile ranges; p-values were calculated using the Kruskal–Wallis and the Mann–Whitney U tests. * The p-value refers to the comparison between groups based on the Kruskal–Wallis test; ** the p-value refers to the comparison between the Control and hBPA groups based on the Mann–Whitney test.
The main findings of the present study were that chronic BPA exposure, in both human-relevant and supraphysiological doses, leads to significant changes in multiple ECG parameters, including the prolongation of the QRS complex, PQ segment, T wave, and QT interval, and a shortening of the ST segment duration, without affecting the P wave duration or the HR.
Experimental studies evaluating the impact of BPA on various pathologies have used different routes of exposure (e.g., intraperitoneal, gavage, etc.)22. In the present study, BPA supplementation in the drinking water was chosen as the route of exposure, as this method provides continuous administration, which is clinically much more relevant than administering a single high dose via other routes. Human exposure to BPA occurs through multiple pathways, including oral ingestion from drinking water or food stored in plastic containers23. Considering these aspects, the mode of BPA exposure used in this study can be seen as the most relevant in terms of human exposure.
In the current study, no significant differences in HR were observed among adult female Wistar rats exposed to either usual or high BPA doses compared to the Control animals. The available data on the effects of BPA on HR are extremely limited. A clinical study conducted in South Korea, including 560 participants, reported an association between increased urinary BPA concentrations and increased average HR, with a slightly less pronounced, effect in male compared to female individuals24. In vitro studies have provided the majority of the data on the potential effects of BPA on HR. In contrast to epidemiological findings, experimental studies generally appear to support a bradycardic effect of BPA exposure. An ex vivo study using intact rat hearts showed a significant decrease in spontaneous cardiac contraction frequency following acute exposure to various BPA concentrations (a 16% decrease at 10 μM and an 85% decrease at 100 μM), which was attributed to BPA’s interference with L-type Ca2+ channels activity25. Similar effects on chronotropism were observed in vitro on neonatal rat cardiomyocytes, with acute exposure to various BPA doses resulting in spontaneous discharge rate reductions ranging from 50.0% to 64.3%26. Chronic BPA exposure (8-10 weeks) in CD11 mice also resulted in a reduction in HR in vivo, as determined by ECG monitoring in “conscious”, unrestrained animals; however, this effect was only observed in male mice and not in females27. The latter results suggest a gender-specific effect of BPA on HR and might offer a hypothesis for why there were no differences in HR between the animals exposed to BPA and the controls in the current study.
Specific studies on BPA’s effects on ECG parameters are extremely limited. In the present study involving adult female rats, although exposure to BPA at both physiological and supraphysiological doses did not influence the duration of the P wave, both doses led to a significant increase in the duration of the PR segment. In a study conducted by Posnack et al., excised adult female rat hearts were exposed to BPA concentrations ranging from 0.1 μM to 100 μM. The electrical activity of the hearts was recorded using ECG electrodes and optical mapping to evaluate cardiac impulse propagation. Similar to the findings of the current study, the authors reported that BPA resulted in PR segment prolongation28. In another experimental study performed in CD1 male mice, chronic exposure to BPA at a dose of ≤ 50 mg/kg body weight/day for a four-week period resulted in a significant prolongation of both the PQ interval and the PR segment compared to vehicle-treated control mice (both p< 0.05). This finding suggests that BPA exposure may induce alterations in atrioventricular conduction, even at relatively short durations of exposure29. In line with the experimental data, including from the present study, a cross-sectional analysis of the Fernald Community Cohort, which included more than 600 patients, revealed a positive association between elevated urinary concentrations of BPA and bisphenol F and increased PQ interval duration in women. Importantly, this association was not observed in males, highlighting a potential sex-specific effect of BPA exposure on atrioventricular conduction30.
Research on the effects of BPA on the QRS complex is limited. In the Fernald Community Cohort, BPA exposure alone showed no significant impact on QRS duration in either sex. However, combined exposure to BPA and bisphenol F was associated with a slight increase in QRS duration in females, while no effect was observed in males30. An experimental study by Omodon et al. on male Wistar rats demonstrated no significant changes in QRS duration across groups exposed to BPA, suggesting no notable abnormalities in ventricular depolarization31. Meanwhile, our findings show that BPA causes a significant increase in QRS complex duration in female rats. These data are in line with those of Patel et al. on C57BL/6 mice, which revealed sex-specific alterations in cardiac electrical conduction following chronic BPA exposure, with BPA-exposed females exhibiting prolonged QRS complex durations after catecholamine challenge32.
In the present study, both human-relevant and supraphysiological doses of BPA led to a significant increase in QT interval duration. In the recent study by Ma et al., that investigated the effects of BPA on action potential parameters of canine ventricular cardiomyocytes using whole-cell patch clamp electrophysiological recordings, acute exposure of ventricular cardiomyocytes to BPA at a concentration of 10−9 M resulted in a significant prolongation of the action potential duration, which clinically corresponds to a prolonged QT interval. The study attributed the impact of BPA on ventricular repolarization to the inhibitory action of this compound on the rapid potassium current33. To further elucidate the effects of low-dose BPA on the electrical properties of cardiomyocytes in a human-relevant model, a study published in 2023 examined the acute effects of BPA at a concentration of 1 nM on cardiomyocytes derived from human pluripotent stem cells. Utilizing patch clamp techniques and confocal microscopy, the study demonstrated that acute BPA exposure led to prolonged repolarization and, consequently, to an increased duration of the action potential via inhibition of the hERG gene, critical for the synthesis of potassium channel components34.
By focusing on female rats, the present study addresses a gap in existing research and provides valuable insights into sexspecific effects of BPA exposure on cardiac electrical function. This targeted approach increases the study’s relevance to a specific subpopulation, particularly prone to BPA-induced abnormalities. In addition, the current study provides insights into the effects of both human exposure-relevant and supraphysiological doses of BPA, with significance in accidental or occupational exposure, such as in the case of workers in the plastics industry. A number of limitations should be considered when interpreting the findings of the present study. The study’s relatively short duration may not have fully captured the long-term effects of chronic BPA exposure on cardiac electrical function. A longer-term study could provide more insights into the chronic effects of BPA exposure. Also, the relatively small sample size (n = 7 per group) may have limited the statistical power of the study. Finally, to establish the clinical relevance of our findings, these results should be validated in human studies.
Significant alterations in ECG parameters were observed at both human relevant and supraphysiological BPA doses exposure. Specifically, prolonged PR, QRS, and QT intervals, coupled with shortened ST segments, indicate impairments in atrioventricular conduction and both ventricular depolarization and repolarization induced by BPA exposure, including at clinically relevant doses. These findings could translate clinically into an increased risk of cardiac arrhythmias. The observed effects highlight the need for additional research into the mechanisms underlying BPA’s cardiotoxicity and its potential implications for human cardiovascular health, particularly given the high human BPA exposure.