Rheumatic heart disease (RHD) is a chronic condition resulting from cumulative heart valve damage caused by a single severe episode or, more commonly, multiple recurrent episodes of acute rheumatic fever (ARF).[1] It typically occurs following exposure to group A streptococcal infections in genetically susceptible individuals. [2] Since RHD progresses over a long period, its prevalence peaks in adulthood, usually between 25 and 45 years.[1,3] Improvements in living conditions and the implementation of prophylactic measures have led to a significant decline in RHD prevalence, with near eradication in many developed countries. However, despite being largely preventable, the disease burden remains disproportionately high in developing regions, where access to primary healthcare is often limited.[4] Multivalve involvement complicates management, as not all lesions are severe at the time of the initial surgery and the disease is progressive.[5]
For young RHD patients, mechanical prostheses are typically required for durability, but the risk of morbidity and mortality due to thrombotic complications and bleeding from anticoagulation therapy with vitamin K antagonists (VKAs) remains excessively high. Additionally, over time, implanted valve protheses can lead to their own complications, often necessitating high risk redo surgeries and complex decision making.[5]
We present the case of a 71-year-old woman admitted to our clinic with progressive dyspnea and fatigue over the past two months. She has a complex medical history, which began at the age of 34 (1985) when she underwent mitral valve replacement with a tilting-disc mechanical prosthesis (Sorin 29) for severe rheumatic mitral stenosis. About twenty years later (2006), a bioprosthesis was implanted in tricuspid position for severe rheumatic tricuspid regurgitation. Just five months after this procedure the patient required a redo tricuspid replacement with a 25-mm mechanical bileaflet prosthesis due to early structural failure of the biological one. Postoperative transthoracic echocardiography (TTE) showed a structurally normal tricuspid prosthesis, but with a high mean transvalvular pressure gradient and an indexed effective orifice area of 0.5 cm2/m2, indicating severe patient-prosthesis mismatch (PPM). The patient’s medical history also includes permanent atrial fibrillation (AFib) and the implantation of a VVI cardiac pacemaker in 2011 for complete atrioventricular block, with left ventricular pacing via the coronary sinus. Her comorbidities include chronic kidney disease, gastritis, anemia and liver dysfunction associated with chronic hepatitis C virus infection, with undetectable viremia at the latest gastroenterological follow-up. Despite good compliance with her therapy regimen, she had labile international normalized ratio (INR) values while on VKAs.
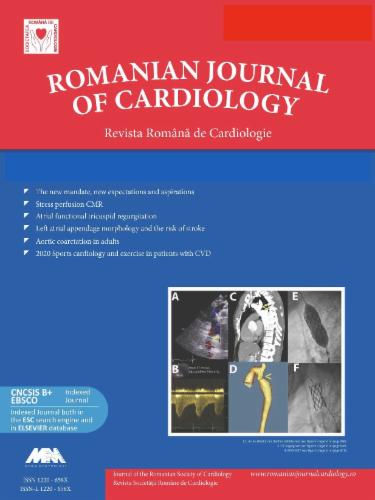
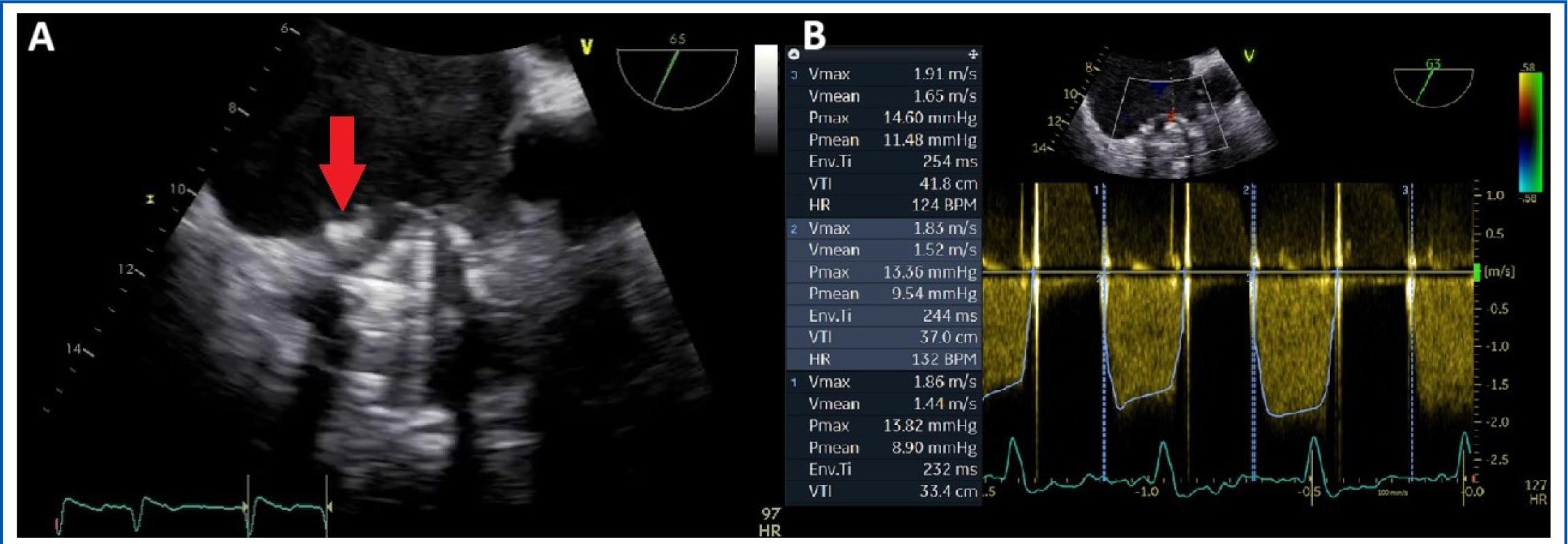
In 2014, the patient’s condition worsened due to an episode of aggravated heart failure. A TTE performed at that time revealed an immobile leaflet and severe obstruction of the tricuspid prosthesis. A comprehensive evaluation was conducted using multiple imaging modalities including transoesophageal echocardiography (TOE) and cinefluoroscopy in addition to TTE, which identified the underlying cause of the obstruction: both pannus and a small thrombus causing blockage of the lateral leaflet in a partially open position, in a patient already known with significant PPM (Figure 1). TOE images also revealed thrombosis of the pacing lead and in the left atrial appendage (LAA) (Figure 2).
Transoesophageal echocardiography. A) 2D-image showing a stuck leaflet of the tricuspid prosthesis due to both pannus and thrombus (red arrow). B) CW Doppler flow interrogation of the tricuspid prosthesis revealing high mean transvalvular pressure gradient (examination in atrial fibrillation).
Transoesophageal echocardiography. A) Pacing lead thrombosis (red arrow). B) Left atrial appendage thrombosis.
The patient was considered for reintervention to replace the tricuspid valve due to severe symptomatic dysfunction of the prosthetic valve. However, considering the high surgical risk associated with a repeated open-heart surgery, along with the patient’s stable clinical status following diuretic treatment (NYHA class II, normal BNP levels) and the small size of the thrombus (<5 mm), a conservative approach was eventually recommended. This approach focused on optimizing anticoagulation therapy, with unfractionated heparin combined with the AVK anticoagulant during hospitalization. A six month follow-up showed stable functional parameters of the tricuspid prosthesis, with significant symptom improvement and resolution of the pacing lead thrombosis.
In 2016, the pacemaker box was replaced. Two years later, in 2018, the pacemaker became dysfunctional due to intermittent non-capture. A new pacing lead was implanted in the coronary sinus, while the original pacing system was kept in place.
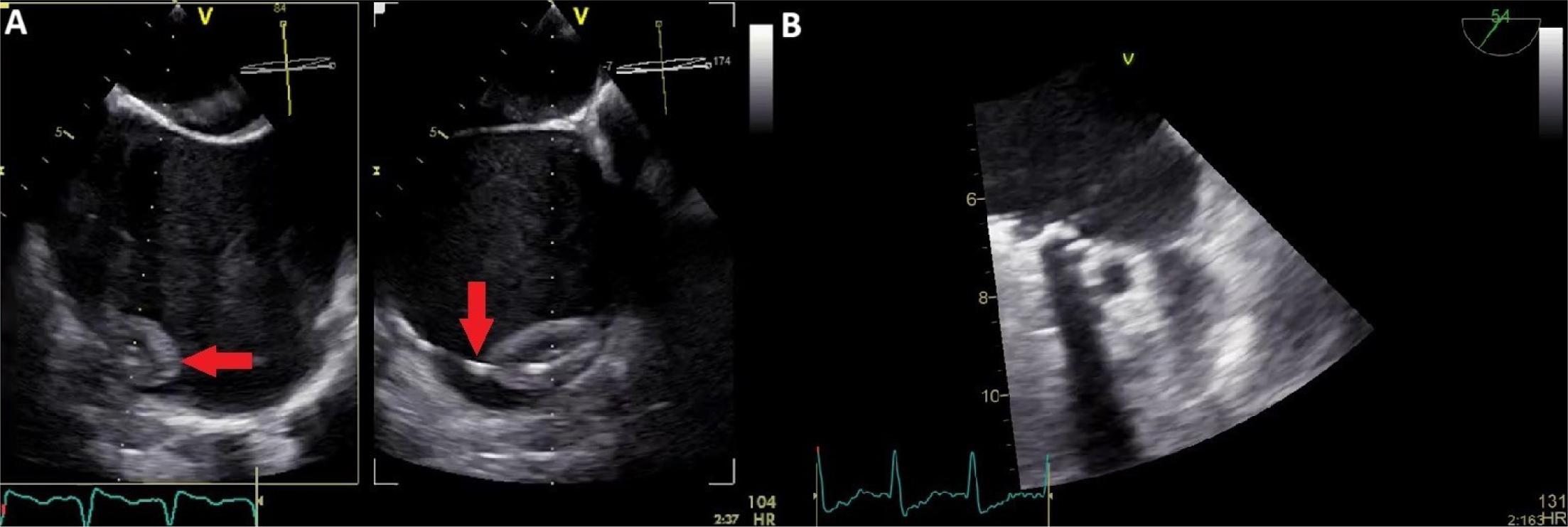
On current presentation, the patient was afebrile and hemodynamically stable, with signs of systemic congestion – jugular vein distention, liver enlargement and mild peripheral edema. Cardiac auscultation revealed a loud systolic murmur in the aortic area and the metallic sounds of mitral prosthesis in the mitral area. Laboratory tests showed a BNP of 466 pg/ml, an increased INR beyond the therapeutic range (4.3), mild anemia (Hb 10.2 g/dl) and mild renal dysfunction (creatinine 1.5 mg/dl), with no signs of an inflammatory syndrome. The electrocardiogram on admission indicated AFib with a ventricular-paced rhythm. Transthoracic echocardiography revealed a non-dilated left ventricle with preserved global systolic function, severe biatrial enlargement, a normally functioning mechanical mitral prosthesis and a severely dysfunctional (previously known) tricuspid mechanical prosthesis. The right ventricle was dilated, with mild systolic dysfunction, and an IVC of 20 mm was revealed, with <50% respiratory variation. Severe aortic stenosis (AS) was noted with significant progression of the valve lesion compared to previous evaluations (Figure 3).
Transthoracic echocardiography. A) 2D parasternal short axis view of the aortic valve showing severe valvular calcifications. B) CW Doppler interrogation showing high velocity transvalvular aortic flow.
Given the symptomatic severe aortic valve disease and the high surgical risk (EuroSCORE II 9.26% for single valve procedure and 14.78% for two major procedures), the Heart Team recommended transcatheter aortic valve replacement (TAVI). Coronary angiography was peformed prior to the TAVI procedure, revealing normal coronary arteries. One month later, the patient succesfully underwent aortic valve replacement with a 26-mm bioprothesis (Edwards Sapien 3). No early periprocedural complications were observed, and the patient was discharged with a recommendation for dual antithrombotic therapy, clopidogrel and acenocoumarol.
One month after TAVI, the patient presented to the emergency department with a right laterocervical pulsatile mass and newly developed hoarseness. An emergency computed tomography (CT) scan revealed a laterocervical hematoma extending into the mediastinum, with active bleeding causing a mass effect on adjacent structures (Figure 4). Surgical intervention was performed for bleeding control and drainage, while the anemic syndrome was corrected through blood transfusions with good outcome. The source of the bleeding was a pseudoaneurysm of a branch of the right subclavian artery, most likely developed due to central venous line manipulation during the prior hospitalization.
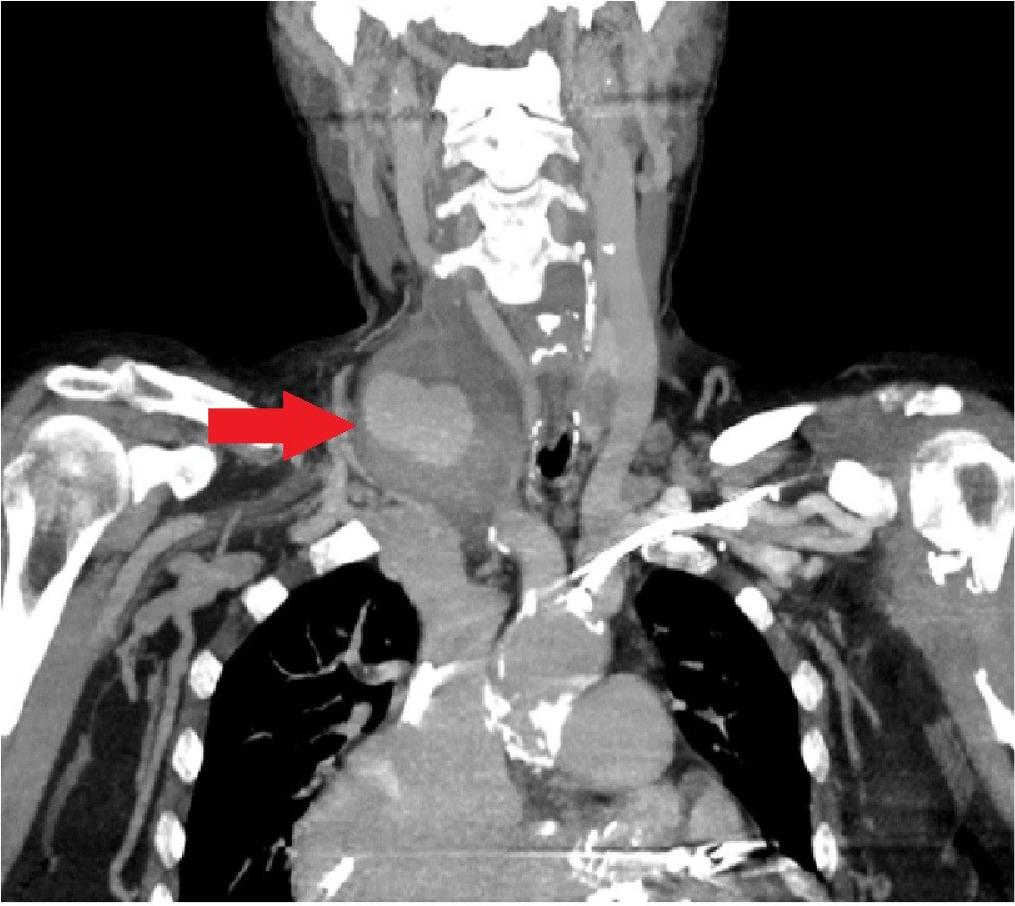
Computed tomography angiography shows a laterocervical pseudoaneurysm.
During the subsequent follow-up period, the patient experienced several hospitalizations due to recurrent presyncope, reporting significant variations in ventricular rate (50-140 bpm) at home – symptomatic primarily during episodes of slow heart rate. Holter ECG monitoring documented episodes of rapid AFib alternating with a ventricular-paced rhythm with intermittent failure to capture (pacing spikes not followed by QRS complexes), despite multiple attempts to reprogram the pacemaker. The issue was resolved upon realizing that the two pacing systems maintained in situ were interfering with each other due to their alternate interrogation at different times. Consequently, the most recently implanted device was reprogrammed to a non-functional mode and plans were made for its removal (Figure 5).
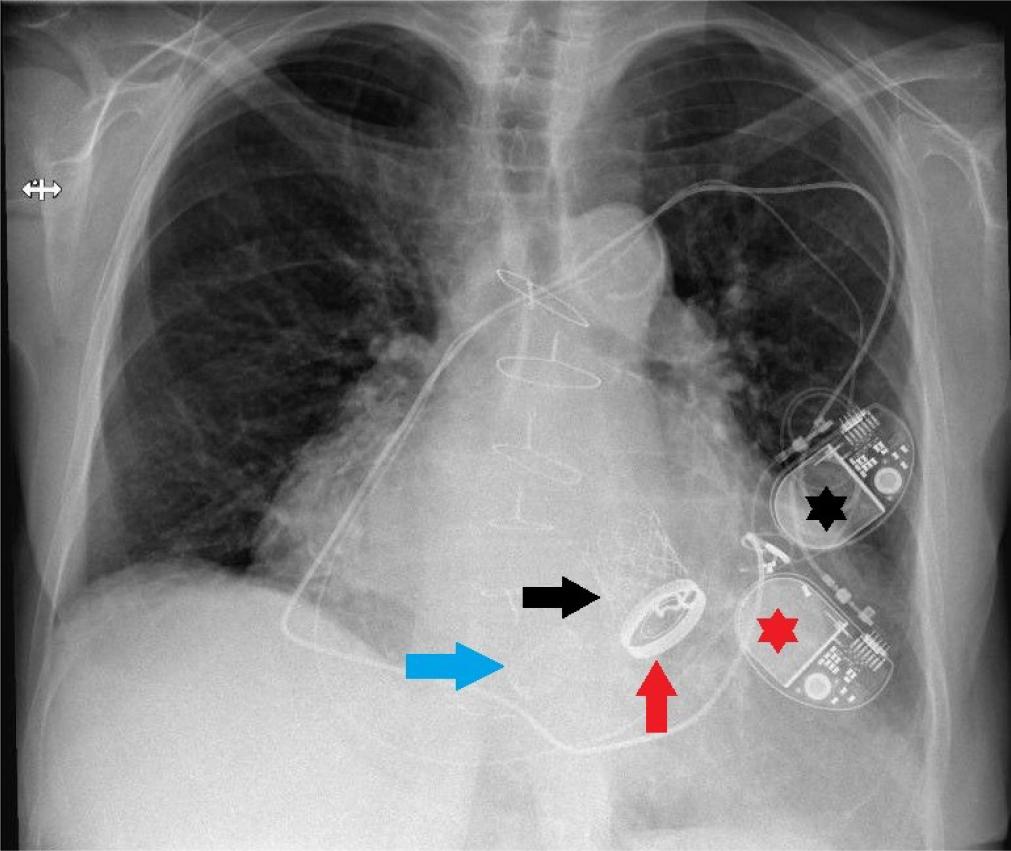
Chest X-Ray revealing the three different valve prosthese (blue arrow - tricuspid prosthesis, red arrow - mitral prosthesis, blac arrow - aortic prosthesis) and the two pacing systems (black asterisk first pacemaker, red asterisk - second pacemaker).
This case illustrates the intricate journey of a patient with RHD and complex multivalvular involvement, characterized by different valve lesions occurring and worsening sequentially, necessitating serial interventions – three valve replacements across four procedures involving various types of prostheses over a span of 36 years.
The natural history of RHD follows a slow, progressive pattern, typically becoming clinically manifest between the second and fourth decades of life.[4] The disease encompasses a spectrum of lesions that form the continuum of RHD. Carditis occurs in over 50% of patients with ARF and is predominantly characterized by valvulitis which manifests as valvular regurgitation.[1] Over time, chronic inflammation drives the transition from latent disease to permanent damage to the heart valves, representing established RHD. [6]
Rheumatic heart disease most commonly affects the left-sided valves, with a particular affinity for the mitral valve. Mitral valve incompetence is the most prevalent valvular lesion early in the disease process (subclinical RHD), while mitral stenosis typically develops later due to persistent or recurrent valvulitis and commissural fusion. Aortic valve involvement is the next most common, occurring in 20-30% of cases, typically associated with mitral valve involvement. In these patients, aortic regurgitation is much more common than stenosis. Right-sided valve involvement is less common in the rheumatic process. Tricuspid stenosis, when seen, almost always occurs alongside mitral stenosis, while tricuspid regurgitation is more frequent, but usually functional, resulting from the deleterious hemodynamic consequences of left-sided valve disease.[4–6]
Multivalve involvement in RHD is not always simultaneous and can pose significant challenges. As RHD is a progressive disease, clinicians often encounter patients who have previously undergone valve replacement and eventually present with significant dysfunction of another valve. This scenario requires high-risk redo surgery and often involves difficult decision making.[5]
Transcatheter aortic valve implantation has revolutionized the management of severe calcific AS over the last decade in industrialized countries. However, it is unlikely to play a significant role in rheumatic AS due to the rarity of isolated rheumatic AS, the relatively young age of these patients and the typically low level of calcification in rheumatic aortic valves.[2,3]
In our case, the patient had bivalvular rheumatic disease and an impressive survival of over 15 years with a severely dysfunctional tricuspid prosthesis. Later in life, she developed severe degenerative AS and, due to high surgical risk, became a candidate for TAVI, the treatment of choice for severe symptomatic AS in patients who are unsuitable for conventional surgery.[7]
Although timely surgery or catheter-based treatment is ideally needed for symptomatic severe valvular disease, such options may be limited, particularly in developing countries. Consequently, medical management is often the only initial option available, targeting the consequences of valvular regurgitation or stenosis, such as heart failure and atrial fibrillation (AFib).[3] Throughout her long medical journey, our patient endured numerous hospitalizations for decompensated heart failure, with diuretic therapy serving as the mainstay of her management.
Survival free from complications is lower after valve replacement with either mechanical or biological prostheses, due to higher rates of valve thrombosis and thromboembolism in the former and a faster degenerative process in the latter.[6,8] Our patient’s evolution was marked by multiple complications following each intervention, experiencing almost every form of prosthesis dysfunction, both-early and late, including patient-prosthesis mismatch, pannus formation and thrombosis. Given the predisposition to thrombosis despite proper anticoagulation and the presence of chronic anemia, a potential neoplastic condition was also considered in this case. A thorough evaluation, including abdominal, pelvic and thoracic computed tomography scans, along with endoscopy and colonoscopy, was performed, ruling out any neoplastic disease as well as any sources of active bleeding. Chronic kidney disease and a mild degree of hemolysis associated with mechanical prostheses were considered as contributing factors to the anemic syndrome.
Anticoagulation is often indicated in RHD, either for patients with mechanical heart valves or for those with RHD-related valvular AFib. However, the need for frequent INR testing can make compliance with VKAs problematic in developing countries.[4] While an anticoagulant that does not require monitoring would be highly beneficial in low- and middle-income countries, where most patients with RHD reside, it is well known that non-vitamin K oral anticoagulants (NOACs) have been found to be suboptimal for these patients and are therefore not recommended by major guidelines for use with mechanical valve prostheses. Vitamin K antagonists remain the oral anticoagulant of choice for patients with significant rheumatic mitral stenosis and AFib.[3]
The INVICTUS trial compared VKAs with rivaroxaban in patients with AFib predominantly due to hemodynamically significant rheumatic mitral stenosis. The results showed that VKA therapy led to a lower rate of a composite of cardiovascular events or death compared to rivaroxaban therapy, without an increased rate of bleeding.[9] In our patient, hemorrhagic complications represented a major issue following each procedure, not due to poor monitoring or non-compliance, but rather because of associated liver cirrhosis with mixed-etiology (chronic HCV infection and chronic liver congestion) leading to lability of the INR and a significant predisposition to bleeding.
Additionally, the coexistence of conduction disorders has led to a new series of complications. The need for permanent cardiac pacing raised technical challenges, particularly considering the presence of the mechanical prosthesis in the tricuspid position. In such cases, alternative options include epicardial lead implantation or, as a less invasive approach, left ventricular pacing via a branch of the coronary sinus.[10] Given the technical challenges and prohibitive hemorrhagic risks associated with major surgical intervention for epicardial lead implantation, the team decided to implant a new pacing lead in a branch of the coronary sinus when the first device became dysfunctional, rather than explanting the initial lead. Consequently, maintaining both pacing systems in situ resulted in a unique situation characterized by functional interference between the two devices and recurrence of presyncopes.
This case illustrates the continuum of RHD and highlights the attention that must be given throughout the disease’s life course to facilitate optimal management in affected populations. It also emphasizes the unique challenges that may arise, which can often make management extremely difficult.