Aortitis includes both infectious and more commonly non-infectious conditions that lead to inflammation of the arterial wall.[1] While non-infectious forms are often associated with large vessel arteritis from rheumatic conditions, infectious forms, though rare, can occur in isolation and are a serious complication of infective endocarditis.[2] These infectious cases carry a worse prognosis due to the rapid onset of acute aortic syndromes (AAS), requiring immediate diagnosis and specific treatment.[1] Infections caused by Staphylococcus, Salmonella, and mycobacteria have been known to lead to infective aortic disease.[3] Due to the non-specific symptoms such as fever, loss of appetite, weight loss, and localized abdominal or back pain, maintaining a high clinical index of suspicion is essential for timely diagnosis.[4] Diagnosing aortitis is challenging due to the diverse causes, which require different treatments, and the difficulty distinguishing between various types of the condition. Therefore, multimodality cardiac imaging plays a central role in the diagnosis, risk stratification, and management of aortic diseases and is strongly recommended by current guidelines.[5] Herein, we report a case of a patient with prosthetic valve endocarditis after aortic valve replacement, complicated with infectious aortitis, multiple embolic lesions, and death.
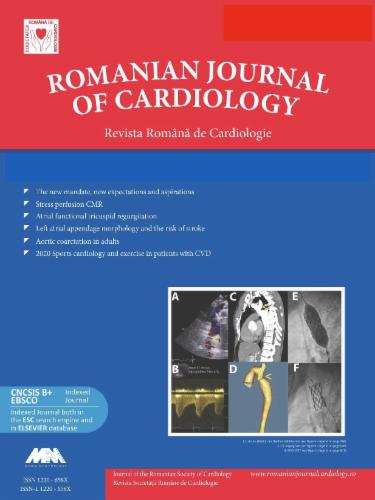
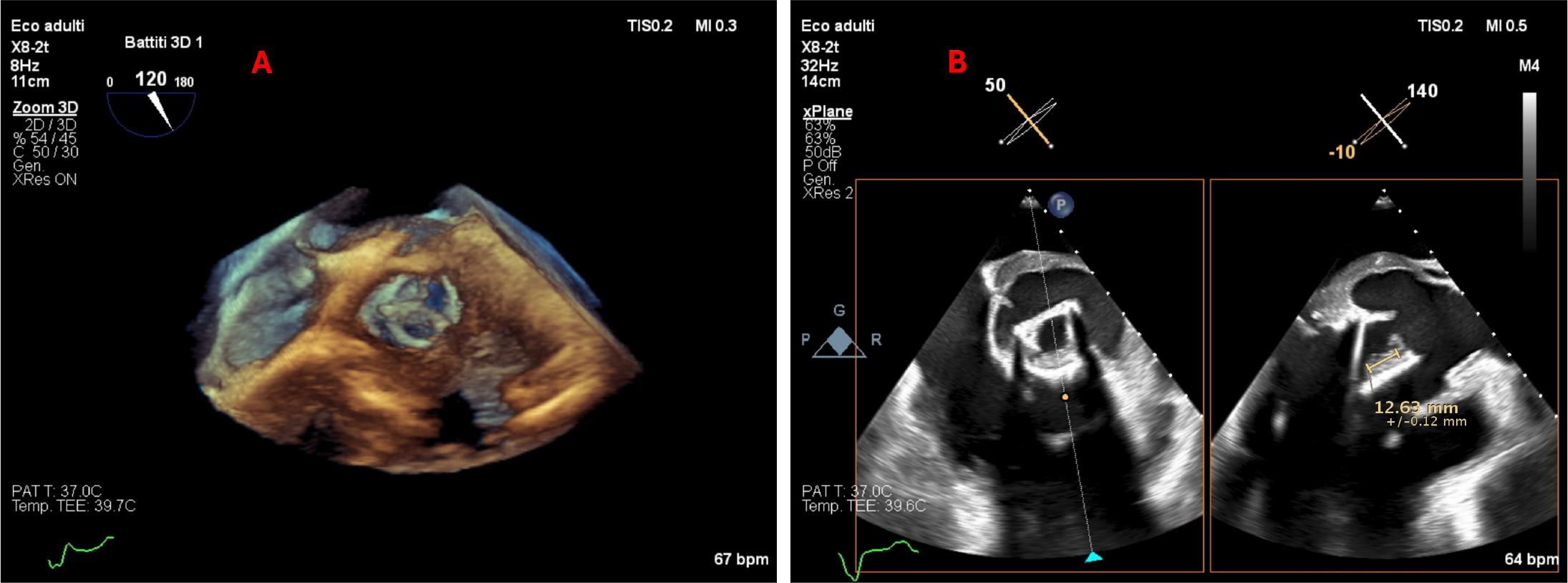
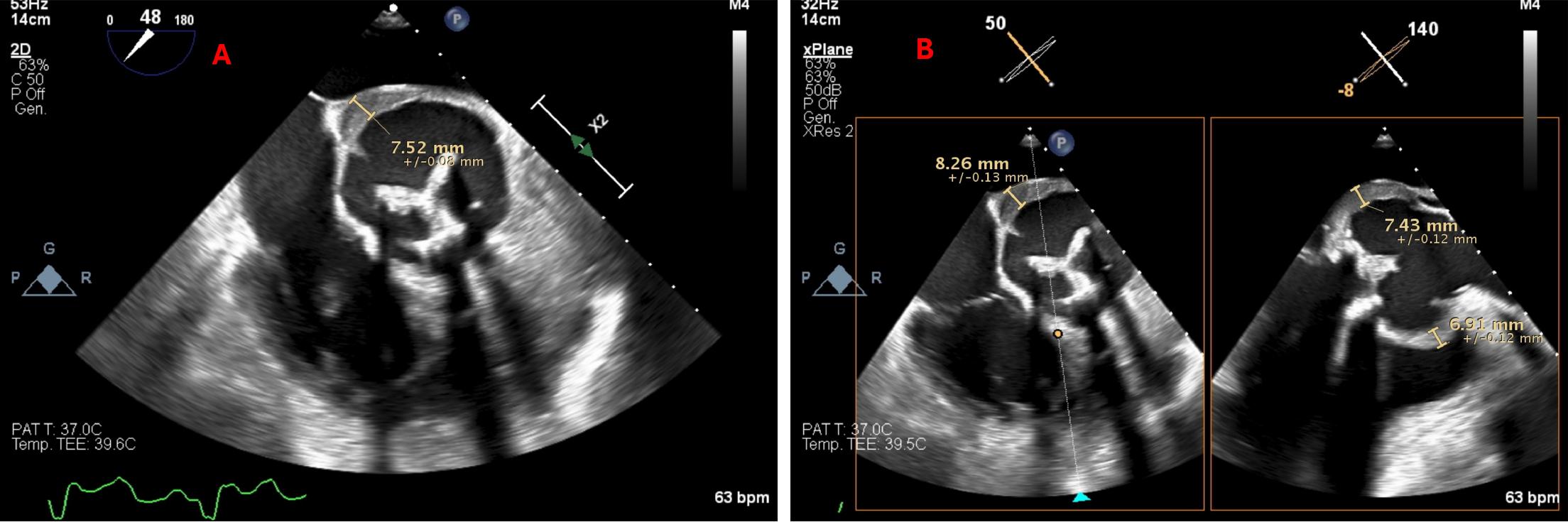
An 81-year-old man was admitted to the Emergency Department for fever, dysuria, and worsening ankle swelling. His medical history was significant for urinary tract stones, hypertension, paroxysmal atrial fibrillation, previous pulmonary thromboembolism, dilated cardiomyopathy, and aortic valve bioprosthesis (Intuity 27 mm), which was implanted 7 years ago. Previous transthoracic echocardiography (TTE), performed one month before the current admission, revealed moderated left ventricular dilatation (end-diastolic volume of 92 ml/m2), moderated reduced left ventricular ejection fraction (LVEF of 38%), aortic bioprosthesis with a mean gradient of 17 mmHg, and normal function of the right ventricle. The patient was recently treated for a genitourinary infection with cefixime for 10 days. He was on chronic treatment with rivaroxaban, amiodarone, beta-blocker, angiotensin-converting enzyme inhibitor, furosemide, and antialdosterone therapy. In the emergency department, his blood pressure was 105/77 mmHg, his pulse was 98 beats per minute, his respiratory rate was 20 breaths per minute, his oxygen saturation was 89% while breathing ambient air, and his temperature was 37.4 °C. Laboratory tests revealed neutrophilic leukocytosis, moderate anemia (Hb 8.2 g/dl), severe hypokalemia, NT-proBNP of 8.628 ng/L, and high values of C-reactive protein (11 mg/dl). Urinalysis revealed numerous bacteria, leukocytes, and erythrocytes. The chest X-ray demonstrated bilateral pleural effusion. The patient was admitted to the Internal Medicine ward with suspicion of genitourinary infection recurrence and consecutive congestive heart failure. Amoxicillin and ciprofloxacin were started with potassium administration. The TTE was performed and highlighted a hyperechogenic mass of approximately 18 mm on the aortic bioprosthesis with mild stenosis and negligible intra-prosthesis regurgitation, highly suggestive of prosthetic endocarditis. Therefore, transesophageal echocardiography (TEE) was performed and demonstrated the presence of vegetation on the aortic biological prosthesis with a diameter of 12x12 mm (Figure 1). Additionally, TEE revealed aneurysmal dilation of the aortic bulb measuring 55 mm, with an approximately 9 mm thickening of the aortic wall, observed anteriorly and posteriorly, extending to the sinotubular junction (Figure 2). The urinary cultures taken were positive for Enterobacter cloacae and Candida albicans. The blood samples were later positive for Staphylococcus aureus. The patient was transferred to the Cardiology department with the diagnosis of acute aortic prosthetic endocarditis complicated with infectious aortitis. Laboratory tests showed white-blood cells of 25.000/μL and a higher C-reactive protein (62 mg/dl) value. The infectious disease specialist recommended a combined regimen of antibiotics, with ampicillin 12 grams/day and ceftriaxone 4 grams/day. A whole-body computed tomography (CT) scan was performed to investigate potential embolic lesions and revealed multiple thromboembolic lesions affecting both the kidney and the spleen. Moreover, the thoracic CT confirmed the aneurysmal dilatation of the aortic root and inhomogeneous aortic mural thickening, both anteriorly and posteriorly, suggestive of infectious aortitis (Figure 3). The initial clinical evolution in the Cardiology ward was characterized by the appearance of abdominal pain, and soon after, the patient’s hospitalization was complicated by intestinal sub-occlusion but without urgent surgical indication. Therefore, a final diagnosis of aortic prosthetic endocarditis, infectious aortitis complicated with multiple thromboembolic septic emboli and intestinal sub-occlusion, was established. The clinical case was reviewed with the Heart Team, and given the patient’s frailty, high risk of intraoperative mortality, and potential for severe intestinal infarction, cardiovascular surgery was deemed prohibitive. Consequently, the patient was maintained on parenteral antibiotics to ensure complete eradication of the pathogen. Despite hemodynamic stability, on the 10th day of antibiotics adjustments, the patient’s condition rapidly deteriorated, culminating in cardiac arrest with no response to resuscitation efforts.
Transesophageal echocardiography using the three-dimensional (A), and the multi-plane method (B) to represent the aortic valve anatomy and identify the prosthetic valvular mass
Transesophageal echocardiography in short-axis view identifying (A) the anterior thickening of the aortic wall, and (B) using the multi-plane modality, the inhomogeneous material both anteriorly and posteriorly (maximum 9 mm), extending up to the sino-tubular junction, highly suggestive of aortic root aneurysm and aortitis
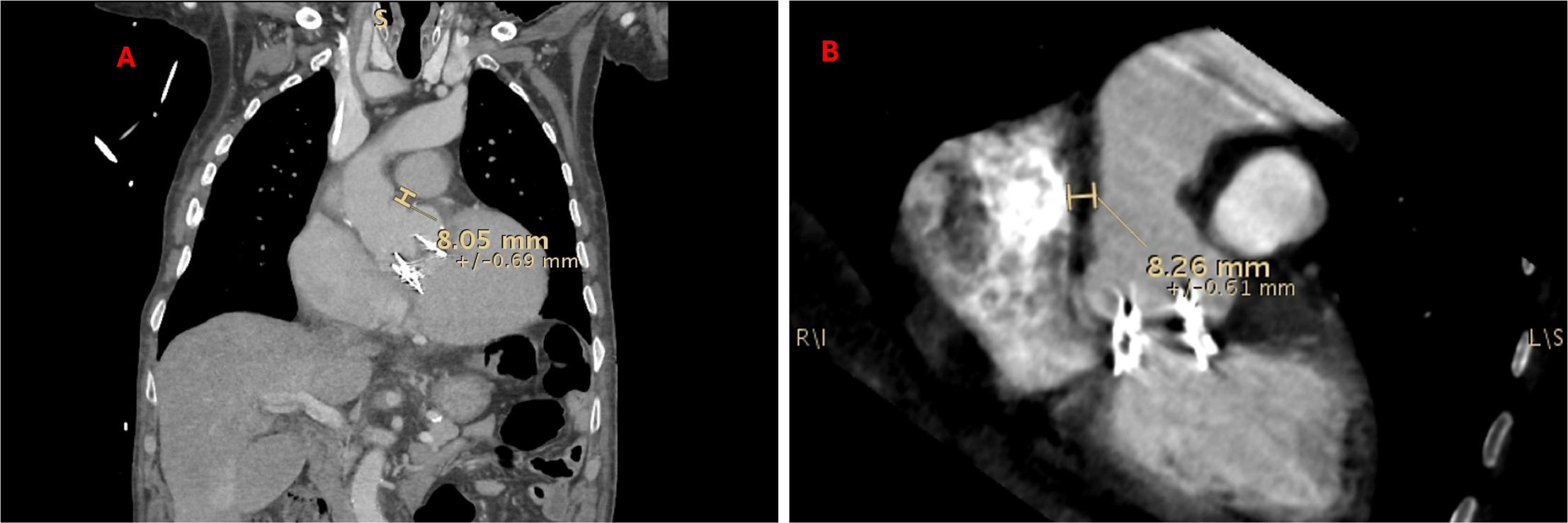
Computed tomography showing (A) in the frontal plane, the anterolateral thickening of the aortic wall; and (B) in the multiplanar reconstruction, depicting the inhomogeneous material with the irregular contour of the aortic root posteriorly
This clinical case illustrates the complex course of a patient with a history of aortic valve replacement (AVR) who developed prosthetic valve endocarditis (PVE) complicated by infectious aortitis and multiple embolic lesions. The patient’s condition ultimately led to death, likely caused by the rupture of the aortic aneurysm secondary to the infectious process. To the best of our knowledge, this is the second documented instance in the literature of infective aortitis treated conservatively.
Infectious aortitis is an exceedingly rare clinical condition, underscored by the fact that only a few cases have been documented in medical literature worldwide. In a nationwide population-based study, aortitis was found in 6.1% of adults who underwent pathological examination after the resection of the ascending aorta.[6] Factors predicting inflammation included connective tissue disease, diabetes, advanced age, and aortic valve pathology.[6] The risk factors for the presented clinical case include advanced age and the aortic prosthetic valve, with slightly elevated transvalvular gradients.
Moreover, the presented clinical case emphasizes the late-onset prosthetic valve endocarditis (PVE) associated with infectious aortitis. The PVE several years after aortic valve replacement (AVR) is rare but is associated with a high mortality rate.[7] The FinnValve registry demonstrated no significant difference in the risk of PVE between transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) over time.[7] However, the literature suggests that most cases occur in the first year post-AVR and late-onset is quite rare.[8] A Danish nationwide study included 2,632 TAVI and 3,777 SAVR patients and over an average follow-up of 3.6 years, 4.4% of TAVI patients, and 4.9% of SAVR patients developed PVE. The median time to PVE hospitalization was 352 days for TAVI (25th to 75th percentile: 133 to 778 days) and 625 days for SAVR (25th to 75th percentile: 209 to 1,385 days).[8]
Similar to other arterial conditions, aortic diseases may remain silent for a considerable period before becoming symptomatic.[9] The onset of AAS often serves as the initial presentation. Prompt diagnosis of suspected infectious aortitis is crucial, followed by the initiation of intravenous antibiotics targeting the most likely pathogen organism.
Differentiating infectious conditions from non-infectious aortic pathologies can be challenging as both endocarditis and aortitis are considered extraordinary mimics of clinical medicine. However, a combination of clinical, laboratory, echocardiographic, and radiological findings may be decisive.[10] Baseline patient characteristics, including older age, recent genitourinary infection, and prosthetic aortic valve, are leading risk factors for infective endocarditis for our patient. Clinical signs and symptoms may not always suggest endocarditis and infectious aortitis, especially in cases without concomitant aortic aneurysm or dissection.[11] Fever and thoracic or back pain may be evident but are neither specific nor particularly sensitive. Laboratory findings may similarly be of limited value, with the notable exception of bacteremia, which should prompt a search for an infectious source when detected.
Therefore, a multimodality imaging approach is needed when a high index of suspicion exists.[11] In our case, TTE was performed to investigate the cause of acute heart failure, which was fundamental to initially suspect the diagnosis of endocarditis.[12] The vegetation discovered, a fixed mass adherent to the prosthetic aortic valve, was a typical red flag of endocarditis.[11,13] According to the European Society of Cardiology guidelines, TEE should be performed to ensure a better characterization of the valve anatomy and extension of the vegetation.[11] The TEE revealed the aortic wall involvement and confirmed the diagnosis. Nevertheless, CT plays a key role in diagnosing, stratifying risk, and managing aortitis by enabling the identification of the affected segment by assessing the maximal diameter of dilatation and, in specific instances, detecting contrast extravasation.[14] Characteristic findings indicating aortitis on CT scans include aortic mural thickening, periaortic soft tissue nodularity or fluid accumulation, saccular aneurysms, and gas within the aortic wall.[9] CT imaging significantly impacts the investigation, management, and long-term monitoring of the disease, as well as prognosis.[1,15] For our patient, the CT examination provided improved spatial resolution for characterizing prosthetic leaflets, identifying aortic vegetation, and visualizing the extent of the inflammatory infectious process involving the aortic wall. Moreover, because of the aortic aneurysm, accompanied by significant intramural heterogeneous thickening suggestive of active inflammation, the patient’s risk of acute aortic rupture was substantially heightened. Additionally, as previously mentioned, the CT scan visualized multiple thromboembolic lesions, aiding clinicians in decision-making.
Although surgical treatment is considered the optimal approach for infectious aortitis, there is a mortality rate of 17% in patients without previous cardiac surgery.[1,4] Given the current lack of comprehensive data to guide treatment decisions, it is essential to thoroughly evaluate the advantages and disadvantages of each treatment option on an individual basis. In our case, the frailty of the patient, the presence of multiple thromboembolic lesions, and the high risk of intestinal ischemia during the surgery made cardiovascular intervention prohibitive. Indeed, surgical intervention for infectious aortitis is extremely complex, with major concerns regarding infection control, complete resection of infected tissue, aseptic grafting, and prevention of recurrent infection. Ideally, patients should achieve clinical remission before undergoing elective repair of an aortitis-related aneurysm.[1]
Therefore, effective antibiotic therapy is mandatory.[11] Nevertheless, as previously noted, the CT scan revealed a complex infectious aortitis with a high risk of aortic rupture. Even though surgical intervention may be indicated solely to prevent aneurysmal rupture, the patient’s current condition was deemed too high-risk for complex surgical intervention, as discussed in the Heart Team. Unfortunately, despite the aggressive antibiotic regimen, the clinical condition of our patient deteriorated rapidly, leading to cardiac arrest and death. This suggests that the most likely cause of death was aortic rupture.
The current clinical case presents a challenging scenario of prosthetic valvular endocarditis, complicated by infectious aortitis, an aortic root aneurysm, and multiple thromboembolic lesions in a patient considered high-risk for cardiovascular intervention, ultimately resulting in death. Infectious aortitis continues to pose a significant mortality rate despite the availability of multimodal imaging techniques that allow a comprehensive approach and rapid diagnosis.