Atrial fibrillation (AF) is one of the most common arrhythmias, requiring close monitoring due to its complications and long-term prognosis. Inflammation plays a significant role in the development of arrhythmic events.1,2 It is well-known that patients presenting with AF, particularly those with a high ventricular response, often exhibit elevated inflammatory markers, which are considered important triggers. Cardioversion is one of the treatment methods used when rate control cannot be achieved or in appropriate patient groups. Approximately half of the patients undergoing cardioversion for AF experience recurrence within three months.3 The underlying cause of AF recurrence in these patients remains unclear. Although several scoring systems have been developed, there are no definitive data on which system is most effective in predicting cardioversion success. However, the role of inflammation in AF episodes is well established.
The leukoglycemic index (LGI), derived from a combination of blood glucose and leukocyte counts, is a parameter that has been studied in this context.4 The fibrosis-4 (FIB-4) index, primarily associated with liver disease, has been linked to mortality. The systemic immune-inflammation index (SII), originally used to predict survival in oncological and rheumatological cases, has recently gained attention. Despite their potential, the use of these three parameters in cardiology remains extremely limited. Recent studies have investigated their relevance in determining the prognosis of cardiovascular diseases.5,6 Because of their practicality, ease of calculation from routine blood tests, and potential high predictive value, these parameters are gaining traction in the field of cardiology. However, their impact on cardioversion success in patients with AF has not been thoroughly explored.
In this study, we aimed to investigate the effects of the LGI, FIB-4 index, and SII on cardioversion success in patients undergoing electrical cardioversion due to AF.
Ethical approval for the study was obtained from the local ethics committee. The study was conducted at a single center between 2019 and 2024 and followed a retrospective design. Patients aged 18 years and older who underwent cardioversion due to permanent AF were included. Patients with paroxysmal AF were excluded from the study. Additional exclusion criteria included patients with active infections, malignancies, a history of hematological diseases, acute coronary syndrome within the last month, congenital heart disease, severe valvular disease, and advanced liver or renal failure [glomerular filtration rate (GFR) < 15]; those who died after the procedure; and patients with incomplete data. The inclusion and exclusion criteria are shown in Figure 1.
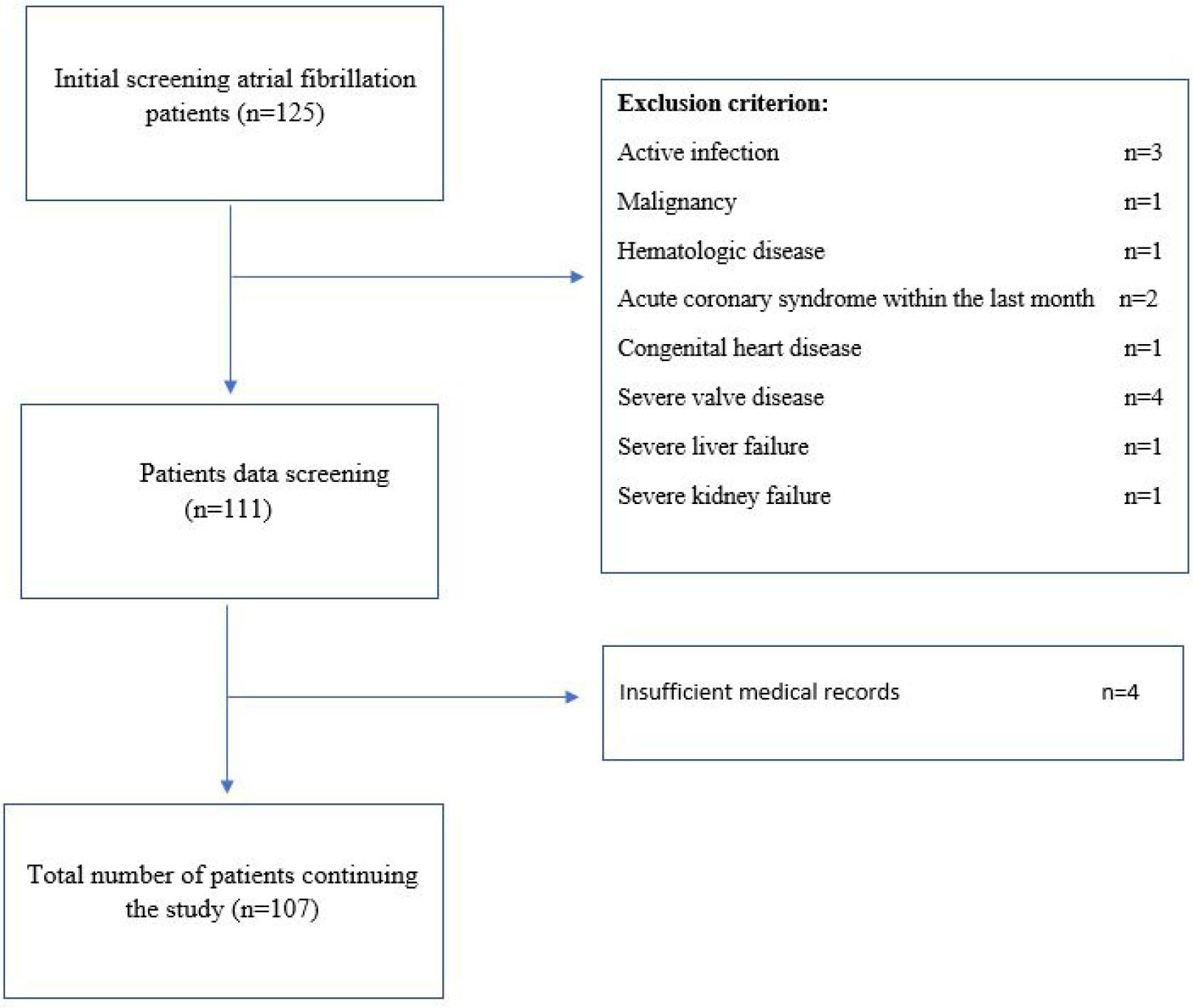
Study flowchart.
A total of 107 patients were included in the study: 64 patients in whom sinus rhythm was achieved following electrical cardioversion and 43 patients in whom sinus rhythm was not restored. Patients were systematically classified based on their demographic, clinical, and laboratory characteristics. Follow-up was conducted after cardioversion. At the three-month follow-up, a 12-lead electrocardiogram (ECG) was performed to determine whether patients were in sinus rhythm or AF. Those still in sinus rhythm at the three-month follow-up were classified in the successful cardioversion group. Data on age, gender, hypertension, diabetes mellitus, and other patient characteristics were obtained from medical records. Blood glucose measurements were made after at least eight hours of fasting. Measurements were made from blood taken from a peripheral vein. All patients with diabetes were using oral antidiabetic drugs, and there were no patients using insulin. Among the drugs used, all patients were taking metformin. While six of the patients who underwent successful cardioversion were taking metformin+sulfonylurea, four of the patients in the unsuccessful cardioversion group were using metformin+sulfonylurea. All patients were not routinely taking antiarrhythmic drugs before the procedure. All patients were taking beta-blockers. All patients were loaded with the same amount of amiodarone just before the procedure, and all patients were given the same amount of amiodarone maintenance infusion after the procedure. All patients were prescribed amiodarone 3*1 tablets at discharge. The relationship between demographic and laboratory findings and cardioversion success is shown in Table 1. Echocardiographic parameters were reviewed by two experienced cardiologists, and patients with inconsistent findings were excluded from the study. The relationship between echocardiography findings and cardioversion success is shown in Table 2. Hematological and biochemical parameters were collected for all patients. LGI was calculated using the following formula: (white blood cell count × glucose) / 1000. LGI values were measured at least 24 hours before cardioversion and at least 24 hours after the procedure. The FIB-4 index was calculated as [age × AST] / [platelet count × ✓ALT] (where AST is aspartate aminotransferase and ALT is alanine aminotransferase), and SII was calculated as [(neutrophils × platelets) / lymphocytes].
Relationship between demographic and laboratory findings and cardioversion success
| Variables | Successful CV (n = 64) | Unsuccessful CV(n = 43) | p-value |
|---|---|---|---|
| Age, years | 65.5 ± 11.3 | 62.9 ± 13.6 | NS |
| Gender (%) | |||
| Male | 54.7 | 46.5 | NS |
| Female | 45.3 | 53.5 | |
| Hypertension (%) | 78.1 | 74.4 | NS |
| Diabetes mellitus (%) | 25 | 23.3 | |
| -- Metformin | 25 | 23.3 | NS |
| -- Metformin+Sulfonylurea | 9.3 | 9.3 | |
| WBC (′109/L) | 10.7 ± 10.7 | 8.9 ± 2.6 | NS |
| Hemoglobin, g/dl | 13.5 ± 1.9 | 13.5 ± 2.2 | NS |
| PLT (′109/L) | 264 ± 60 | 241 ± 77 | NS |
| GFR | 78 ± 27 | 79 ± 24 | NS |
| Urea, mg/dl | 38.8 ± 15.4 | 39 ± 13.9 | NS |
| Creatinine, mg/dl | 1.0 ± 0.2 | 1.0 ± 0.3 | NS |
| Albumin | 4.1 ± 0.3 | 3.7 ± 0.5 | NS |
| TSH, mU/L | 2.2 ± 1.8 | 2.8 ± 2.5 | NS |
| SGOT, U/L | 20.7 ± 7.9 | 22.7 ± 15.6 | NS |
| SGPT, U/L | 22.3 ± 13.1 | 32.6 ± 55.8 | NS |
| Pre-procedural LGI | 1.2 ± 1.2 | 1.07 ± 0.3 | NS |
| Post-procedural LGI | 0.92 ± 0.41 | 1 ± 0.9 | NS |
| Fibrosis-4 index | 1.2 ± 0.5 | 1.5 ± 1.2 | NS |
| SII | 735 ± 409 | 840 ± 757 | NS |
CV: cardioversion; WBC: white blood cell; PLT: platelet; GFR: glomerular filtration rate; TSH: thyroid-stimulating hormone; SGOT: aspartate aminotransferase; SGPT: alanine aminotransferase; LGI: leukoglycemic index; SII: systemic immune-inflammation index; NS: no significance
Relationship between echocardiography findings and cardioversion success
| Variables | Successful CV (n = 64) | Unsuccessful CV(n = 43) | p-value |
|---|---|---|---|
| Ejection fraction (EF) | 53.1 ± 8.5 | 56.3 ± 7.7 | NS |
| End diastolic diameter (EDD) | 48.7 ± 4.5 | 48.1 ± 5.4 | NS |
| End systolic diameter (ESD) | 29.8 ± 5.1 | 29.8 ± 6.5 | NS |
| Left atrium (LA) | 41.9 ± 5 | 40.6 ± 5.6 | NS |
| Systolic pulmonary artery pressure (sPAP) | 36.8 ± 10.5 | 38 ± 11.5 | NS |
| Mitral stenosis | 3 (4.7) | 3 (7) | NS |
| Mitral insufficiency | 12 (18.8) | 6 (14) | NS |
| Heart rate | 97.9 ± 28.1 | 89.7 ± 22.5 | NS |
CV: cardioversion; NS: no significance
Data analysis was performed using SPSS software (version 20.0; SPSS Inc., Chicago, IL). Continuous variables were expressed as mean ± standard deviation or median [interquartile range (IQR)], depending on the data distribution. Independent Student’s t-tests were used to compare differences between two groups for normally distributed variables, and the Mann–Whitney U test was used for non-normally distributed variables. Differences in categorical variables were assessed using the Chi-square test. p-value < 0.05 was considered statistically significant.
The mean age of patients with successful cardioversion was 65.5 ± 11.3 years, while for those with unsuccessful cardioversion, it was 62.9 ± 13.6 years. No statistically significant difference was observed between the groups. Although hypertension and diabetes mellitus were more prevalent in the successful cardioversion group, no statistically significant difference was found between the groups.
Laboratory parameters such as white blood cell count (WBC), platelet count (Plt), and albumin levels were numerically higher in the successful cardioversion group, but no significant differences were detected between the groups. AST and ALT levels were higher in the unsuccessful cardioversion group, but again, no statistically significant difference was observed between the groups.
The pre-procedural LGI was found to be higher in the successful cardioversion group, but this difference was not statistically significant. Although the FIB-4 index and SII were numerically higher in the unsuccessful cardioversion group, no statistically significant difference was found between the groups.
Echocardiographic parameters such as left atrial diameter and mitral regurgitation rate were higher in patients with successful cardioversion, but no statistically significant differences were detected between the groups. Heart rate was also higher in the successful cardioversion group, yet no statistically significant difference was observed.
LGI has recently gained attention in cardiology, particularly in studies related to the prognosis of coronary artery disease (CAD). In CAD, an increase in neutrophil dominance results in higher proteolytic enzyme release, which exacerbates endothelial damage. This endothelial dysfunction can cause electrical instability in the heart, leading to arrhythmias that negatively impact the prognosis of CAD. While the relationship between LGI and CAD has been studied, there is no published research on its association with AF, despite AF being one of the most common arrhythmias.
Inflammation has been identified as an independent risk factor for the development of AF in various studies.7–9 In a study by Zheng et al., they found that patients with AF with higher SII had a worse prognosis.10 In our study, SII was also found to be higher in patients with unsuccessful cardioversion; however, no statistically significant difference was observed between the groups. This lack of statistical significance may be related to our relatively small sample size and the short follow-up period.
AF occurs in approximately one in three patients postoperatively after cardiac surgery, often due to increased inflammatory cytokines during the postoperative period.11 Elevated levels of inflammatory markers are often seen in the blood parameters of these patients. Inflammation is also a crucial factor for cardioversion success in patients with AF. Some studies have shown that inflammation markers like C-reactive protein (CRP) are associated with cardioversion success in patients with AF.12 For example, Yo et al. found that patients with higher pre-cardioversion high-sensitivity CRP (hsCRP) levels had a higher recurrence of AF.13 Similarly, a study by Meyre et al. found that patients with elevated hsCRP levels before catheter ablation had a higher AF recurrence rate within one year after successful ablation.14 Jani et al. showed that AF recurrence is most common within the first three months after cardioversion.15 Based on this evidence, we chose a three-month follow-up period to assess cardioversion success in our study.
Atrial electrical remodeling occurs within the first 24 hours after cardioversion and is known to affect cardioversion success in patients with AF. In AF, inflammatory markers like WBC are known to accumulate in the atrial tissue. In our study, we assessed the LGI before and after cardioversion to examine its potential impact on atrial electrical remodeling and cardioversion success.
The increased stress response in AF not only leads to a buildup of inflammatory cells in the atria but also contributes to a hyperglycemic environment. Patients with higher LGI are expected to have a lower success rate for cardioversion due to this atrial impact. In addition, the long-term stress response may suppress myocardial contractility, potentially explaining the negative effects of high LGI on cardiac function. Future studies could explore the relationship between LGI and tachycardia-induced cardiomyopathy in patients with long-term AF. In our study, LGI was higher before the procedure in the successful cardioversion group, but no statistically significant difference was found between the groups. This could be due to several factors, including the lack of consideration for the diabetic status of the patients or the fact that many patients were on intense medical therapy for AF, reducing the presence of high ventricular response AF episodes.
The chronic pressure load created by mitral regurgitation (MR) can cause structural remodeling of the atrium, i.e., fibrosis. Fibrosis can sometimes limit the electrical pathways of the heart, making it difficult for AF to continue. Therefore, fibrotic tissue can limit the irregular spread of electrical impulses throughout the atrium, creating a more stable electrical environment during cardioversion.16 Studies showing that fibrotic tissue reduces the frequency of AF attacks by limiting electrical conduction support this hypothesis.17 In patients with MR, the constant pressure load created by blood leaking back into the left atrium can lead to atrial remodeling over time. This can result in enlargement of the left atrium. Various studies have shown that atrial enlargement may provide electrical stability, which may increase stability during cardioversion and increase the likelihood of successful rhythm conversion. This has led to the hypothesis that an enlarged left atrium may positively affect electrical stability. Since the surface area of an enlarged atrium increases, the propagation process of electrical waves may change. The increased surface area suggests that small-scale electrical impulses propagating from irregular foci may follow a more organized conduction path instead of large, disorganized AF waves. This may help electrical fluctuations to spread over a wider area and reduce local concentrations. Therefore, it may contribute to easier electrical stability during cardioversion.18 The increase in atrial wall tension and its positive effects on cardioversion are supported by studies on tension increase and changes in the electrical behavior of myocytes. In this area, there is evidence that the dilated atrium may have more effective excitability during cardioversion. The hypothesis that the dilated atrium better absorbs high-voltage current during electrical cardioversion is based on findings that the dilated atrium spreads electrical energy over a wider area.19
The FIB-4 index is a parameter that has gained significant attention in recent years due to its high predictive value and ease of calculation in daily practice. High FIB-4 index levels have been associated with adverse outcomes in the general population, especially in patients with liver cirrhosis. Over time, patients with AF may experience impaired right heart function and are more prone to diastolic heart failure and right-sided heart failure compared to healthy individuals. In these patients, increased filling pressures in the right atrium and right ventricle, along with backward flow of blood, can lead to venous congestion in the liver and surrounding areas, causing liver dysfunction. Karabağ et al. found elevated FIB-4 index levels in patients with acute pulmonary embolism, attributing this to impaired right heart function.20 In our study, FIB-4 index levels were also higher in patients with unsuccessful cardioversion, but no statistically significant difference was observed between the groups. This could be due to the relatively small sample size and the lack of evaluation of comorbid conditions that may affect right heart function, such as lung disease or tricuspid valve disease.
Our study has several limitations. Being retrospective in nature, the small sample size, and the short follow-up period are among the main constraints. Other limitations include the lack of division of patients into homogeneous groups based on the presence or absence of diabetes when calculating the LGI, having a more heterogeneous patient group, using fewer subjects, and not including some biological markers that have higher theoretical relevance in terms of AF pathophysiology. The fact that we could not include factors, such as clinical presentation of AF, European Heart Rhythm Association (EHRA) class, and history of ablation before cardioversion, in detail and that the patients’ glycated hemoglobin levels were not recorded are additional restrictions. Moreover, we did not take into account patients’ histories of chronic liver disease, chronic lung disease, or rheumatologic diseases when assessing the FIB-4 index, which may also be considered a limitation.
AF is a significant arrhythmia that can lead to high mortality and morbidity. Various scoring systems have been developed to predict cardioversion success. The LGI, FIB-4 index, and SII are parameters that may affect cardioversion outcomes. However, these parameters are insufficient on their own to predict cardioversion success. Larger, more comprehensive randomized studies are needed to better elucidate the effectiveness of these indices.