Atherosclerosis represents the primary mechanism involved in cardiovascular diseases’ morbidity and mortality through a progressive systemic inflammatory process.[1] In this manner, the patients are exposed to an increased risk of developing atherosclerosis in multiple vascular territories, and targeted, individualized management is required. Coronary and carotid arteries are two major affected vascular territories, and their association with the atherosclerotic process has increased incidence and a major influence on quality of life, making them a common clinical scenario.[2] This paper emphasizes the importance of screening for atherosclerosis burden in other vascular territories in patients with severe coronary atherosclerotic disease.
We present a case of a 58-year-old male, a former smoker, who was elective admitted for moderate exertion dyspnea and mild vertigo when changing position from supine to standing upright. The patient denied any relevant hereditary history of cardiovascular disease but with the presence of multiple cardiovascular risk factors: hypertension (HTN), type 2 diabetes mellitus (T2DM), and dyslipidemia. Grade 3 arterial hypertension with very high cardiovascular risk was noticed for almost 20 years, affirmative with controlled blood pressure values at home. Eight years before the admission, a diagnosis of T2DM was confirmed, and the patient was started on an oral hypoglycemic regimen (Metformin+Glibenclamide). At admission, high basal glycemic values and a glycated hemoglobin value of 7.72% were exposed, and a diabetologist’s advice was considered to obtain adequate glycemic control.
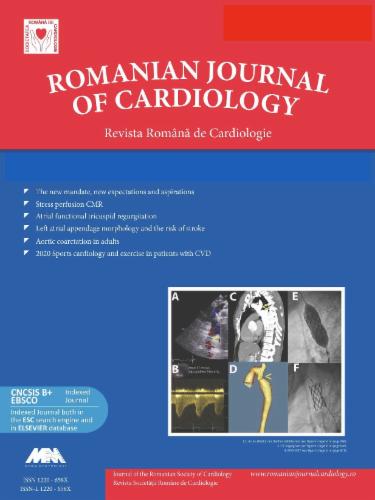
Additionally, the patient experienced multiple cardiovascular events in his personal history. An inferior myocardial infarction (MI), as the first manifest cardiovascular major event, was diagnosed incidentally in 2020 during a coronary angiogram for CCS IV angina. At that time, triple vessel disease (insignificantly left main stenosis, significant left anterior descending coronary artery-LAD, circumflex artery-LCx stenosis, and occlusion of right coronary artery-RCA) was documented (Figure 1). Percutaneous coronary intervention (PCI) for RCA was not successful, but two drug-eluting stents (Orsiro 2.75/18 mm and Xience ProA 2.5/38 mm, respectively) were implanted in the LAD at that time.
First diagnostic coronary angiogram (December 2020). Panel A: In LAO caudal view, an intermediate left main coronary artery stenosis, and significant lesions of LAD, LCx and OM are depicted. LAD - left anterior descending artery, LCx - left circumflex artery, LAO - left anterior oblique, LMCA - left main coronary artery, OM - obtuse marginal artery, PDA - posterior descending artery, RCA - right coronary artery.
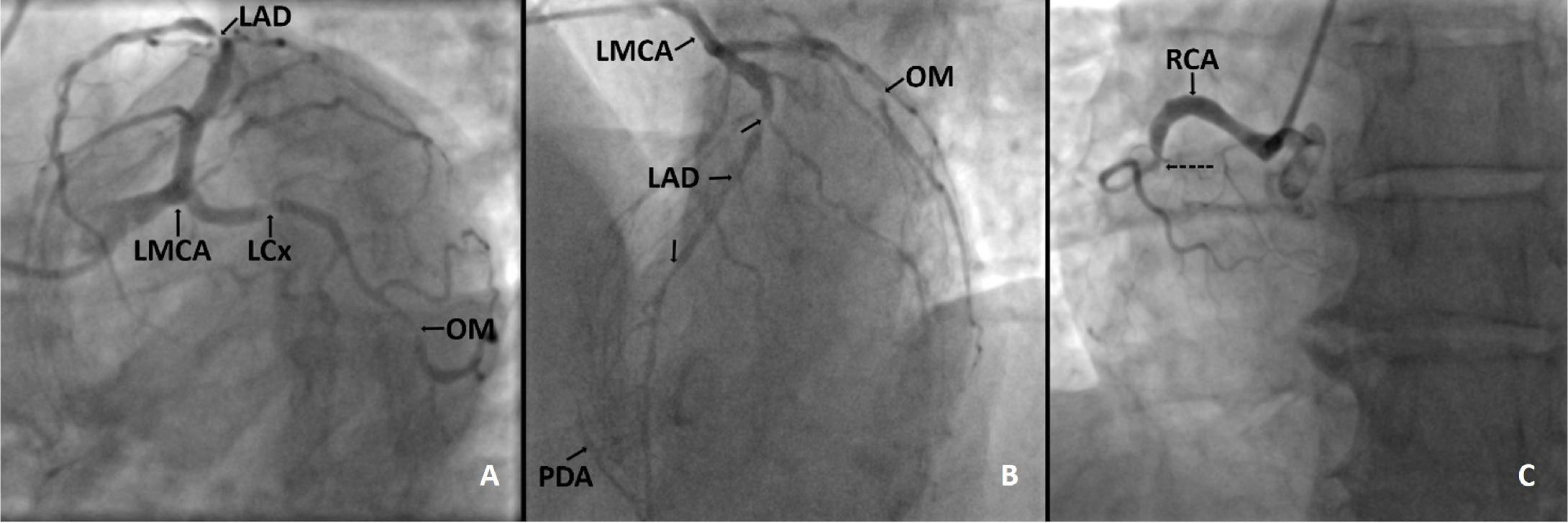
After one year, a second coronary angiography was scheduled due to worsening angina, and the significant stenosis of LCx was treated with an Onyx™ 2.5/30 mm stent. A third PCI (2023) targeted the significant LAD medial segment, completed with stent implantation (Orsiro™ 2.75/30 mm) (Figure 2 panels A-D). Complete surgical revascularization was not considered at any time, as the patient declined it in the first place.
Staged percutaneous coronary interventions performed on LAD and LCx. Panel A: Angiographic results after stents implantation performed in December 2020 in proximal-mid segment and distal part of LAD (continuous arrows). The lesion in the mid-part of LAD (dotted arrow) was considered intermediate at that time (LAO cranial view). Panel B: The results of PCI completed in March 2021 with stent implantation in the OM (RAO caudal view). Panel C illustrate the progression of the lesion in the mid segment of LAD (arrow) and the angiographic finał result after stent implantation in March 2023 is outlined in panel D respectively (arrow). LAD - left anterior descending artery, LCx - left circumflex artery, LAO - left anterior oblique, LMCA - left main coronary artery, OM - obtuse marginal artery, PDA - posterior descending artery.
The patient was admitted for cardiovascular reevaluation one year after the last coronary angioplasty was done. At the time of admission, the patient was hemodynamically stable. Physical exam revealed normal lung sounds, no pulmonary rales, rhythmic heart sounds without murmurs, blood pressure of 115/80mmHg, and heart rate of 70 beats per minute without femoral or carotid bruits.
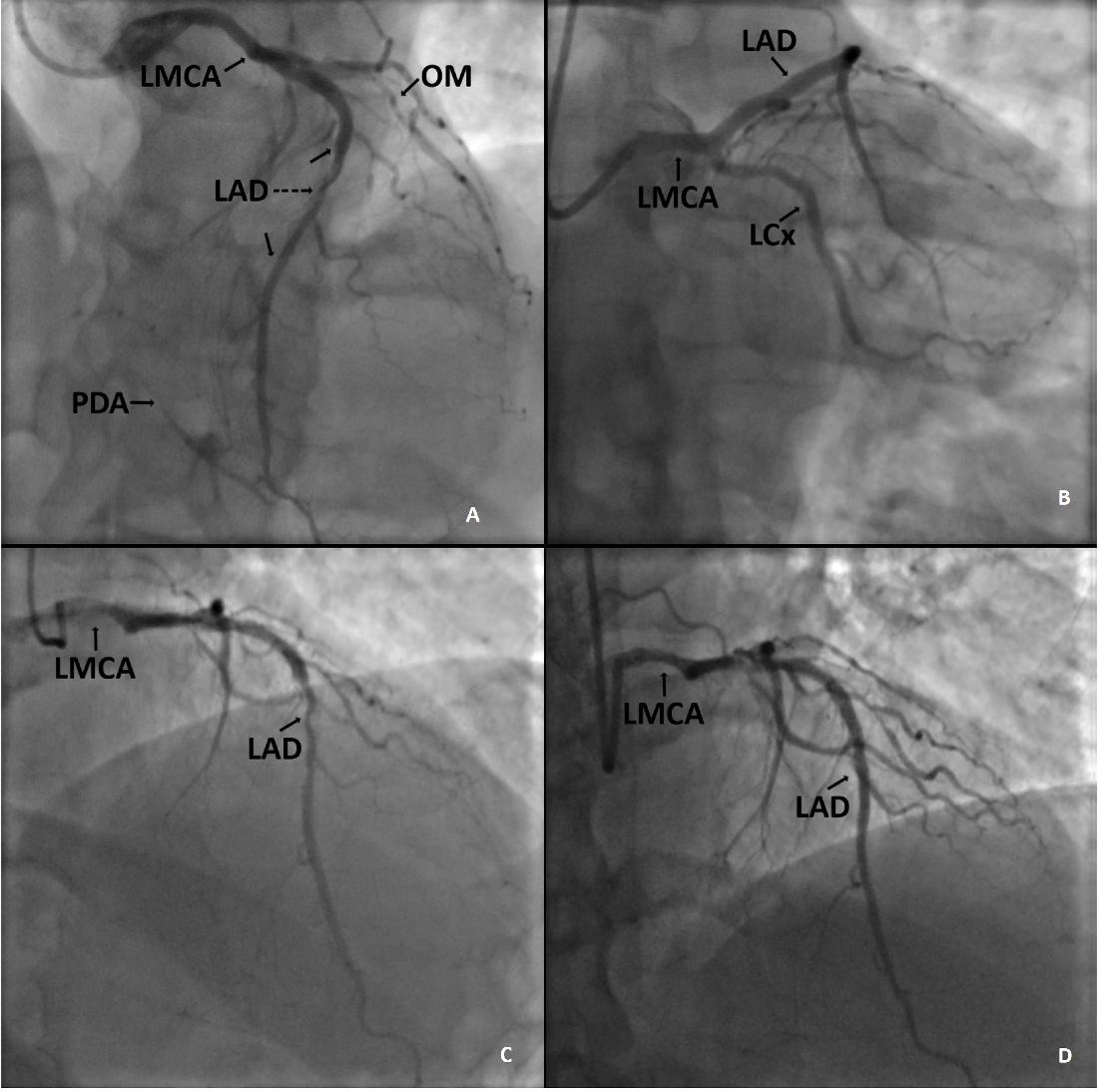
The electrocardiogram (ECG, BTL-08 Plus machine, BTL Industries, Hertfordshire, UK) outlined sinus rhythm, intermediate QRS axis, and inferior MI sequelae with Q waves in DII, DIII, and aVF leads. Bidimensional standard echocardiography (GE Vivid™ E9 ultrasound system, 1.5-4.5 MHz probe, GE Healthcare, Boston, MA, USA) showed a moderate reduced ejection fraction of the left ventricle (LVEF 48%, Simpson’s biplane method) due to akinesia of the inferior wall, mild tricuspid, and mitral regurgitation, without pericardial effusion. When the left ventricular Global Longitudinal Strain (GLS-LV) was evaluated, an average value of -16.9% and hypo-contractility of the inferior wall and basal antero-septal segment were identified. (Figure 3)
The global longitudinal strain of the left ventricle performed one year after the last PCI. The results are normal (-20.0%) in A4C view, and subtle disturbances in LAX view (- 16.9%), A2C view (-13.9%), but the mean value of -16.9% of GLS-LV are conclusive for altered longitudinal contraction of the myocardium. A2C - apical 2 chambers, A4C - apical 4 chambers, GLS-LS - global longitudinal strain of the left ventricle, LAX - long-axis, PCI - percutaneous coronary intervention.
During hospitalization, a routine Duplex ultrasound imaging of carotid and lower limb arteries was completed using a 2.4-10 MHz linear array probe (GE Vivid™ E9 ultrasound system, GE Healthcare, Boston, MA, USA), and ≥ 90% bilateral carotid artery stenosis were exposed (ulcerative plaques, filiform flux through the lesion, velocities of 518 cm/s on the right side and 320 cm/s on the left side, respectively). A computed tomography angiography (CTA, Somatom Definition AS™ 512-slice scanner Siemens Healthcare GmbH, Erlangen, Germany) was performed to evaluate the supra-aortic and bilateral carotid lesions and to decide the therapeutic approach. Postprocessing scans confirmed the bilateral severe stenosis with alternating stable and unstable atherosclerotic plaques. (Figure 4, 5)
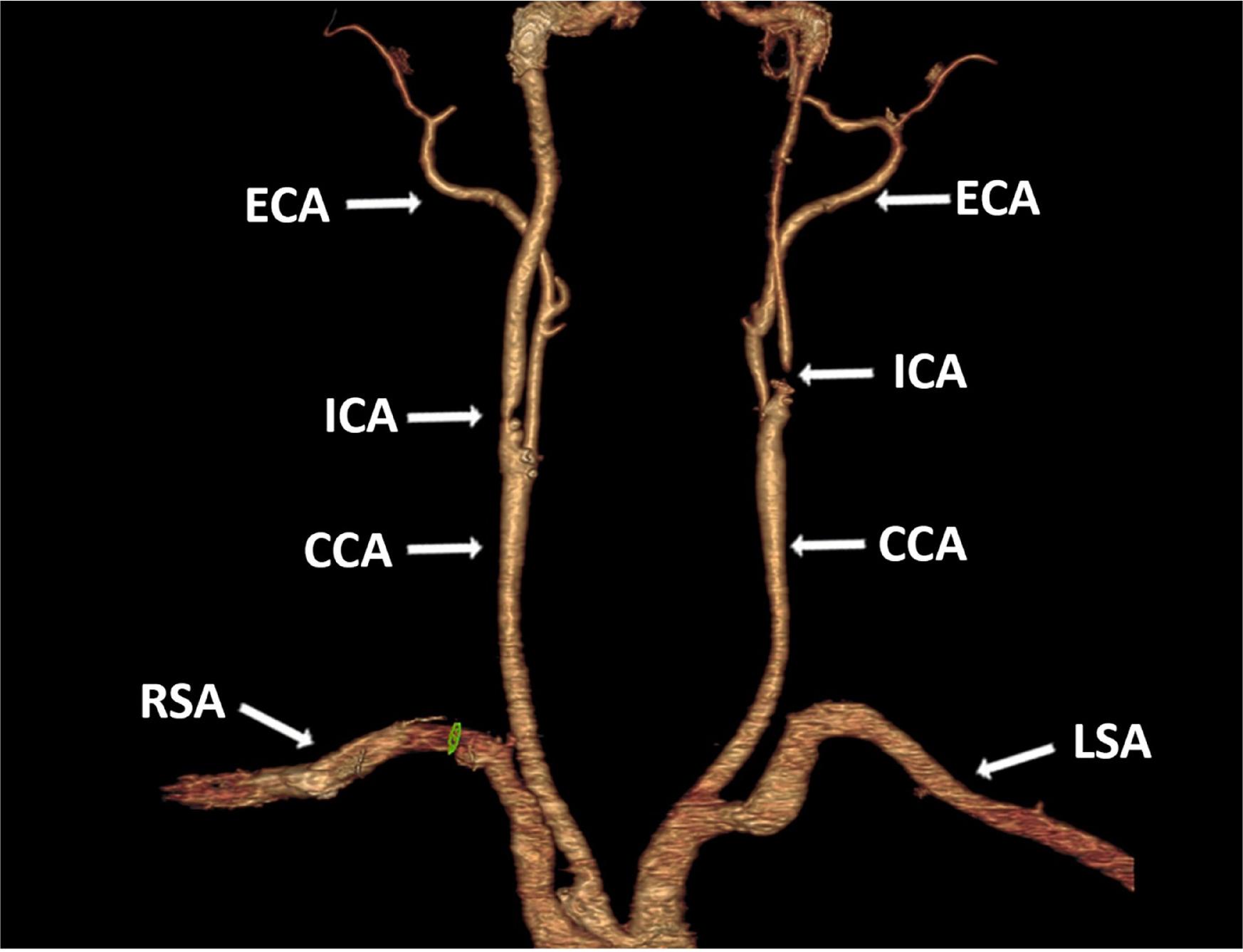
Three dimensional reconstruction of the supraortic arteries. Severe stenosis of bilateral ICA are depicted. No significant stenosis involving bilateral CCA, ECA, LSA and RSA were identified. ICA - intemal carotid artery, CCA - common carotid artery, ECA - extemal carotid artery, LSA - left subclavian artery, RSA - right subclavian artery.
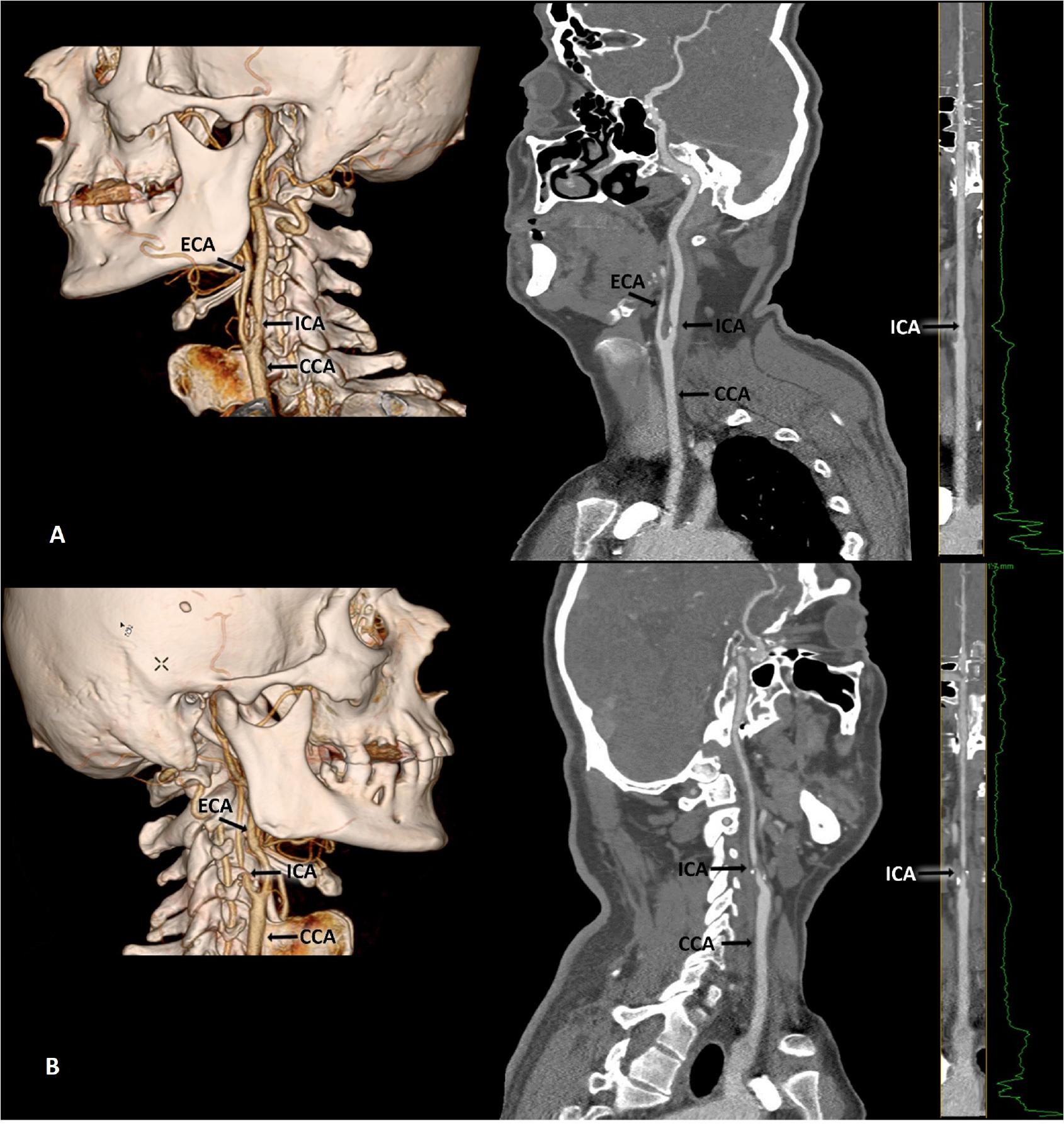
Three dimensional and sagittal multiplanar reconstructions confirmed the severity of left ICA (panel A) and right ICA respectively (panel B). ICA-internal carotid artery, CCA-common carotid artery, ECA-external carotid artery.
Non-invasive screening (ankle-brachial index, Doppler ultrasound) for lower extremity arterial disease was negative.
The pharmacological approach consisted of a double antiplatelet regimen (Aspirin 100mg o.d.+Clopidogrel 75mg o.d.), angiotensin-converting enzyme inhibitor (Ramipril 2.5mg b.i.d.), beta-blocker (Bisoprolol 2.5mg b.i.d), dihydropyridine calcium channel blocker (Amlodipine 5mg o.d), fixed-dose combination of Spironolactone 50mg+Furosemide 20mg o.d., and high-intensity statin (Atorvastatin 80mg o.d). At the same time, glycemic control was achieved with an SGLT2 inhibitor (Dapagliflozin 10mg o.d.) and a combination of a biguanide and a second-generation sulfonylurea (Metformin 400mg+Glibenclamid 2.5mg b.i.d).
In line with current recommendations related to the proper management of extracranial cerebrovascular disease, the conjoined decision of the heart team (clinical cardiologist, interventional cardiologist, vascular surgeon, and anesthesiologist), staged bilateral carotid endarterectomy (CEA) should be pursued over transfemoral-carotid artery stenting (TF-CAS). A pre-operative neurological consult was done, including a Doppler ultrasound that confirmed the severe stenosis. Within one week after CTA was performed in April 2024, according to the recommendations of the neurologist, and considering preventing possible future cerebrovascular events on the left-dominant side cerebral hemisphere, the patient underwent a first unilateral standard left carotid endarterectomy, with selective shunt and primary suture, even though the right-side stenosis was more severe. Surgery was successful, and no perioperative or shortterm postoperative complications (hypotension, wound hematoma, ipsilateral ischemic stroke, carotid thrombosis, transient vagus, hypoglossal, and/or glossopharyngeal nerve injuries or dysphagia) were noticed. The case was scheduled within 30 days for a second CEA addressed to the right carotid artery, according to the recommendations of the vascular surgeon.
This paper emphasizes the importance of extensive screening of vascular lesions in patients with multiple aggregate cardiovascular risk factors and a history of defined acute cardiovascular events. The presence of severe coronary artery disease is a hallmark of aggressive and advanced systemic atherosclerosis. A further important aspect of this case report underlines the concomitant and diffuse development of atherosclerosis in multiple arterial territories, from which the coronary and carotid systems significantly impact prognosis and quality of life.[3] In some cases, the adaptive capacity and hemodynamic particularities of the cerebral blood flow led to asymptomatic clinical pictures, which can conceal or diminish the symptoms even in severe cases, like the above-presented case. Accordingly to Duraiswamy et al., statistical analyses granted an incidence of approximately 36% of asymptomatic cases among the ones diagnosed with uni- or bilateral carotid stenosis.[4] Onur-Beyaz et al., in a large cohort of patients who underwent screening for carotid artery disease by Duplex ultrasound, reported an incidence of 3.1% for greater than 70% carotid stenosis in the general population with at least one cardiovascular risk factor.[5]
In a group of 63 patients diagnosed with coronary artery disease, Shenouda et al. disclosed that among the main cardiovascular risk factors, HTN is strongly correlated with carotid calcifications, whereas T2DM and dyslipidemia were associated with a higher risk of coronary atherosclerosis.[6] In our case, two main risk factors (HTN and dyslipidemia) were present for the last 20 years, and T2DM was confirmed four years before the first major cardiovascular event. The atherosclerotic process was described as concomitant in carotid and coronary systems in a relatively modest cohort of 50 patients presenting with ST-segment elevation myocardial infarction (STEMI), compared with the same number of 50 cases of stable coronary artery disease by LeBlanc et al. in 2017. However, it was greater in the carotid arteries of new-onset acute STEMI without a previous history of chronic coronary syndrome.[7]
The magnitude of the atherosclerotic burden diagnosed in this case was inconsistent with the clinical presentation, and the lack of symptoms was challenging for diagnosis and management. According to the European Society of Cardiology (ESC) guidelines, surgical endarterectomy and carotid stenting are the main therapeutic options for revascularizing carotid artery disease.[8] The European Society for Vascular Surgery guidelines recommend that in asymptomatic patients, feasible for CEA, life expectancy of more than five years, and more than one feature suggesting a higher stroke risk, surgery should be considered (class IIa B indication) in comparison with CAS (class IIb B recommendation), alongside withthe best medical treatment.[9] It has been demonstrated that in young patients, even in asymptomatic cases, CEA reduced the 10-year stroke risk with beneficial effects on the patient’s life.[10]
Although the risk of fatal events is similar between CEA and CAS, the risk of non-fatal events is higher with CAS than CEA.[11] The presented report identified no high-risk criteria for endarterectomy; therefore, the decision was directed toward CEA. A meta-analysis of four studies regarding staged or synchronous carotid artery stenting revealed an increased risk of stroke at 30 days post-procedure in the case of the simultaneous revascularization approach. However, the long-term endpoint did not differ between the two clinical situations.[12] Furthermore, it was proved that early second-stage endarterectomy has a higher rate of complications compared to a delayed one of more than 30 days.[13] The strategy of staged CEA was also supported by the high risk of developing hyperperfusion syndrome, described in the literature as one of the most serious complications of revascularization methods for internal carotid artery stenosis caused by a severe decrease in cerebrovascular reactivity due to inadequate collateral blood flow.[14]
The COMPASS trial showed a real benefit of the combined treatment with Aspirin (100 mg o.d.) and low dose Rivaroxaban (2.5 mg b.i.d) in patients with coronary artery disease and peripheral artery disease, without an increase in bleeding risk. Nevertheless, a double antiplatelet therapy (DAPT with Aspirin 100 mg o.d. plus Clopidogrel 75 mg o.d) was recommended due to risk factors listed in the ESC 2023 guideline for the acute coronary syndrome (T2DM, plurivascular disease, at least three stents implanted and total length stent over 60 mm).[15,16]
Even though it may seem aimless to perform carotid artery screening in asymptomatic patients, some cases, such as the one presented above, may reveal unexpected results, and patients could be at increased risk of cerebrovascular events. Furthermore, we consider that the screening of other vascular territories is mandatory in patients with previously extensive coronary artery disease and significant risk factors. Staged CEA, by the side of the best medical treatment, may be the first-line choice for this patient phenotype. A structured screening program for carotid and peripheral artery disease should be popularized to prevent the extension of atherosclerotic burden in patients with established CAD. Well-designed targeted clinical trials on large cohorts of patients are necessary to define rigorous diagnostic algorithms and precise management based on distinct clinical protocols, including comprehensive preprocedural neurologic evaluation.