A stuck leaflet is a rare complication of transcatheter aortic valve implantation (TAVI). It consists of a leaflet with absent or reduced motion after the valve implantation in the aortic annulus. This can provoke dramatic changes in the patient’s hemodynamics and progress rapidly into worsening and eventually life-threatening hypotension that requires cardiopulmonary resuscitation to be managed.
Generally, leaflet malfunction presents in one of the three leaflets, although involvement of all valve leaflets has been described. The cases defined in the literature were treated by placing a second device in the seat of the non-functioning valve (valve-in-valve, ViV) (1,3).
An 83 year old woman with effort angina and dyspnea was referred to our cardiology department and diagnosed with severe aortic valve stenosis.
She also suffers from ischemic cardiopathy treated with previous percutaneous coronary intervention, paroxysmal atrial fibrillation, hypertension, diabetes mellitus, and peripheral arteriopathy.
A complete instrumental assessment was performed, with an echocardiogram demonstrating severe aortic stenosis with mean pressure gradient of 50 mmHg and valve area less than 1 cm2.
At the direction of the Heart Team, the patient was scheduled for transcatheter aortic valve implantation.
A complete assessment of the arterial routes and aortic valve was performed with a computed tomography scan, as usual in our institution. The valve showed asymmetrical distribution of calcium with a greater degree of calcification on the left and non-coronary cusp (Fig 1-2).
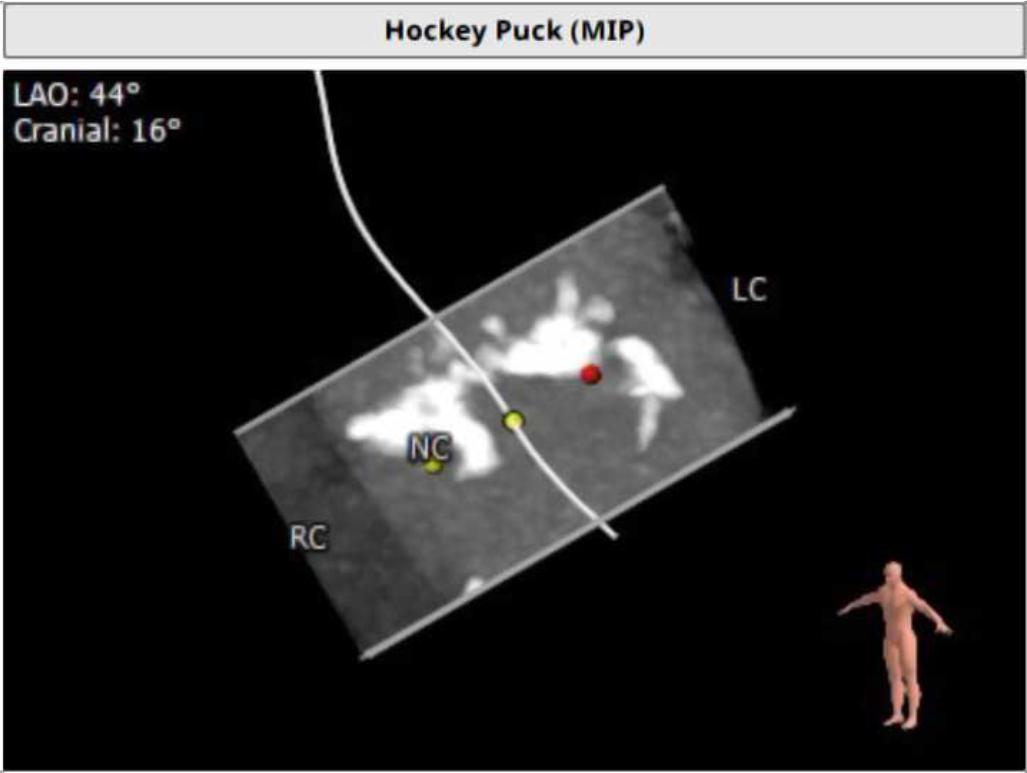
Hockey puck view that enhances aortic valve calcifications.
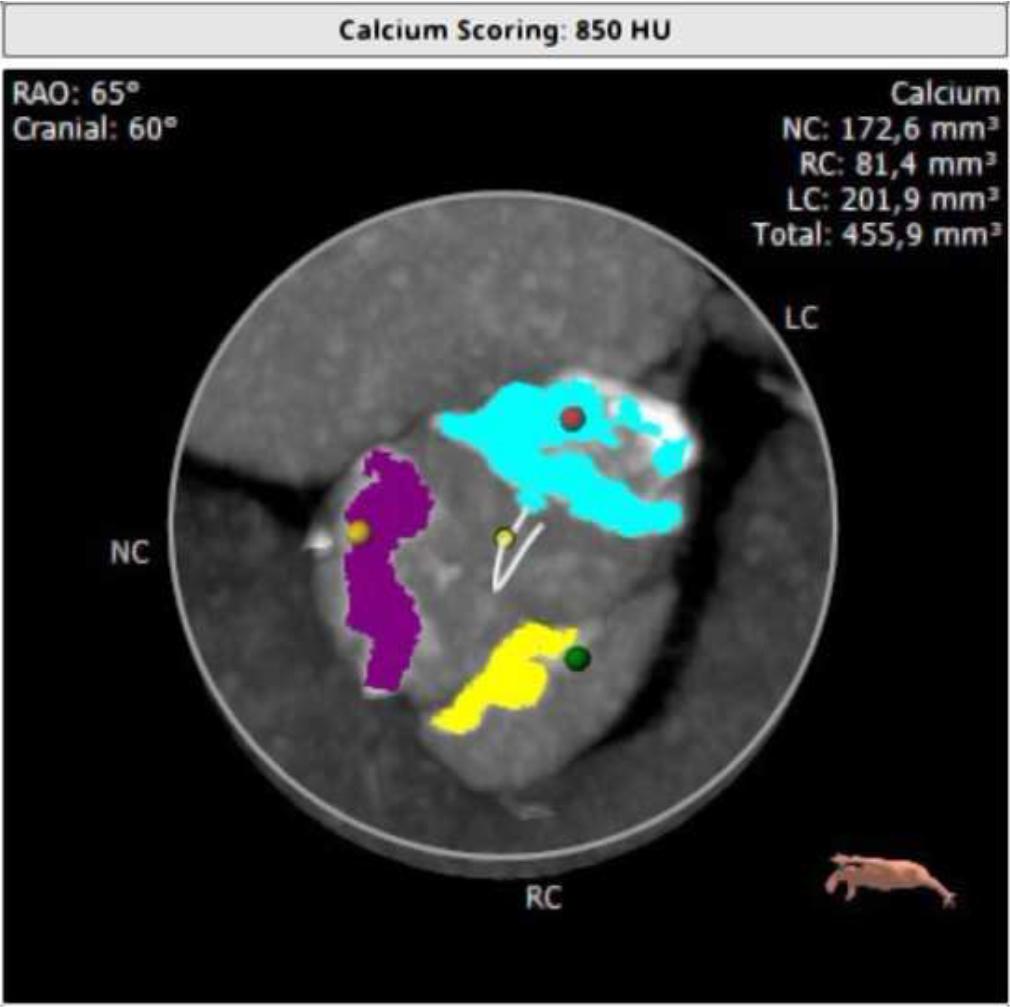
Distribution of aortic valve calcification with volume quantification (3mensio evaluation on contrast-enhanced CT). The total calcium volume was 455.9 mm3 using a threshold of 850 HU, with prevalence of calcium on left coronary cusp (201.9 mm3) and noncoronary cusp (172.6 mm3).
The CT analysis showed an aortic virtual basal ring with the following measures: max diameter 26 mm, min diameter 20 mm, perimeter 71.4 mm, derived perimeter 22.7 mm.
The procedure was performed with conscious sedation. Using right femoral access, pre-dilation was performed using a VACSIII 20/40 balloon, followed by the implantation of a Portico™ valve (25 mm) with an implantation depth of 9 mm (non-coronary cusp) and 8.44 mm (left coronary cusp). The cover index was 8%, not indicating less oversizing. After the release of the device, there was evidence of severe intraprosthetic regurgitation (Fig. 2, Video 1).
Transesophageal echocardiography (TEE) depicted a severe malfunction of the cusp facing the right coronary Valsalva sinus, manifested as severe hypomobility (Fig. 3, Video 2). Since the patient remained hemodynamically stable, it was not necessary to use inotropes and vasoconstrictors, to practice cardiopulmonary resuscitation or to institute extracorporeal circulation.
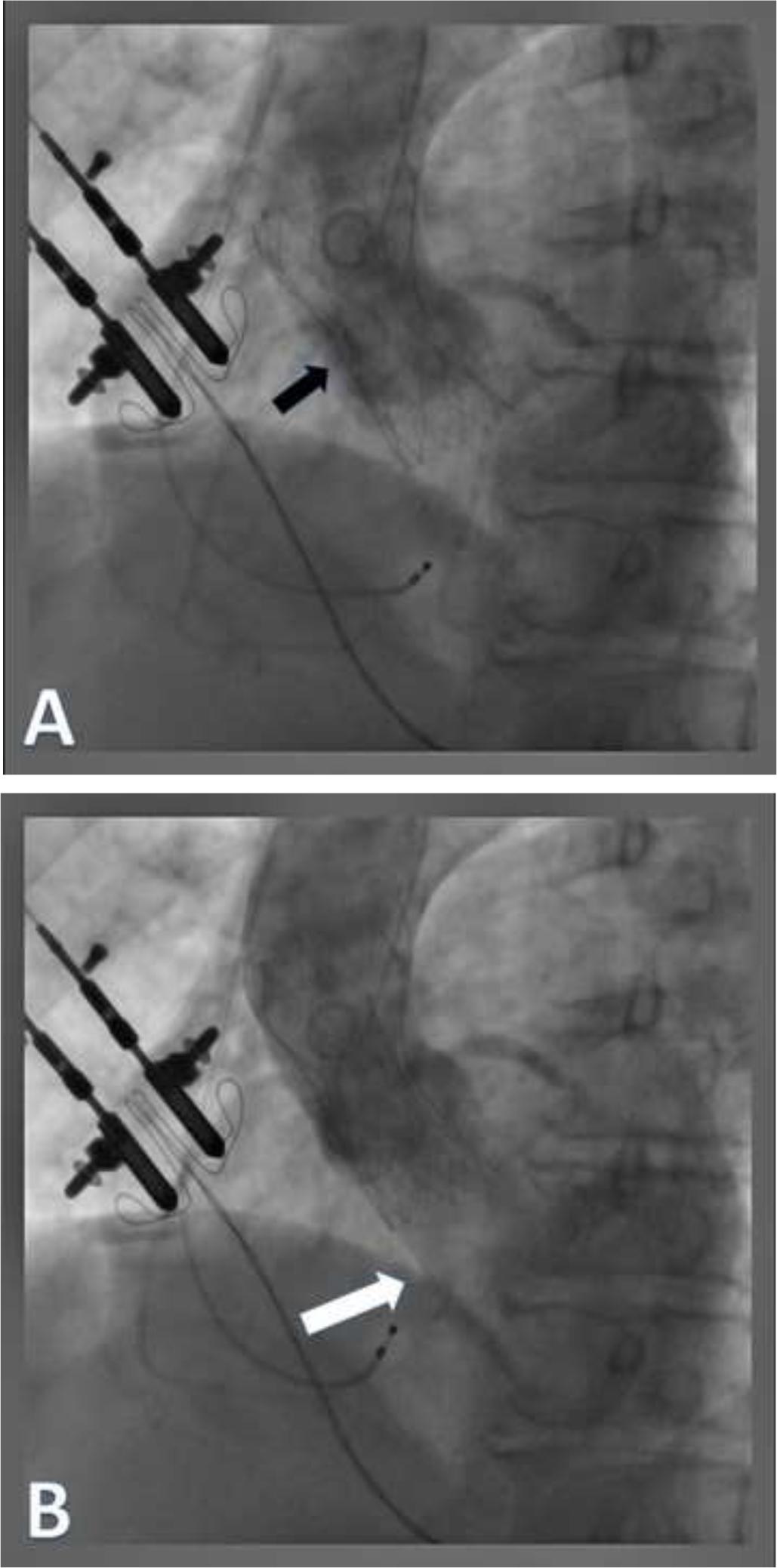
Angiographic view after implantation of Portico aortic valve bioprosthesis (black arrow). A: Systolic frame. B: Diastolic frame showing severe (grade 4) central aortic regurgitation (white arrow).
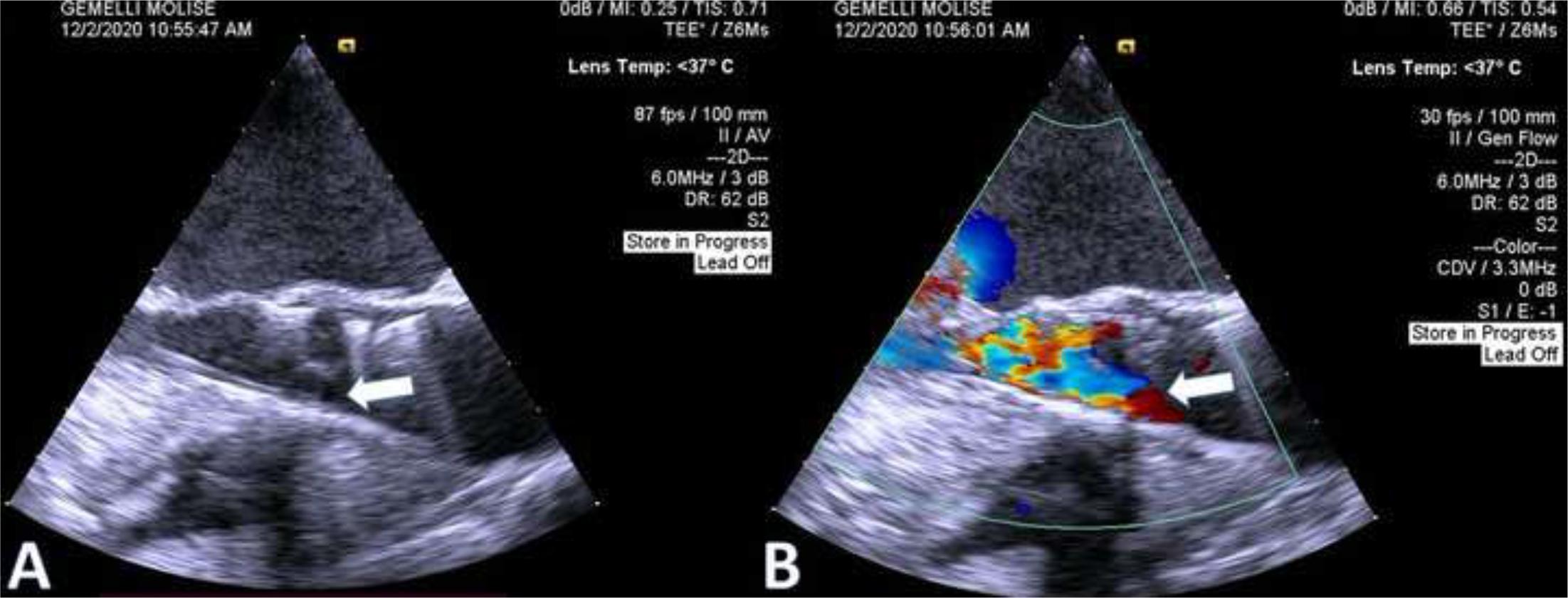
Transesophageal echocardiography LVOT view. A: 2D echo showing stuck leaflet (leaflet not visible in picture, white arrow) in anterior position. B: 2D color showing severe intraprosthetic regurgitation.
Several ineffective attempts were made by manipulating coronary and pigtail catheters to restore the leaflet’s mobility.
The procedure was therefore optimized with a two post-dilatation with VACSIII 20/40 balloon and finally with cusp mobilization. At the end, the TEE check showed absence of intraprosthetic regurgitation and only mild posterior periprosthetic leak (Video 3). Therefore, it was not necessary to place a second prosthetic valve in place of the first one.
The post-operative course was regular, and the patient continued her cardiological follow-up, remaining stably asymptomatic.
In this paper, we describe a rare case of a stuck “open” leaflet after TAVI resolved by ballooning procedure, with no need for another valve implantation.
Few other sporadic cases of frozen leaflets have been described, in most cases affecting a single leaflet of a balloon-expandable valve (BEV). Okuyama et al. described a case in which all three leaflets were simultaneously stuck just after post-dilatation. The reason why this happens is not clear. Possible explanations, apart from an unsuccessful deployment of the valve inside the aortic annulus (1), can lie in the trapping of the transcatheter aortic valve leaflet by the native calcified valve leaflet; otherwise, the problem is in the preparation of the valve itself. In fact, prosthetic valves are crimped as tight as possible to allow an easier passage of the device through the sheath. This extremely tight crimping may alter the structure of the valve, preventing one leaflet from opening adequately once the valve is released (2,4).
The treatment of this frightening complication consists of hemodynamic support, an attempt at manipulation with a catheter, and the insertion of a second prosthesis within the first valve.
The several other reported cases of frozen leaflets were all treated with deployment of a second valve (ViV) with prompt restoring of an adequate function of the prosthetic device.
In our case we have described a singular case (described for the first time, to our knowledge) of a frozen leaflet in a self-expandable valve (SEV), resolved not with ViV procedure, but with balloon postdilatation. In this case, valve under-expansion could be another reason for this complication; indeed, asymmetric expansion of the valve stent could lead to unfavorable closing forces on the stuck open leaflet. We think that balloon post-dilation was effective in resolving this frightening complication.
A prompt diagnosis of a frozen leaflet is crucial to treat a rare but severe complication of the TAVI procedure and ensure a good outcome for the patient. In addition to ensuring the necessary hemodynamic support, an attempt to mobilize the stuck leaflet with a balloon should always be performed, as long as it does not delay the preparation of the second valve to be implanted immediately if a satisfactory angiographic result has not been obtained.
In conclusion, doctors should be aware of rare but severe complications in the course of TAVI, such as root rupture and stuck leaflets, when performing the procedure and providing care afterward.