The synthesis of vitamin D3, or the „sunshine vitamin,” begins at the level of the skin, where, under the action of solar rays such as type B ultraviolet with a wavelength between 290 and 315 nanometers, the photochemical conversion of 7-dehydrocholesterol into pre-vitamin D3 takes place, which is then converted by isomerization into vitamin D3, a steroid hormone (1). Several factors can alter skin synthesis: skin pigmentation, age, use of sun protection creams, and amount of ultraviolet B type available depending on latitude, seasonality, time of day, duration, and intensity of direct sun exposure (2).
Vitamin D is crucial in controlling calcium and phosphorus metabolism through its effects on the parathyroid glands, kidneys, and intestines (3). In addition to poor musculoskeletal health, vitamin D deficiency has been linked to hypertension, abnormal lipid levels, obesity, diabetes, and cardiovascular diseases (CVD) (4,5).
Vitamin D deficiency is a widespread condition with an estimated prevalence of around 30–80% among adults globally (6). Based on Endocrinology Society guidelines, clinicians should aim for a 30 ng/ mL level of 25 (OH)D and a daily vitamin D intake of up to 2,000 IU (7). While a serum level of 25 (OH)D above 30 ng/mL is generally considered sufficient for enhancing the health of muscles and bones, the ideal level for other organs is still debatable (8).
The world’s leading cause of death is cardiovascular disease (9). Although the number of deaths caused by cardiovascular disease has reduced in developed countries in the past few years, it is anticipated that around 23.3 million people will die from it by 2030. Therefore, more investments are being made in preventing and treating cardiovascular risk factors (10,11).
The Tromsø study found that individuals with the lowest serum 25 (OH)D levels had a 32% higher mortality risk than those with the highest levels. The study took place over 11 years and involved 4751 participants in northern Norway (12). Similarly, in the Framingham Offspring Study, a group of 1739 individuals was observed for 5.4 years, and it was found that the hazard ratio for a cardiovascular incident was 1.80 for those whose serum 25(OH)D levels were <10 ng/mL compared with those with levels >15 ng/ml (13).
Dyslipidemia plays an essential role in the incidence of cardiovascular diseases, causing the onset of atherosclerosis and thereby favoring the occurrence of coronary heart disease and stroke (10,11).
Dyslipidemia is a metabolic condition characterized by abnormal levels of serum lipids, including total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG) (14).
Observational studies have shown a positive correlation between elevated 25-hydroxyvitamin D levels and a favorable serum lipid profile. As a result, recent studies have explored the effectiveness of taking vitamin D supplements as a potential treatment approach for various conditions, including dyslipidemia (15).
According to a recent meta-analysis, vitamin D supplements significantly decreases TC, TG, and LDL-C (16). Another metaanalysis found no statistically significant effects on the lipid profile from vitamin D supplementation; therefore, it is impossible to draw firm conclusions (17).
This study aimed to assess the impact of oral daily vitamin D supplements on the lipid profile among patients with CVD risk.
We conducted a prospective study on 154 patients randomly referred to the Endocrinology Department of County Clinical Emergency Hospital Bihor, Oradea, from September 2018 to March 2020, investigating the effect of oral daily vitamin D supplementation on lipid profile. The patients were followed for 6 months after admission.
The hospital`s Ethics Committee approved the study. All subjects gave their written informed consent before entering the study, and all procedures were done in agreement with the Declaration of Helsinki.
Patients were 19 to 82 years old and had at least one cardiovascular risk factor, such as hypertension, diabetes, dyslipidemia, or obesity. For each patient, we have completed medical records with demographic characteristics, previous medical and personal history, and previous treatment. Physical examination findings and anthropometric measurements were noted.
Key exclusion criteria included being on vitamin D supplements, having a history of acute or chronic liver or renal disease, hyperparathyroidism, or hypercalcemia.
Patients were assigned to receive one pill of 2,000 international units (IU) of vitamin D3 (cholecalciferol) daily for 6 months, whether on statin or not. The compliance rate was determined by requesting patients to return the medicine containers.
A blood sample was taken to determine the level of vitamin D, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG). Blood sampling was performed at baseline and at 6 months, according to common standards in clinical biochemistry.
Vitamin D status was divided into 4 categories: deficiency (≤20 ng / dl), insufficiency (21-29 ng / dl), optimal level (30-100 ng / dl) and toxicity (≥100 ng / dl).
Dyslipidemia was considered present in the following cases: a level of total cholesterol above 200 mg/dl, LDL cholesterol with values higher than 100 mg/dl, HDL cholesterol with values lower than 50 mg/dl, and triglycerides with values above 150 mg /dl.
Statistical analysis was performed with MedCalc® version 12.5.0.0 (MedCalc® Software, Mariakerke, Belgium). Kolmogorov- Smirnov test was used to assess the normal distribution of variables. Continuous variables with normal distribution were represented by mean and standard deviation, and those with asymmetric distribution by interquartile range, as well as frequency and percentage for categorical variables. Chi-square test (for categorical variables), paired or unpaired Student-test (for normal distribution), and Wilcoxon test or Mann–Whitney test (for non-normal distribution) were performed to analyze between-group differences. In the study, a p-value <0.05 was considered statistically significant.
A total of 154 patients responded to our re-evaluation request 6 months after initiation of treatment with vitamin D 2000 international units (IU) daily. Serum level of vitamin D showed a significant increase after 6 months of treatment: from a mean basal level of 18.5 ng/ml (± 9.0) to a mean level at 6 months of 43.1 ng/ml (± 9.5) – p<0,0001 (Student’s test for paired groups).
About two-thirds of patients were on cholesterol medication; therefore, 100 patients received vitamin D supplements in addition to the statin treatment, and 54 benefited from oral vitamin D treatment only.
We compare the two groups’ initial demographic and clinical data (Table 1).
| Characteristic | With Statin (n=100) | Without statin (n=54) | P value |
|---|---|---|---|
| Sex (M/F) | 40/60 | 16/38 | 0,2709* |
| Age (years) – mean (SD) | 60,3 (7,6) | 57,3 (13,1) | 0,0731** |
| BMI (kg/m2) – mean (SD) | 28,2 (7,3) | 30,3 (6,1) | 0,0739** |
| 25 OH-vitamin D level (ng/dl) – mean (SD) | 19,0 (9,7) | 17,2 (7,7) | 0,2401** |
M=male, F=female, SD=standard deviation
*- chi-square test with Yates’ correction
**- Student test for independent groups
Patients who also received statins were older than those in the non-statin group, but this difference did not reach statistical significance. There were no significant differences between groups regarding gender distribution and body mass index. In contrast, the serum level of vitamin D initially was lower in cases treated without statins, but this difference did not reach the statistical significance threshold either.
If we refer only to patients who did not receive statins during the 6 months, only vitamin D, the following laboratory results were recorded (Table 2).
| Parameter | Baseline | After 6 months of treatment | P value |
|---|---|---|---|
| 25 OH-vitamin D level (ng/dl) – mean (SD) | 17,3 (7,7) | 43,2 (9,8) | <0,0001* |
| Total cholesterol (mg/dl) – mean (IQR) | 186,5 (171-213) | 185,5 (173-210) | <0,0001** |
| HDL cholesterol (mg/dl) – mean(IQR) | 54,5 (46-62) | 54,5 (47-63,3) | 0,0697** |
| LDL cholesterol (mg/dl) – mean (IQR) | 113 (90-127) | 110 (90-125) | <0,0001** |
| Triglycerides (mg/dl) – mean (IQR) | 91,5 (66-113) | 93 (67-115) | 0,9578** |
SD=standard deviation, IQR=interquartile range, HDL= high density lipoproteins, LDL= low density lipoproteins
*- Student test for paired groups
**- Wilcoxon test
The effect on serum 25 OH vitamin D level is significant in the group treated only with vitamin D supplements. A significant improvement was observed in the total cholesterol and LDL levels even if the patients did not benefit from statin treatment (Figure 1). No statistically significant change was observed in HDL cholesterol and triglycerides in this group.
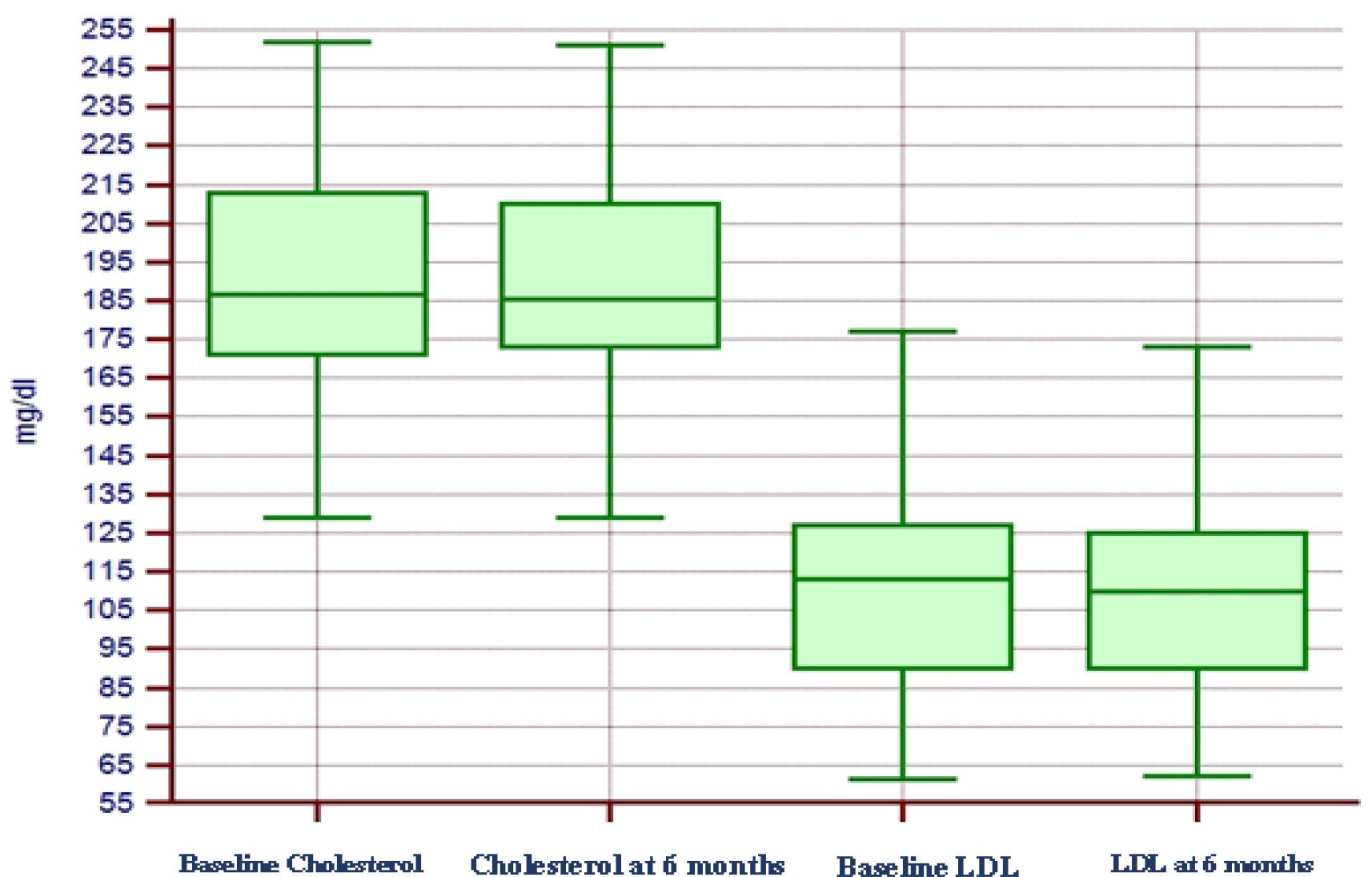
Evolution of serum level of total cholesterol and LDL cholesterol in patients who did not receive statin treatment during the follow-up period. (LDL=low density lipoproteins, IQR-interquartile range)
The differences regarding the laboratory test results between the two reference points (difference = value at 6 months - initial value), related to the two groups studied (with and without statins associated with oral vitamin D treatment), are described in Table 3.
| 6 months differences | Statin group (n=100) | Without statin group (n=56) | P value |
|---|---|---|---|
| 25 OH-vitamin D level (ng/dl) – medie (IQR) | +23,9 (+19,4 - +29,3) | +29,2 (+19,9- +29,7) | 0,0139* |
| Total Cholesterol (mg/dl) – mean (IQR) | -2,0 (-5 - -1) | -2,0 (-4 – 0,0) | 0,2491* |
| HDL cholesterol (mg/dl) – mean (IQR) | +1 (0 - +1) | 0 (0 - +1) | 0,0168* |
| LDL cholesterol (mg/dl) – mean (IQR) | -2,0 (-4 - -1) | -1 (-2,8 - 0) | 0,0013* |
| Triglycerides (mg/dl) – mean (IQR) | -1 (-2 - 0) | -0,5 (-1 - +1) | 0,0105* |
IQR=interquartile range, HDL= high density lipoproteins, LDL= low density lipoproteins
Significant differences were observed in serum LDL cholesterol, HDL cholesterol, and triglyceride changes. The decreases observed among patients who received statins were more pronounced than those who received only vitamin D supplementation. However, the reductions in total cholesterol were comparable.
In this study, we investigated the impact of daily vitamin D supplementation on lipid profiles among patients at high risk of cardiovascular disease.
In our study, more than half of the patients had vitamin D deficiency (62.33%). The prevalence of vitamin D deficiency is a major pandemic health problem affecting both adults and children. It is estimated that around 30-50% of people worldwide are affected by vitamin D deficiency, and around 70% of Europeans are affected by it [18]. In Romania, current data suggests that 40-75% of people are vitamin D deficient (19).
In our study, vitamin D supplementation significantly improved serum vitamin D levels. This finding is consistent with previous studies on vitamin D supplementation (20, 21). It has been reported that the intake of 100 international units (IU) of vitamin D can increase the serum level of vitamin D by 1 ng/ml (22).
In our study, the daily doses of vitamin D were those recommended by the Endocrine Society in its guidelines to clinicians, and none of the study patients reached the toxic level of vitamin D concentration, which is above 100 ng/ml and the upper limit for hypercalcemic serum concentration of the vitamin D (7,23). This proves that recommended doses do not reach toxic levels of vitamin D in serum while successfully correcting states of deficiency and insufficiency, and daily doses of 2000 IU could be considered safe and effective.
Many studies have demonstrated a clear relationship between low vitamin D levels and a higher risk of cardiovascular disease and mortality (24, 25).
A large meta-analysis, which included 34 studies with over 180,000 participants, examined published dose-response associations between vitamin D levels and cardiovascular disease (CVD) outcomes. The correlation between the dose and response demonstrated a non-linear increase in the risk of cardiovascular events when vitamin D levels were below 20 ng/ml. Still, there was no additional reduction in CVD events at higher levels. This meta-analysis showed a consistent decline in the relative risk of cardiovascular disease mortality from 5 ng/ml vitamin D to the highest value measured, 40 ng/ml (24). On the other hand, The Vitamin D and Omega-3 (VITAL) Supplemental Study sought to determine whether vitamin D supplements could be a helpful strategy for the primary prevention of cardiovascular disease and cancer. The study found no difference between the two treatment groups’ outcomes regarding mortality or the occurrence of major cardiac events, even with a large study population of 25,871 people and a sufficient dosage of 2,000 IU of vitamin D (26).
Dyslipidemia is a known risk factor for CVD and is linked to vitamin D deficiency (27). Numerous studies have been conducted in various populations to examine the relationships between vitamin D and serum lipids. A study conducted in Germany found that among older women, levels of 25 hydroxyvitamin D (25(OH)D) were inversely correlated with total cholesterol and low-density lipoprotein cholesterol (LDL-C) and positively correlated with high-density lipoprotein cholesterol (HDL-C) (28). Results from a Finnish study involving 909 men between the ages of 45 and 75 show that serum 25(OH)D levels are negatively associated with total cholesterol, triglycerides (TG), and LDL-C (29). A 10 nmol/l increase in 25(OH) D was linked to a reduction in triglycerides and very low-density lipoprotein cholesterol (VLDL-C), according to study results on 4,330 adult Danish subjects (30).
In the present study, a reduction in serum total cholesterol and LDL-C was associated with vitamin D supplementation. Still, there was no significant impact on HDL-C or triglycerides in the statin-free group. Consistent with our results, prior research has shown notable positive effects on lipid profiles (31), whereas others found no benefit (32). These varying outcomes may be attributed to differences in population characteristics, study design, variations in dosage supplementation, and confounder variables.
A large meta-analysis summarized data from randomized clinical trials on the effect of vitamin D supplementation on lipid profile. The findings show that vitamin D supplementation increases HDL-C and decreases total cholesterol, LDL-C, and triglycerides in a minor but significant way (33). Similar effects of vitamin D supplementation were reported in a more recent meta-analysis for total cholesterol, LDL-C, and triglycerides (34). These results are in line with our study results regarding the effect on total and LDL-C. The results of the group treated with vitamin D supplementation and statin were slightly different, with the most beneficial results on LDL-C,
HDL-C, and triglycerides. The International Lipid Panel suggested that statin, combined with vitamin D supplementation, could be an effective management strategy for hypercholesterolemia, especially in patients with vitamin D deficiency (35). Some studies showed a lowering effect on total cholesterol and LDL-C in patients receiving atorvastatin treatment combined with vitamin D supplementation compared to those with atorvastatin alone (36).
However, there are also studies with conflicting findings. In a double-blind, randomized, placebo-controlled trial from Norway, which included a total of 251 healthy adults with low vitamin D levels, 4 months of vitamin D3 supplementation did not affect lipid profiles (37). Similarly, a significant retrospective study that included 8592 patients with low vitamin D (average baseline level of 14.3 ng/mL) discovered that elevating the vitamin D level to 41.6 ng/mL did not improve serum lipid levels (38).
Several analyses based on the duration of the intervention indicate that vitamin D treatment has a more substantial impact on LDL-C in trials of shorter duration. One possible reason for this could be that longer-duration studies are often linked to inadequate adherence from participants. Conversely, research of extended duration demonstrated a noteworthy decrease in HDL-C levels (39).
There are various ways in which vitamin D might impact lipid metabolism. Earlier data indicated that a rise in calcium absorption in the intestines could potentially decrease the synthesis and release of hepatic triglycerides (40). Vitamin D may prevent the synthesis and release of TG by promoting calcium absorption in the intestines. Additionally, it has been proposed that increased intestinal calcium could decrease fatty acid absorption by producing insoluble calcium- fat complexes. Reduced fat absorption, mainly from saturated fatty acids, would lower serum LDL-C levels. Furthermore, calcium may increase the conversion of cholesterol into bile acids, lowering cholesterol levels (41). Other investigations have found that high parathyroid hormone (PTH) levels can contribute to a rise in TG, while higher vitamin D concentrations can lower serum PTH levels (31). As a result, vitamin D may affect TG concentrations by controlling PTH levels. Moreover, prior research has presented compelling proof linking insufficient vitamin D levels to impaired beta-cell performance and insulin resistance. This, in turn, could impact the metabolism of lipoproteins, resulting in elevated triglyceride levels and reduced HDL cholesterol levels. Furthermore, it has been proposed that vitamin D plays a role in lipid metabolism, including the formation of bile acid in the liver, indicating that vitamin D may directly impact lipid regulation (42).
There are additional suggested ways in which vitamin D may influence lipid metabolism, namely increasing the activity of genes related to fatty acid oxidation and generating new mitochondria in fatty tissue (43). Vitamin D is primarily stored in adipose tissue, and there is a strong correlation between obesity and a high occurrence of vitamin D deficiency (44). An intervention study showed that the decrease in adiposity was correlated with the increase in serum vitamin D concentrations. Research indicated that human adipocytes express vitamin D receptors and enzymes responsible for metabolizing vitamin D, such as 25-hydroxylase and 1α-hydroxylase. This finding suggests that vitamin D plays a role in influencing the biology of adipose tissue (43, 44).
According to the Endocrine Society, the maximum acceptable level of vitamin D intake per day is set at 10,000 IU. Based on their Clinical Practice Guidelines, it can be indirectly assumed that they consider vitamin D levels between 30 ng/dl and 100 ng/dl sufficient. In comparison, levels above 100 ng/dl may pose potential risks (45). Vitamin D supplementation at doses of 2,000 IU/day is generally safe, but we still don’t know its useful dose for treating non-bone diseases.
Our study has limitations: we used only one supplementation dose of vitamin D3, there are a low number of patients, and patients are only from a single center. To further understand vitamin D’s therapeutic potential for dyslipidemia, large-scale randomized studies of vitamin D supplementation should be designed to assess changes in serum lipid levels in well-defined groups.
We found that 2000 IU vitamin D supplementation daily for 6 months benefits serum lipid levels. In conclusion, raising serum vitamin D concentrations may be beneficial in treating dyslipidemia in patients with cardiovascular risk factors. Further studies regarding the beneficial effect of vitamin D supplementation on profile lipid outcomes are required.