Cardiovascular diseases remain the leading cause of mortality worldwide, with coronary artery disease (CAD) being a major contributor.[1] Despite the significant improvements in cardiovascular primary prevention strategies from the last decades, CAD is still responsible for 38% of female and 44% of male cases, with an annual incidence of 5.8 million new cases estimated overall in European countries.[2] Therefore, early and accurate detection of CAD is crucial for effective management and prevention of adverse cardiovascular outcomes. Coronary computed tomography angiography (CCTA) has emerged as a pivotal non-invasive imaging modality for detailed assessment of coronary anatomy and plaque characteristics, playing a significant role in diagnosing and managing ischemic heart disease (IHD).
Traditionally, there are several non-invasive cardiovascular imaging methods for diagnosing and prognostic stratification IHD, including stress echocardiography, single photon emission computed tomography (SPECT), or stress magnetic resonance imaging (MRI). However, with the advent of CCTA, it is now possible to identify and quantify non-obstructive coronary plaque or to intercept an earlier stage of the disease.[3] In this regard, several recent trials, including the SCOT-HEART trial and the PROMISE trial, emphasized how patients in whom non-obstructive coronary disease was documented had the same risk of developing distant acute myocardial infarction as patients with obstructive coronary disease.[4,5] In fact, CCTA can be considered the only non-invasive imaging method capable of characterizing the coronary plaque responsible for both myocardial infarction and chronic coronary syndromes.[6]
In the context of acute coronary syndromes (ACS), CCTA is currently indicated in the evaluation of patients presenting to the emergency room with chest pain at a low-intermediate risk of CAD. [7] In particular, the most recent European guidelines limit the use of CCTA if the high-sensitive cardiac troponin dosage is negative or uncertain, if there are no dynamic changes in the electrocardiogram tracing, and if there is no recurrence of chest pain.[8]
On the contrary, CCTA has a consolidated use as a first-line diagnostic test in the evaluation of symptomatic patients for typical or atypical angina in the suspicion of chronic coronary syndrome, with class I indication.[9] In particular, concerning the ability to identify obstructive stenoses compared to the gold-standard invasive evaluation by coronary angiography, CCTA has demonstrated a sensitivity between 85% and 95% in several multicenter trials and a negative predictive value close to 100%.[10,11,12]
In recent years, thanks to the new, modern technologies available, a paradigm shift has led to an increasingly extensive use of CCTA in evaluating patients with suspected IHD. Table 3 summarizes the key conclusions of major trials evaluating the role of CCTA in cardiovascular risk assessment.
Whereas the 2019 ESC Guideline for the Management of Chronic Coronary Syndrome (CCS) recommended CCTA as the preferred strategy for patients with a low clinical likelihood of CCS and no prior history of CAD, the updated 2024 ESC Guidelines for CCS broadened the indication to include patients with a low to moderate pre-test likelihood of CAD.[9] However, the new guidelines kept its contraindication of not performing CCTA when there is a fast, irregular heart rate, extreme obesity, or any condition that makes obtaining good image quality unlikely.[9]
The latest National Institute for Health and Care Excellence (NICE) guidelines update reflects this change. CCTA is recommended for the initial evaluation of all patients with typical and atypical angina regardless of pre-test probability. In contrast, stress imaging is recommended only if the identified coronary lesions have ambiguous functional significance.[13] Furthermore, the 2021 American guidelines on the evaluation of chest pain sets CCTA and functional tests on the same level of evidence for patients with intermediate-high pretest risk of CAD. It is recommended to choose between the two methods based on the patient’s age (i.e. in the case of age < 65 years, the CCTA is better, while in the case of age ≥ 65 years, the functional tests are preferred).14 Moreover, a recent study highlighted the use of CCTA as a cost-effective method for coronary allograft vasculopathy surveillance in patients with cardiac transplantation, outperforming the traditional invasive coronary angiography in terms of logistical and economic burden.[15]
Recent data have shown that there is no significant difference in the long-term risk of major adverse cardiovascular events (MACE) between patients with chronic coronary syndrome who undergo non-invasive coronary evaluation via CCTA and those undergoing invasive coronary angiography.[16] Consequently, the endorsement of CCTA for evaluating coronary anatomy is further supported by a lower incidence of major procedure-related complications associated with an initial CCTA-based strategy.[16]
Technological advancements enabling the acquisition of high-resolution images and the development of new, precise, and faster post-processing techniques have recently expanded the application of CCTA, from assessing the degree of stenosis to analyzing coronary plaque.[17]
This review summarizes the latest evidence on plaque analysis using CCTA, from identifying high-risk features to advanced automated quantification techniques, and discusses their clinical and prognostic implications for guiding treatment decisions.
In clinical practice, computer tomography (CT) scanners feature rotating gantry housing detector arrays and X-ray tubes. Essential components include a motorized scanner table, a synchronization ECG system, and a rapid contrast injection system.[18] A collimator directs the X-ray beam to enhance image resolution and reduce patient radiation exposure. Modern CT scanners use a “multislice” technique to capture multiple sections along the z-axis per rotation, enabling fast data acquisition and high spatial resolution. “Dual-energy” CT scanners improve temporal resolution with two X-ray sources and detectors.[19] Images are reconstructed with algorithms assigning Hounsfield Unit (HU) values to each pixel, showing tissue attenuation. Multiplanar reconstructions (MPRs) offer 3D views of coronary vessels for detailed analysis of anatomy, stenosis, and plaque composition.[20]
In recent years, there has been a growing technological development to implement the degree of spatial resolution in CT, up to resolution ranges of 0.150-0.200 mm.[21] However, ultra-high spatial resolution (UHR) CT imaging techniques are more susceptible to motion artifacts and exhibit increased image noise. [22] Despite these limitations, UHR CT provides several advantages, such as an improved definition of heavily calcified segments that are small in diameter or contain previous stents. Furthermore, it can offer a better morphological characterization of the coronary plaque than traditional CT, with a higher resolution than other non-invasive methods.[22] Plaque characterization still presents some limitations, including considerable variability of results between observers and between qualified observers and automatic methods, so using high-resolution methods could reduce variability between observers and favor automatic tools in recognition of the coronary contours. [23] Furthermore, changes in the pathophysiological process of atherosclerosis occur in the morphology and formation of coronary plaque below the spatial resolution of traditional CT methods.[24] Therefore, UHR CT could be valuable for the ongoing monitoring of plaque reduction in patients undergoing treatment with lipid-lowering drugs.
Over the years, various methods have been developed to quantify the burden of atherosclerotic plaques.[25,26,27] Pioneering approaches in coronary artery stenosis assessment often employ semi-quantitative methods, which estimate the plaque burden (Table 1). These techniques circumvent the need for coronary vessel segmentation, offering either a straightforward cumulative stenosis evaluation or, in more advanced forms, incorporating plaque location and composition. These methods are (1) the Segment Stenosis Score (SSS), which provides that each coronary segment is assigned a value from 0 to 5 based on the severity of the stenosis. These values are subsequently added to obtain a final value;[25] (2) the Segment Involvement Score (SIS), which provides that each segment is assigned a value from 0 to 1 on the presence or absence of coronary plaque. These values are then added together;[25] (3) the Leaman score, which takes into consideration various elements, including the location of the plaque, the type of plaque (calcified or non-calcified), and the degree of stenosis.[26,27]
The advantages and limitations of the current cardiac computed tomography methods for assessing coronary artery plaque burden.
| CT method | Description | Advantages | Limitations |
|---|---|---|---|
| SSS | Scores each segment based on stenosis severity | Quick estimation of plaque burden | Lacks detailed plaque composition |
| SIS | Scores the presence of plaque in each segment | Simple, rapid assessment | Does not quantify stenosis severity |
| Leaman Score | Considers plaque location, type, and stenosis degree | Detailed assessment | Time-consuming |
| Quantitative | Automated plaque volume and composition analysis | Accurate, detailed quantification | Requires advanced software |
CT – Computed Tomography; SSS – Segment Stenosis Score; SIS – Segment Involvement Score
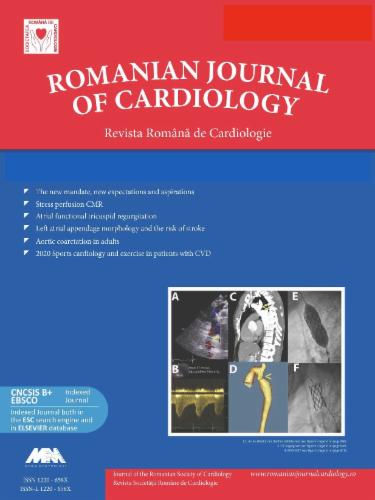
The advent of dedicated CCTA software has recently enabled the quantitative evaluation of coronary plaque burden. This software automatically traces the boundary between the lumen and the vessel wall or plaque surface and between the external wall and the epicardial fat. The volume between the lumen and the external wall of the vessel, corresponding to the plaque volume (in mm3), is calculated using an automatic algorithm.[28] Several studies have compared the most common CCTA software and the more sensitive invasive evaluation methods, such as intravascular ultrasonography (IVUS) and optical coherence tomography (OCT). These methods strongly correlate with evaluating coronary plaques analyzed by CCTA, even in patients with multivessel pathology.[29,30] While IVUS offers both substantial benefits and a low complications profile, its widespread adoption in cardiovascular imaging centers is hindered by elevated costs and the requisite expertise of operators.[29,30] Besides quantifying the overall coronary plaque burden, CCTA enables the characterization of atherosclerotic plaque composition (Figure 1). Therefore, coronary plaques can be classified based on the average HU value into calcific (>350 HU), fibrous (130-350 HU), and fibro-fatty (30-130 HU) plaques.[31] Furthermore, fibrous and fibro-fatty plaques can be subdivided based on spatial heterogeneity: homogeneous plaques exhibit similar HU values throughout, whereas heterogeneous plaques contain areas with varying HU values. [32] Furthermore, CCTA allows the identification of plaque high-risk features (HRF) from a qualitative/morphological point of view (Table 2): (1) positive remodeling, i.e. the increase of at least 10% in the external diameter of the vessel in correspondence with the plaque when compared to the reference segment of the same coronary vessel; (2) low attenuation plaque, i.e. low attenuation values within the plaque, <30 HU; (3) spotty calcifications, i.e. focal and small calcifications <3 mm; (4) Napkin-Ring Sign, i.e. a portion with higher peripheral ring-like attenuation than the non-calcified portion of the plaque.[33] These plaques correlate with a higher likelihood of future cardiovascular events, underscoring the importance of accurate plaque characterization.[33] In this regard, a sub-study of the ROMICAT II trial, which included 472 patients undergoing CCTA in the emergency room, highlighted how the presence of any of these high-risk characteristics was associated with a significant increase in the relative risk of experiencing ACS, regardless of the degree of stenosis.[34] Similar results were also obtained from a sub-study of the PROMISE trial, where HRF was associated with a higher rate of MACE. Moreover, this association remained consistent even after adjusting for cardiovascular risk profile and significant stenoses.[35]
Methods of coronary plaque characterization in the left anterior descending artery using the software Aquarius TeraRecon (North Carolina, United States of America). The histogram of different plaque components is depicted on the left panel.
Characteristics and clinical relevance of high-risk coronary plaque features detected by cardiac computed tomography angiography.[31]
| Plaque Feature | Description | Clinical Relevance |
|---|---|---|
| Positive Remodeling | Vessel enlargement at the plaque site | Indicator of plaque vulnerability |
| Spotty Calcifications | 1-3 mm calcifications in the context of a soft plaque | Indicator of plaque vulnerability |
| Low Attenuation Plaque | Low density (<30 HU) | Associated with increased risk of rupture |
| Napkin-Ring Sign | Hypoattenuating core with a hyperattenuating rim | A strong predictor of adverse events |
HU – Hounsfiled Units
Summary of the key conclusions of major trials evaluating the role of CCTA in cardiovascular risk assessment.
| Title | Journal, year | Key conclusions |
|---|---|---|
| Coronary CT Angiography versus Standard Evaluation in Acute Chest Pain (ROMICAT-II) [34] | N Engl J Med. 2012 |
|
| 1-Year Outcomes of FFRCT-Guided Care in Patients With Suspected Coronary Disease: The PLATFORM Study [46] | J Am Coll Cardiol. 2016 |
|
| Prognostic Value of Noninvasive Cardiovascular Testing in Patients With Stable Chest Pain: Insights From the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain)[5] | Circulation. 2017 |
|
| Coronary CT Angiography and 5-Year Risk of Myocardial Infarction (SCOT-HEART trial)[4] | N Engl J Med. 2018 |
|
| Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data[54] | Lancet. 2018 |
|
| CT or Invasive Coronary Angiography in Stable Chest Pain (DISCHARGE trial)[16] | N Engl J Med. 2022 |
|
In the context of the new available methods, dual-energy CT (DECT) can provide additional data and improve the differentiation of plaque components. This method utilizes two distinct photon spectra, which are produced either by modulating the voltage of a single X-ray tube or by operating two X-ray tubes at different voltage levels.[36]. Measuring differences in attenuation in images acquired with low- and high-energy spectra leads to improved tissue characterization.[36] Also, this technique can reduce artifacts caused by overlapping densities or the presence of metal, improving the overall quality of the images. On the other hand, interpreting DECT images requires specialized knowledge and experience to exploit the additional information the technology provides fully. In a study by Obaid et al., dual-energy levels (100 kV and 140 kV, respectively) enhanced sensitivity and specificity for identifying the necrotic core of plaques in ex vivo models.[37] Another ex vivo study also demonstrated the potential of DECT for differentiating between lipid-rich and fibrotic plaques.[38] Nevertheless, despite this evidence, further in vivo studies are needed to explore the role of DECT in plaque characterization.
Photon-counting CT (PCCT) constitutes a more recent and advanced promising approach to improve the accuracy of plaque analysis but with limited diffusion in clinical practice. In particular, the photon-counting CT method is based on measuring each penetrating photon individually to differentiate and quantify the structural composition of the atherosclerotic plaque.[39,40] PCCT offers a significant advantage in coronary artery imaging because it provides superior spatial resolution and image quality. By reducing artifacts associated with coronary stents, cardiac pacemakers, and calcified coronary plaques, PCCT enables more precise visualization of the coronary arteries. This enhanced image clarity is achieved through the separate quantification of multiple energy levels, facilitating more precise tissue characterization and accurately assessing calcified plaque burden.[39,40] Several studies, conducted either in vitro or postmortem, illustrate the high precision of the photon counting method in characterizing atherosclerotic plaques.[41,42,43] Recently, a study by Mergen et al., the first in vivo investigation involving 20 patients, demonstrated that the photon-counting method significantly reduced blooming artifacts, allowing for precise identification of non-calcific plaque components. (i.e. fibrotic and lipids).[44]
In addition to providing morphological details of coronary plaques, CCTA enables the integration of anatomical and functional assessments. This is particularly valuable in complex scenarios, such as in patients with known IHD or those who have undergone percutaneous or surgical revascularization, where non-invasive prognostic stratification can be challenging. CT-derived fractional flow reserve (FFRCT) allows us to obtain the exact measurement offered by the invasive approach but in a non-invasive way, exploiting fluid dynamics algorithms.[45] The PLATFORM trial prospectively evaluated the feasibility and safety of the FFRCT method compared to coronary angiography. The study confirmed the advantages of FFRCT, demonstrating equivalent clinical outcomes for patients with stable, new-onset chest pain undergoing both CCTA with FFRCT and coronary angiography.[46] While FFRCT offers significant diagnostic advantages, its widespread adoption in clinical practice is hindered by economic constraints. Contemporary real-world evidence indicated that FFRCT has the potential to rationalize patient management and accelerate diagnostic pathways but may not be cost-effective for all stenosis severity.47
Perfusion CT (CTP) is a more recent, advanced functional imaging technique used to evaluate myocardial blood flow, providing detailed information on tissue perfusion. However, CTP requires dedicated sequences and stressors such as adenosine and regadenoson, which are necessary compared to FFRCT. Static CTP provides only qualitative and semi-quantitative analyses, whereas dynamic CTP enables comprehensive quantitative measurements (mL/min/gram). However, both techniques are vulnerable to patient and cardiac artifacts and require prolonged and complex analysis.[48] Despite these disadvantages, CTP is reliable in evaluating microcirculatory dysfunctions, and adding CTP to CCTA can increase the sensitivity of detecting significant CAD.[49,50] Moreover, CTP can ensure tissue characterization even in patients with myocardial fibrosis due to myocardial infarction scars. Cardiac magnetic resonance imaging (MRI) is the gold standard for detecting cardiac fibrosis. However, its limited availability and various technical contraindications (such as non-compatible intracardiac leads) make CTP exams a potential alternative. From a physiologic point of view, CTP can offer the same diagnostic capabilities as cardiac MRI, including myocardial blood flow quantification and late contrast enhancement assessment, but with a shorter acquisition time.[49,50] Overall, CTP is a valuable tool, providing critical information on tissue perfusion that can guide clinical decision-making and treatment planning. In conclusion, the combined use of these functional methods may benefit symptomatic patients with an intermediate pre-test risk of CAD.[49, 50, 51]
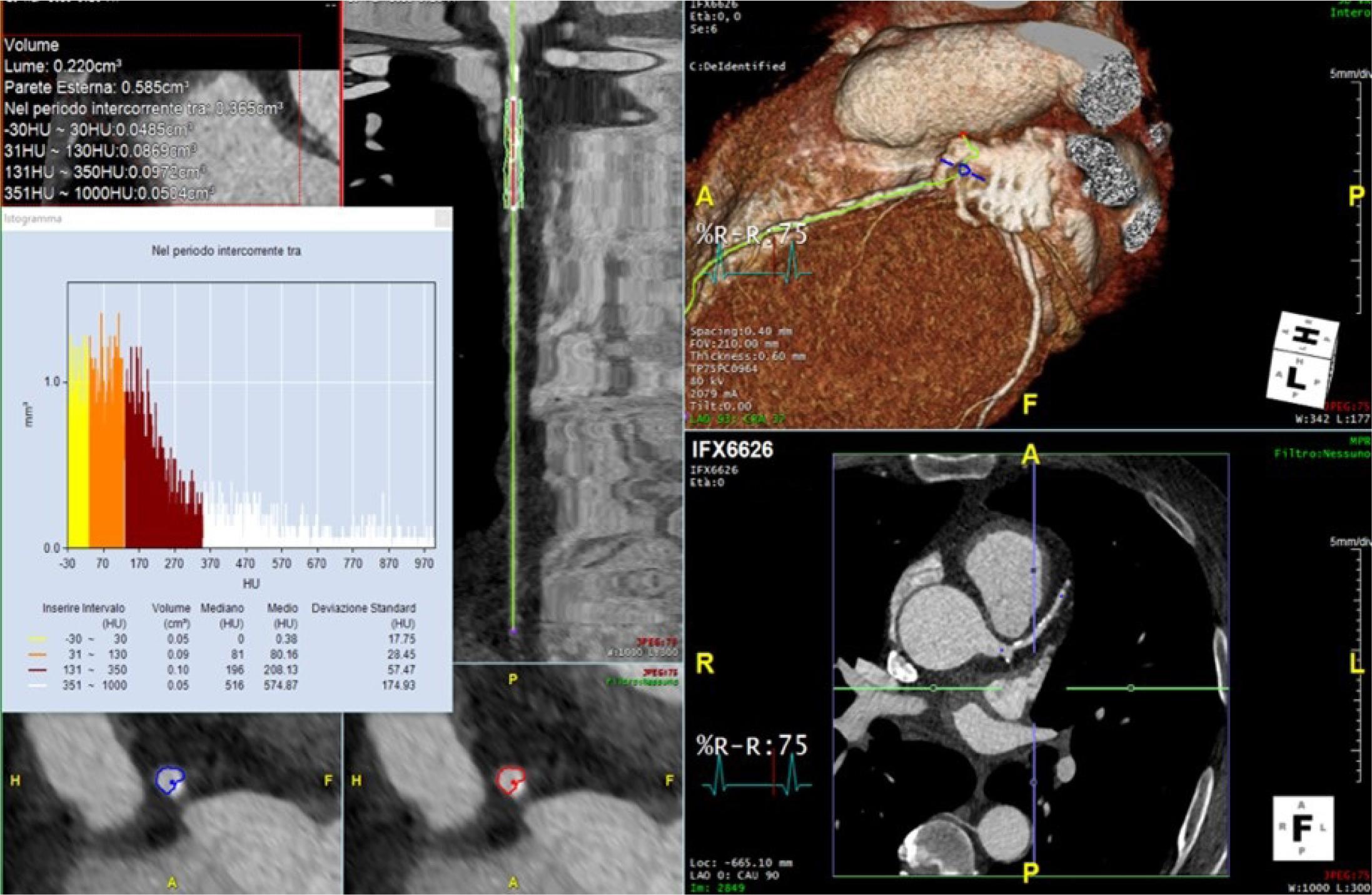
Perivascular coronary adipose tissue plays a fundamental role in the pathophysiology of cardiovascular diseases, particularly in the context of IHD, as it can release pro-atherosclerotic adipokines. [52] A strong bidirectional relationship exists between the coronary artery wall and the surrounding adipose tissue, making the latter an accurate sensor of inflammation levels. This relationship is evidenced by changes in the adipose tissue’s phenotype, including adipocyte differentiation, size, and the ratio of lipid to aqueous components.[53] A 3D tool, namely the Fat Attenuation Index (pFAI), has recently been developed, capable of accurately analyzing the weighted gradients in the CT attenuation of peri coronary fat (Figure 2).[51,53] The CRISP CT study, a post-hoc analysis of prospectively collected data from two large European centers, demonstrated how pFAI assessment significantly improved prognostic stratification in patients undergoing CCTA.[54] In particular, high pFAI values (cut-off 70.1 HU) were associated with an increased risk of all-cause death. [54] A recent study by Kuneman et al. highlighted the prognostic significance of pFAI, showing that in patients with ACS, the average pFAI value was higher around precursors of culprit lesions compared to non-culprit lesions and lesions in patients with chronic CAD.[55] This suggests that the inflammation process promotes the formation of high-risk plaques that tend to rupture before clinical symptoms appear. Evaluating pFAI with CCTA and assessing HRF presence can lead to a more accurate cardiovascular risk assessment.[55,56] A retrospective study of 371 patients undergoing CCTA demonstrated that in cases of mild and moderate stenoses, the presence of HRF (especially low attenuation plaque) and a high pFAI value were significantly and independently associated with an increased risk of mortality and invasive procedures.[57] The evaluation of pFAI can also find an interesting application of the assessment by CCTA of patients with elevated troponin values and electrocardiographic alterations but without critical coronary disease. In this context, a study documented that patients diagnosed with myocardial infarction with non-obstructive coronary arteries (MINOCA) had significantly higher average pFAI values compared to healthy individuals, indicating the presence of inflammation in this patient group.[58] The Oxford Risk Factors and Non-invasive Imaging (ORFAN) trial is the largest cohort of patients undergoing CCTA and has a higher follow-up period for cardiovascular outcomes.[59] This study revealed that quantitative assessment of perivascular inflammation using the FAI Score in patients without obstructive CAD identified a substantial subset of patients with elevated residual inflammatory risk and subsequent cardiovascular outcomes.[59] Therefore, the severity of inflammation, as measured by the number of inflamed coronary arteries, exhibited a dose-dependent association with increased risk of cardiovascular events. Moreover, the authors tested the ability of an artificial intelligence (AI) risk algorithm to predict future cardiovascular events in the same cohort of patients. They have demonstrated that this AI risk model presents high predictive values for cardiac mortality and MACE.[59] This study represents the inaugural demonstration of an AI-assisted predictive tool incorporating FAI score, atherosclerotic plaque burden, and patient risk factors for clinically significant risk reclassification in individuals undergoing routine CCTA.[59]
Pericoronary fat attenuation index (pFAI) analyses using the software Aquarius TeraRecon (North Carolina, United States of America) show gradients in the CT attenuation of peri coronary fat.
The currently available advanced plaque analysis techniques allow for obtaining additional prognostic information compared to traditional risk factors and anatomical evaluation with standard CT. Studies with long-term follow-up have demonstrated the important clinical implications in evaluating patients with suspected coronary disease. In a study of 1168 CCTA patients, a 5.7-year follow-up showed that patients with higher volumes of non-calcific and low-attenuation plaque had a greater incidence of MACE (cardiac death, myocardial infarction, and late coronary revascularization). [60] In a mixed cohort study of 274 asymptomatic patients, 254 with acute chest pain but no ACS, and 327 with ACS, quantitative plaque analysis showed an increase in total plaque volume across different risk profiles. ACS patients had plaques with low attenuation, containing more fibro-adipose and necrotic tissue.[61]
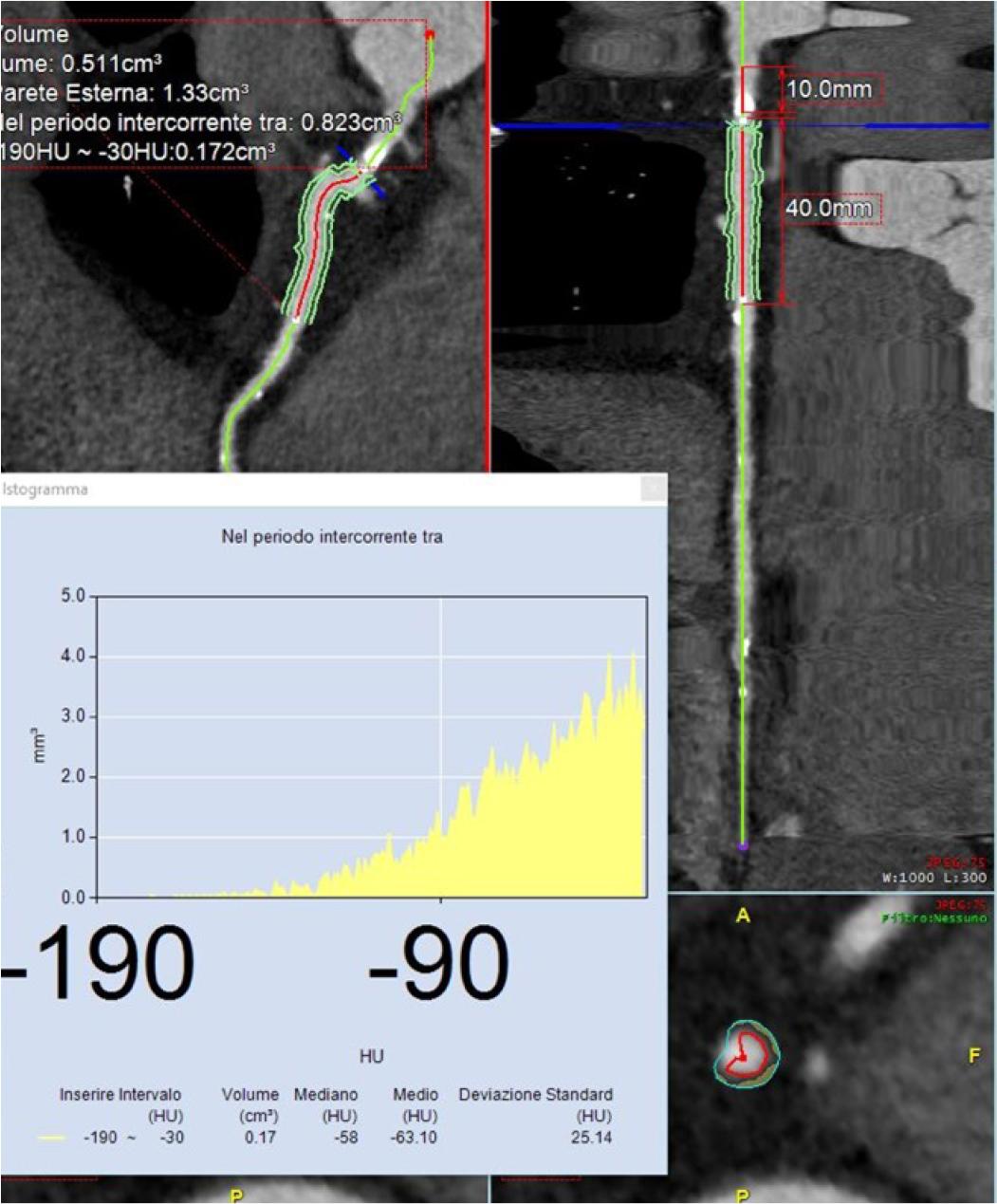
Integrating advanced plaque analysis into clinical practice significantly impacts patient management by enhancing risk stratification, guiding treatment decisions, and monitoring treatment effectiveness (Figure 3). A key advantage of quantitative analysis is its ability to monitor changes in atherosclerotic plaque composition over time, especially those induced by pharmacological treatments. [62] The multicenter PARADIGM study found that statin users experienced slower global atherosclerotic plaque progression and faster calcific plaque development.[63] Moreover, it was observed that diabetic patients presented a greater progression of plaque, not only in terms of disease burden but also of unfavorable characteristics.[64]
The proposed flowchart of the cardiac coronary computed tomography (CCTA) evaluation in patients with stable chest pain.
In clinical practice, CCTA can aid in selecting patients for coronary angiography. The CONSERVE trial showed that using CCTA improved coronary angiography’s diagnostic yield and reduced invasive procedures, leading to a 57% cost reduction.[65,66] There is also evidence of the possible application of CCTA in pre-procedural planning in patients who need coronary revascularization. In a study by Serruys et al., two heart teams were randomized to choose between PCI and CABG based on either CCTA images or coronary angiography. Each team calculated the anatomical SYNTAX score using their assigned imaging method and integrated clinical information to determine the SYNTAX score II, guiding the patient’s treatment. The study found high agreement on the final decisions between CCTA and coronary angiography.[67,68] Recently, the FAST TRACK CABG trial further confirmed these data, demonstrating that in a cohort of 114 patients with chronic coronary disease and low operative risk, the planning and execution of CABG was feasible based solely on CCTA. Furthermore, the follow-up conducted at 30 days using CCTA demonstrated good patency of the anastomoses in 92% of cases, while the percentage of complications was low.[69]
Despite the significant benefits of CCTA, especially quantitative plaque analysis, some limitations persist. The primary factors hindering broader adoption are radiation exposure and the need for potentially greater contrast medium injections.[70] While quantitative tools provide notable benefits, assessing their limitations and validating them against established methods is crucial to ensure they deliver reliable data for clinical decision-making.[71] Recent studies have compared leading quantitative analysis software with IVUS, a gold standard for assessing atherosclerotic plaque[72]. In one study evaluating 22 non-calcified plaques from 20 CAD-suspected patients, the software and IVUS showed an excellent correlation in plaque volume measurements.[72] Another study involving 51 patients demonstrated a strong correlation between software and IVUS in identifying plaque burden and minimal luminal area.[73]
While CCTA is a fast and widely available imaging technique, it is more costly than more straightforward stress tests. Additionally, plaque analysis software can be time-consuming and challenging to integrate into routine clinical practice. However, the advent of AI offers the possibility of increasing effectiveness and reducing human errors and interpretative variability.[] An interesting application of AI is the CaRi-Heart Risk score, a multiparametric tool designed to predict the risk of fatal cardiovascular events over 8 years. This score combines patient risk factors with assessments of plaque burden and pFAI.[75] Deep learning (DL) models can automatically measure the volume and composition of coronary plaque in CCTA scans, increasing the efficiency of the CCTA workflow. Moreover, AI-based stenosis evaluation can reduce inconsistencies between different readers and minimize errors in interpretation. A new deep learning system accurately measures coronary plaque and stenosis. This system was tested on a large dataset of 6,946 coronary lesions from 1,196 patients. It showed strong agreement with radiologists in measuring the degree of stenosis. Additionally, the system accurately categorized the stenosis’s severity, matching the clinical evaluation results.[74] This suggests that DL can be a reliable tool for diagnosing coronary artery disease. Beyond the role of diagnostics, AI tools also have the potential to predict MACE in patients with chronic coronary syndrome. Recently, a DL-based coronary plaque volume analysis was identified as predictive of cardiac events.[75] Finally, an attractive prospect concerns the possibility of integration with radiomic analysis. This approach is based on the ability to identify HRF by exploiting machine learning algorithms and big data datasets with thousands of plaque imaging features.[76] This approach promises to refine plaque characterization and improve prognostic accuracy.
Advances in CCTA-derived plaque analysis have significantly enhanced our ability to assess and manage IHD. By providing detailed insights into plaque characteristics and their clinical implications, these technologies are shaping the future of cardiovascular care. Continued research and technological innovation will further improve the accuracy and utility of CCTA in clinical practice. CTCA-derived plaque analysis extends beyond diagnostics to prognostication and therapeutic planning. Ongoing research continues to refine our understanding of the correlation between plaque characteristics and clinical outcomes. Future directions involve harnessing the full potential of CTCA in large-scale studies, fostering standardization in reporting, and exploring novel avenues, such as integrating functional information for a more holistic assessment.
The evolution of CTCA-derived plaque analysis signifies a paradigm shift in cardiovascular imaging, enhancing diagnostic accuracy, risk stratification, and treatment planning. As precision medicine advances, the integration of advanced CTCA-derived plaque analysis is poised to redefine the approach to intricate cardiovascular pathologies.