Aortic stenosis (AS) is one of the most common valve diseases after mitral regurgitation, being associated with high mortality and morbidity in the absence of early diagnosis and optimal treatment [1]. Most commonly, AS is associated with the degenerative calcific process, but congenital structural disease or rheumatic heart disease can cause it. Valvular narrowing with hemodynamic obstruction leads to the left ventricle (LV) hypertrophy and remodeling, followed by heart failure and death [2,3].
Currently, no pharmacotherapies are proven to slow the progression of AS. Therefore, TAVI or surgical aortic valve replacement (SAVR) remain the only options for AS treatment. According to European Society of Cardiology and American College of Cardiology/American Heart Association guidelines, TAVI represents the first line of treatment for frail individuals with symptomatic severe AS who are at high surgical risk. [4,5]. Despite its success, TAVI carries inherent complications, the most commonly being coronary obstruction, myocardial infarction, conduction abnormalities, stroke, bleeding, acute kidney injury, valve malposition, and paravalvular regurgitation [6]. Moreover, limited TAVI durability due to bioprostheses degeneration and failure may require further interventions [7]. Proven bioprosthetic valve thrombosis was associated with early degeneration in a significant number of patients[8]. Also, subclinical aortic valve leaflet thrombosis characterized by thickening and reduced motion was more frequent in transcatheters than in surgical valves and may be linked to early bioprosthetic deterioration [9,10]. TAVI-in-TAVI has become an alternative procedure for patients deemed at high risk for surgical intervention with good long-term outcomes [11].
We present the case of an elderly patient who underwent a successful TAVI-in-TAVI for a degenerated bioprosthetic valve with severe stenosis. An excellent result was achieved with the reduction of transaortic gradients and improvement in functional NYHA class without post-procedural complications. This case highlights the importance of proper patient selection using multimodality imaging and suggests the need for TAVI-in-TAVI to become an available and safe option for the management of failed bioprosthesis valves.
An 83-year-old woman was admitted to our department for dyspnea with minimal exertion, palpitations, and fatigue. The patient has a medical history of coronary artery bypass graft (CABG) at age 71 with the left internal mammary artery grafted to the left anterior descending artery (LAD). Additionally, eight years later, she underwent a percutaneous coronary intervention of the LAD when the graft was found to be occluded. In 2018, at age 78, she was diagnosed with symptomatic severe AS. Transthoracic echocardiography showed a heavily calcified aortic valve with a limited opening (Supplementary material online, Video 1) and a mean pressure gradient of 61 mmHg (Figure 1A). According to current guidelines, she underwent TAVI using a bioprosthetic valve (Edwards Sapien 23 mm) without complications during or after the procedure. Post-procedural echocardiography revealed excellent performance of the bioprosthetic aortic valve (Supplementary material online, Video 2), demonstrating a low trans-prosthetic gradient (Figure 1B). There was a significant and sustained drop in BNP from 2528 pg/mL preTAVI (September 2018) to 88 pg/mL (February 2020). Further evolution was favorable until four years later (November 2022), when she presented progressive worsening of heart failure symptoms, in spite of optimal heart failure treatment, with an NTproBNP of 1368 pg/mL.
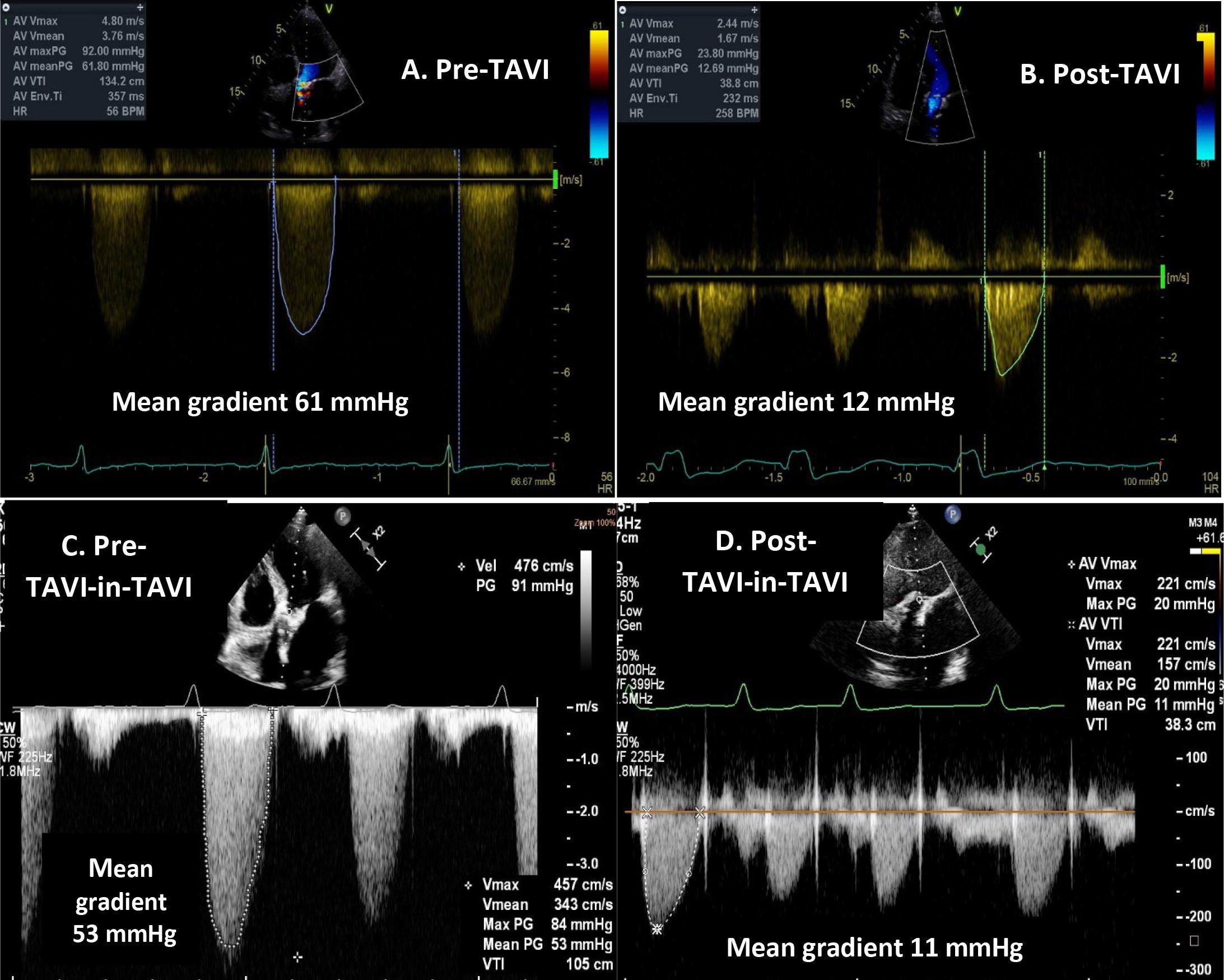
Evaluation of aortic valve function with continuous-wave Doppler echocardiography before transcatheter aortic valve implantation (A), after transcatheter aortic valve implantation (B), before TAVI-in-TAVI (C), and after TAVI-in-TAVI (D).
Physical examination revealed an optimal blood pressure of 120/70 mmHg and heart rate of 80 beats per minute, arrhythmic heart sounds with a grade 4/6 systolic ejection murmur over the aortic area radiating to the carotid arteries. The electrocardiogram showed atrial fibrillation, and the heart rate was 80 beats/min, with no electrical signs of myocardial ischemia. Transthoracic echocardiography revealed a severely calcified bioprosthetic valve with restricted motion of both the right and left coronary cusps, a mean gradient of 58 mmHg, iAVA 0.26 cm2/m2 (Figure 1C). Additionally, the left ventricle ejection fraction was preserved (LVEF 55%), with impaired LV relaxation, moderate mitral, and tricuspid regurgitation with PASP estimated at 40 mmHg.
Considering the history of CAD, a coronary angiography was performed and showed no restenosis of the stent in the LAD and no additional coronary lesions (Figure 2).
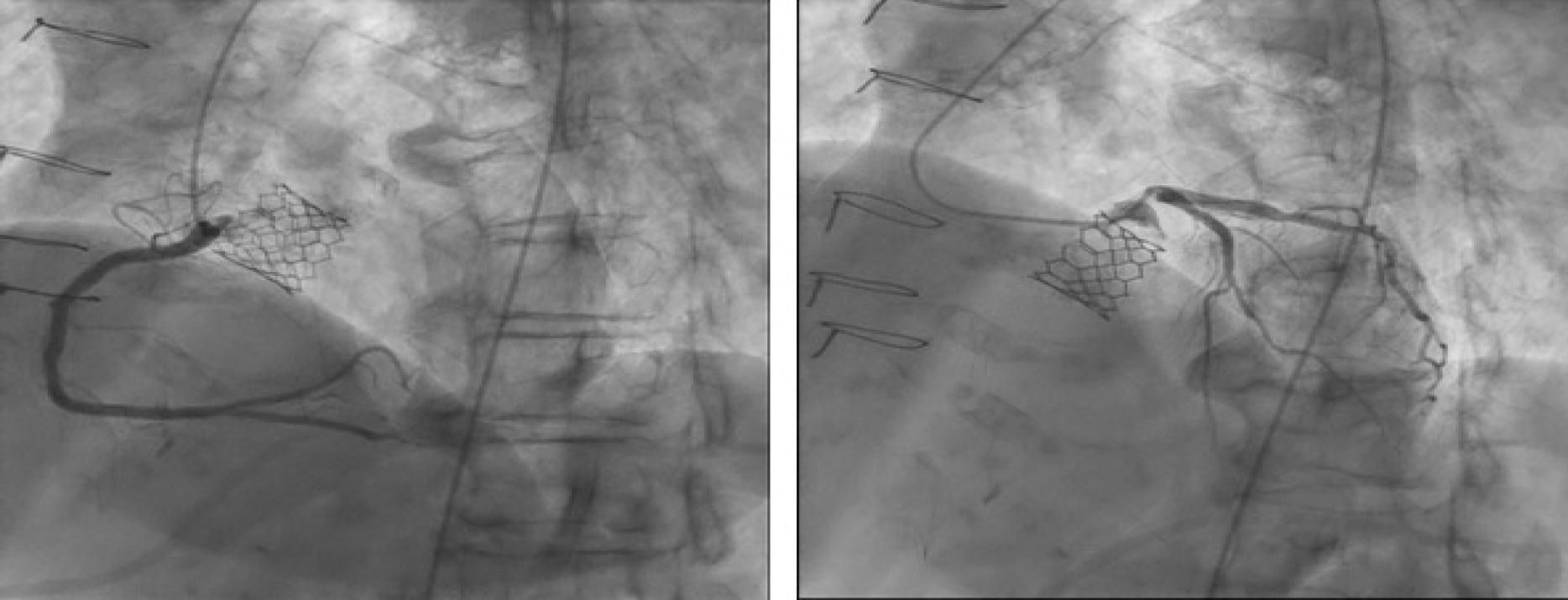
Coronary angiography performed in 2022 showed no coronary lesions. The stent of the first Edwards Sapien aortic valve implanted at TAVI can be seen.
The utility of multimodality imaging in the selection and implantation of the most appropriate prosthesis and assess the risk for coronary obstruction is well established and included for our case transesophageal echocardiography (TEE) and contrast-enhanced computed tomography (CT) to demonstrate the mechanism of valve restenosis.
TEE (Figure 3) showed structural valve degeneration with thickened leaflets and restricted motion of both the left and right coronary cusps, thickening, and calcification of the bioprosthesis valve (Supplementary material online, Video 3), but there was no sign of valvular thrombosis or infective endocarditis. Three-dimensional imaging of the aortic valve confirmed reduced leaflet mobility and limited opening of the aortic valve (Supplementary material online, Video 4).

TEE showed structural valve degeneration with restricted motion of both the left and right coronary cusps (LCC and RCC respectively) and limited opening of the aortic valve, seen here in systolic frames of the 2D and 3D views of the aortic valved.
Pre-procedural evaluation included contrast-enhanced CT, which identified significant calcification of the three leaflets with reduced mobility, particularly affecting the right and left coronary cusps, with limited opening and incomplete closure of the aortic valve. The aortic valve annulus area was 3.98 cm2, the ascending aorta diameter was 36.3 mm, and the distance from the coronary ostium to the aortic valve annulus (coronary height) was 12 mm, which is adequate for safely performing the ViV procedure (Figure 3). Additionally, the CT scan excluded the presence of a thrombus or endocarditis.
With EuroSCORE II of 10.3%, the patient was deemed a high risk surgical candidate and the Heart Team decided that TAVI-in- TAVI was the best treatment option. Using femoral approach, an 23 mm Edwards Sapien 3 valve was implanted into the degenerated first implanted Edwards Sapien bioprosthesis. X-ray fluoroscopy and angiography confirmed a fully expanded, well-seated transcatheter prosthetic aortic valve (Supplementary material online, Video 5).
Transthoracic echocardiography showed a significant reduction of trans-prosthetic pressure gradient to 31/15 mmHg with minimal paravalvular regurgitation; there were no wall motion abnormalities or pericardial effusion. The chest x-ray revealed a fully expanded aortic valve-in-valve, without pleural effusion or signs of congestive heart failure (Figure 6). The patient had an immediate improvement in symptoms, and the post-procedural course was uneventful. The patient was discharged home three days post-procedure. After one year of follow-up, echocardiography showed good functioning of the bioprosthetic aortic valve with low trans-prosthetic gradient (Figure 1D), a decrease in BNP levels, and the patient was able to perform daily activities without any assistance.
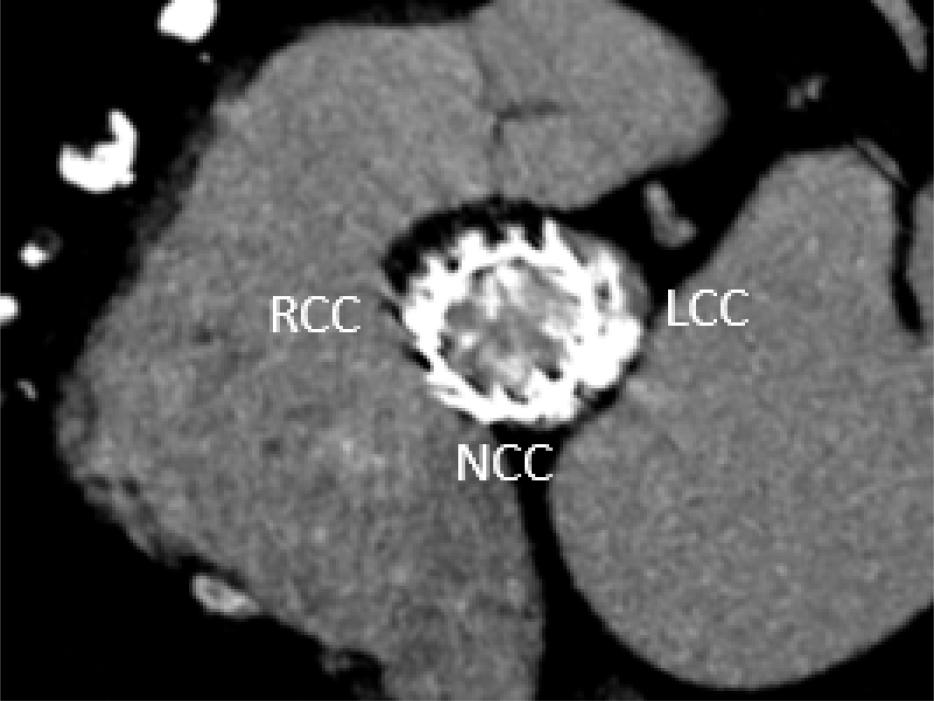
Pre-TAVI-in-TAVI Cardiac CT showed calcification of the three biologic prosthesis leaflets, with reduced mobility mainly of the right and left coronary cusps, with limited opening during ventricular systole (picture taken from systolic frame).
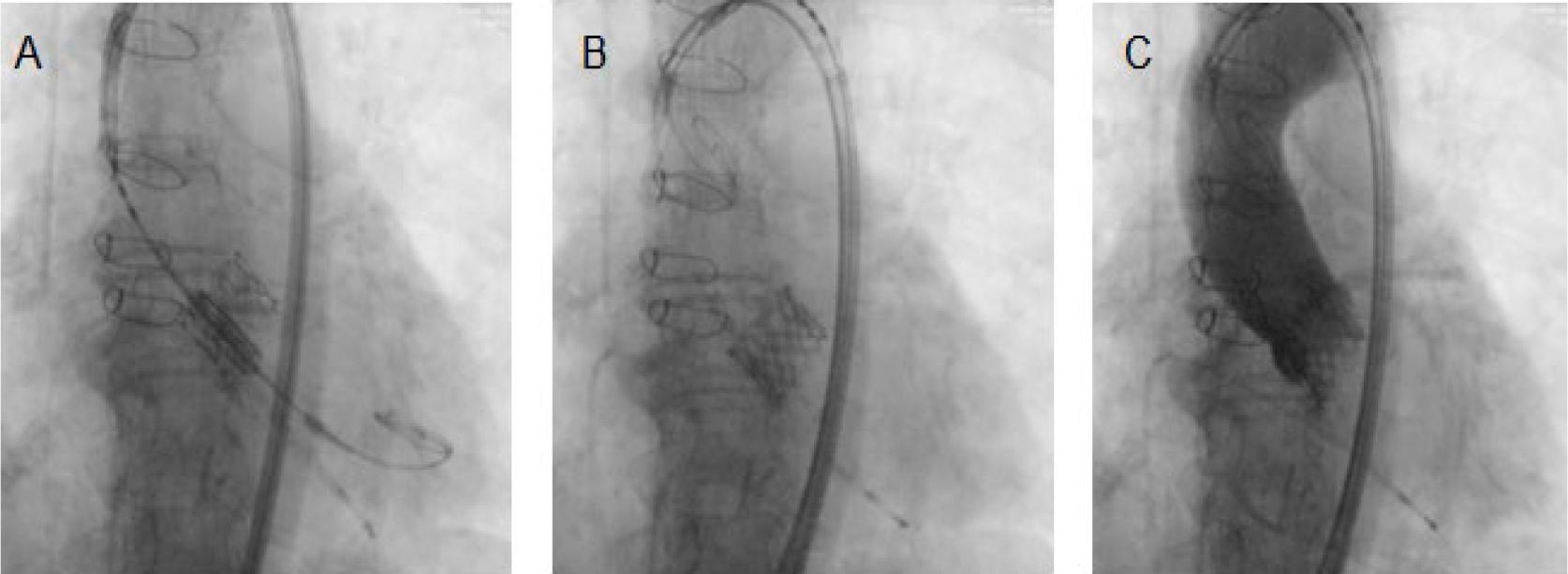
TAVI-in-TAVI with an Edwards Sapien 3 valve. (A) Using a balloon valvuloplasty, a 23 mm Edwards Sapien 3 valve was inserted into the degenerated 23 mm Edwards Sapien 3 bioprosthesis. (B) Expanded new Edwards Sapien 3 valve bioprosthesis. (C) X-ray fluoroscopy after transcatheter aortic valve deployment demonstrating a fully expanded, well-seated transcatheter prosthetic aortic valve.
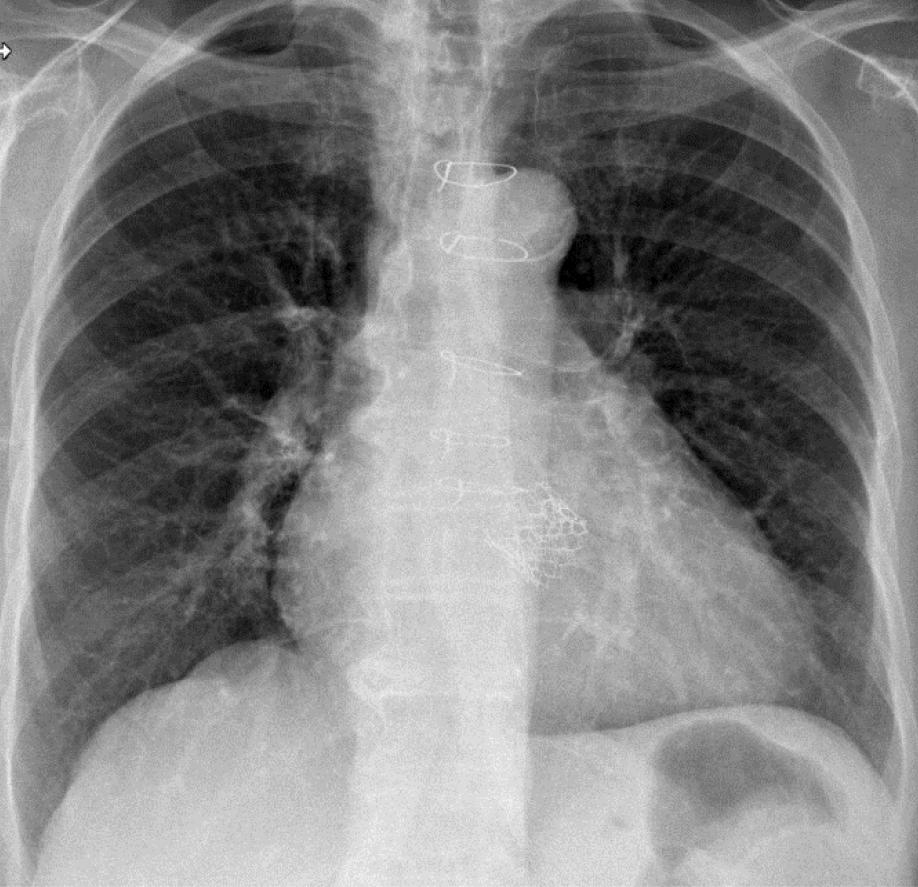
Chest X-ray after TAVI-in-TAVI reflecting the complex medical journey of the patient: sternum wires from the first CABG surgery and the two prosthetic stents from the first TAVI and the second TAVI-in-TAVI superposed in the center of the X-ray.
AS is a strongly age-related health burden with a prevalence of 2% among people in their 60’s but rising to 10% in the eighth decade of life. Most commonly, AS is the consequence of a degenerative process with extensive valve calcification due to aging or a congenitally abnormal valve morphology, such as bicuspid aortic valve or rheumatic heart disease [12]. The pathophysiological mechanism of AS is now recognized as an active process similar to atherosclerosis. Initial endothelial injury, attributed to common risk factors such as old age, hypertension, smoking, hypercholesterolemia, and diabetes, facilitates the infiltration of low-density lipoproteins (LDLs) and lipoprotein(a), subsequently triggering a local inflammatory response and contributing to fibrosis and calcification of the aortic valve. Morphological adaptation of LV to the valvular narrowing includes maladaptive ventricular remodeling followed by heart failure and, ultimately, death. BNP and highly sensitive troponin are non-specific biomarkers used for detecting myocyte injury and measuring ventricular stretch due to AS, thereby predicting an increased risk of death [3,13]. In our patient, there was a strong correlation between the BNP level and the progression of aortic valve disease. A second peak of BNP was observed when the aortic prosthesis malfunctioned, followed by a subsequent decrease after the TAVI-in-TAVI procedure.
Currently, no pharmacotherapies are recommended for slowing the progression of AS. However, observational studies have suggested that well-known therapeutic agents such as angiotensin-converting enzyme inhibitors and angiotensin receptor blockers or statins, but also novel pharmacological interventions including lipoprotein(a) lowering therapies, vitamin K supplementation or inhibitors of osteoclast-mediated bone resorption may improve valvular dysfunction by reducing inflammation, fibrosis, and calcification. Unfortunately, data from randomized controlled trials proving the beneficial effects of these therapies are lacking, and the only treatment option for AS remains the valve replacement [14].
Therefore, aortic valve replacement has been the definitive choice of therapy. Actually, TAVI is considered an alternative to SAVR for the treatment of severe AS with positive outcomes, but the life expectancy of these patients might exceed the durability of bioprosthetic valves with potential requirements for subsequent TAVI-in-TAVI procedures. The decision to refer for aortic valve replacement is currently based on the severity of AS and the presence of AS-related symptoms or signs of left ventricular systolic dysfunction [15].
Both TAVI and SAVR are associated with improving clinical status and survival [16]. The indications for TAVI have expanded from elderly patients at prohibitive surgical risk to younger and even low-surgical-risk patients due to increased operator experience and improved devices used for this procedure, which dramatically reduced complications [17].
Moreover, the NOTION trial found no significant differences regarding the risk for all-cause mortality, stroke, new-onset atrial fibrillation, or permanent pacemaker implantation after eight years of follow-up in patients at low surgical risk who are undergoing TAVI versus SAVR [18]. The management of asymptomatic severe AS remains a controversial decision. Despite the relatively good prognosis of asymptomatic patients, the risk of late referral associated with irreversible organ damage, life-threatening events, and increased mortality remains the major limitation of watchful waiting. On the other hand, early intervention increases the risk of complications such as prosthetic valve thrombosis or endocarditis, paravalvular regurgitation, atrioventricular conduction abnormalities, and structural valve deterioration with earlier reintervention. Current guidelines recommend a careful weighing of potential risk vs. benefit with the mention that improvement of catheter interventional techniques may change the threshold to intervene in asymptomatic patients [19].
With the increasing use of bioprosthetic valves that are prone to degeneration, the need for reintervention is expected to grow. While biological heart valves offer outstanding hemodynamic performance and eliminate the need for lifelong anticoagulation therapy, there remains a notable concern regarding their durability. The main factors contributing to the dysfunction of biological heart valves include structural valve degeneration, thrombosis, and endocarditis [20]. Structural valve degeneration, likely the most prevalent form of biological valve dysfunction, is marked by enduring intrinsic alterations in the valve structure, such as leaflet tear, calcification, and pannus deposition, leading to stenosis or intra-prosthetic regurgitation. The mechanisms beyond structural changes involve high mechanical stress, local inflammation, macrophage infiltration leading to fibro-calcifying processes, and the promotion of a pro- thrombotic state [21]. Several registry studies have documented a cumulative incidence of structural valve degeneration ranging from 4.8% to 13.3% in the 5 to 7 years following TAVI [22]. In our patient, symptoms and discovery of a high transprosthetic gradient occurred four years after the index-TAVI.
TAVI-in-TAVI has become an effective and safe option with noticeably improved outcomes, recommended for the treatment of degenerated aortic bioprosthesis in patients with prohibitive risk for surgical redo. The use of TAVI expanded with the utilization of valve-in-valve techniques for a diverse subset of patients, including TAVI within TAVI, TAVI within a degenerated surgically implanted bioprosthesis, or even TAVI-in-TAVI-in-surgical bioprosthesis. The TAVI-in-TAVI procedure is intricate, with numerous potential challenges. Thus, it should be carried out in high-volume centers by experienced staff due to the significantly elevated risk of peri- and post-procedural complications compared to TAVI on native valves [11,23]. The main issues of TAVI-in-TAVI include malposition, elevated post-procedural gradients, prosthesis-patient mismatch, coronary obstruction, and leaflet thrombosis [24]. The next challenge will be improving implanting devices and techniques of TAVI-in-TAVI to eliminate adverse events completely.
Over the last twenty years, less invasive interventions have changed the natural history of AS. TAVI has become the preferred therapeutic strategy for aortic valve replacement in patients with severe AS aged 75 years or older and in those who are at high surgical risk. However, larger TAVI populations and longer intervals since the index intervention led to more cases of bioprosthesis degeneration, for which TAVI-in-TAVI appears as a very promising treatment option with satisfactory short and long-term results similar to those with a single valve.
The presented case is the first successful TAVI-in-TAVI performed in our Medical Centre and highlights the safety and efficiency of the procedure. Thus, the next challenge will be the improving of implanting devices and techniques to completely eliminate adverse events.