
The widespread application of coronary angiography has resulted in more frequent identification of congenital coronary artery anomalies and an improved understanding of the clinical significance of such anomalies [1,2]. Coronary artery anomalies are rare congenital abnormalities often found incidentally on conventional coronary angiogram or coronary computed tomography angiography. They may result in various clinical outcomes. Coronary artery anomalies may be abnormalities of the origin, course, or structure of the epicardial coronary arteries. An anomalous origin of one or more coronary arteries is detected in about 0.16–1.3% of patients undergoing coronary angiography [3,4,5,6,7,8].
The objective of this study was to investigate the prevalence of coronary artery anomalies, the clinical and laboratory characteristics of patients with coronary artery anomalies, and the outcomes at 1-year follow-up of these patients in a high-volume coronary interventional center in Romania.
To define the study population, we reviewed all coronary angiograms performed between 01.01.2014 and 31.12.2014. A total number of 5832 coronary angiograms were analyzed, and we identified 31 patients with coronary artery anomalies. We included in the study the patients with anomalies in the origin, course, and number of coronary arteries and with coronary fistulas. We excluded from the study population patients with myocardial bridging of coronary artery because they represent another category of patients that can erroneously raise the incidence of coronary artery anomalies. All clinical, laboratory, and angiographic data were recorded.
The annuary prevalence of coronary artery anomalies was 0.53% in our study population. Eighty-seven point four percent of the patients had origin and distribution anomalies, and twelve point nine percent of the patients had a coronary artery fistula. In 61% of cases the left coronary artery was anomalous and 39% of cases had an anomaly involving the right coronary artery (figure 1).
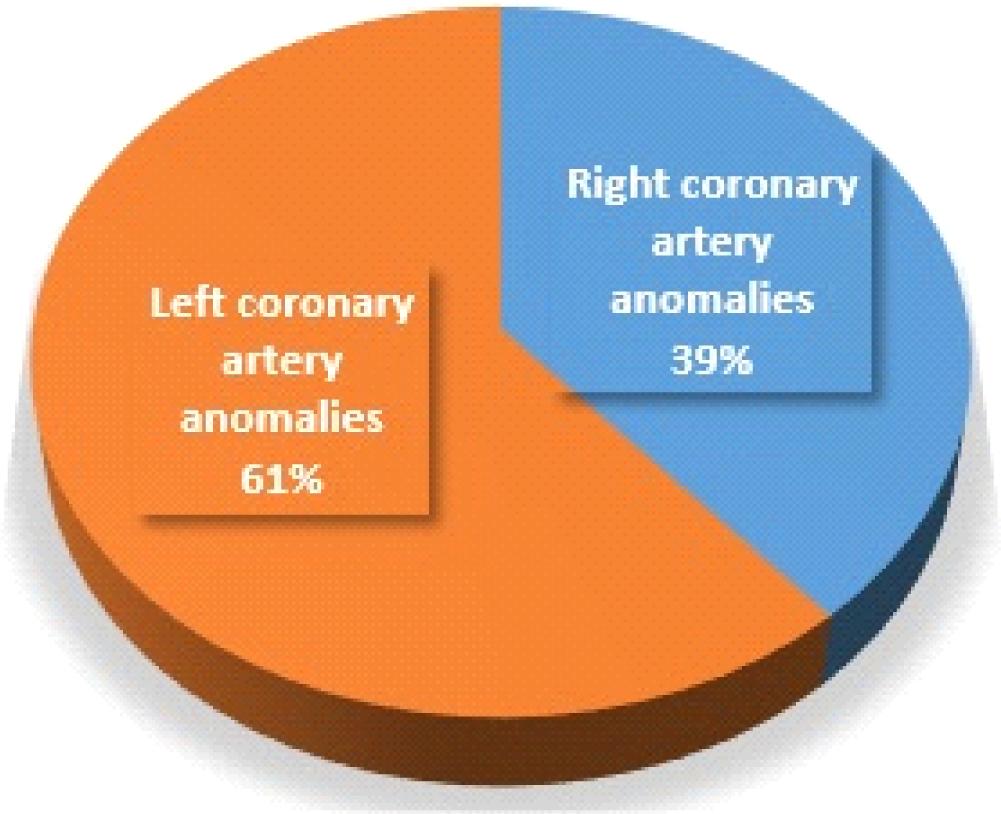
Frequency of left and right coronary artery anomalies.
The mean age at diagnosis was 65 years and 59% were male patients. Sixty-one point three percent of the patients underwent coronary angiogram due to atypical chest pain (table 1). The most common cardiovascular risk factors between patients with coronary anomalies were hypertension (77.4%) and dyslipidemia (64.51%). Sixteen point one percent of the patients with coronary anomalies had a previous myocardial infarction and twelve point nine percent presented with myocardial infarction, either ST segment elevation myocardial infarction (STEMI) or non-ST segment elevation myocardial infarction (NSTEMI).
Baseline clinical characteristics of patients with coronary anomalies
| • Age | 65 (42–81) | |
| • Gender | Female | 59% |
| Male | ||
| • Presenting symptoms | ||
| Typical chest pain | 32.25% | |
| Atypical chest pain | 61.29% | |
| No chest pain | 6.46% | |
| Presenting with STEMI | 6.45% | |
| Presenting with NSTE-ACS | 6.45% | |
| • Risk factors | ||
| Hypertension | 77.4% | |
| Diabetes | 16.12% | |
| Dyslipidemia | 64.51% | |
| Smoking | 25.8% | |
| • Underling cardiac problems | ||
| Previous myocardial infarction | 16.12% | |
| Previous coronary intervention | 25.8% | |
| Previous dilated cardiomyopathy | 19.35% | |
| Valvular heart disease (at least moderate severity) | 35.5% | |
STEMI – ST segment elevation myocardial infarction, NSTE-ACS – non-ST segment elevation acute coronary syndrome
Twenty-nine percent of the patients had significant coronary artery disease (figure 2). Most of the patients had no coronary lesions (58%). The most common coronary artery anomalies were the anomalous origin of left circumflex artery from the right coronary artery (38.71%) (figure 3) and the anomalous origin of right coronary artery from right coronary sinus of Valsalva (19.35%) (table 2) and the least common was anomalous origin of RCA from the LAD (0.017%) (figure 5). Eight (25.8%) patients underwent coronary revascularization by percutaneous coronary intervention (7 patients − 22.58%) or coronary artery bypass grafting (1 patient − 3.22%). No death or significant complication were recorded in the 31 patients during the 5 years follow-up.
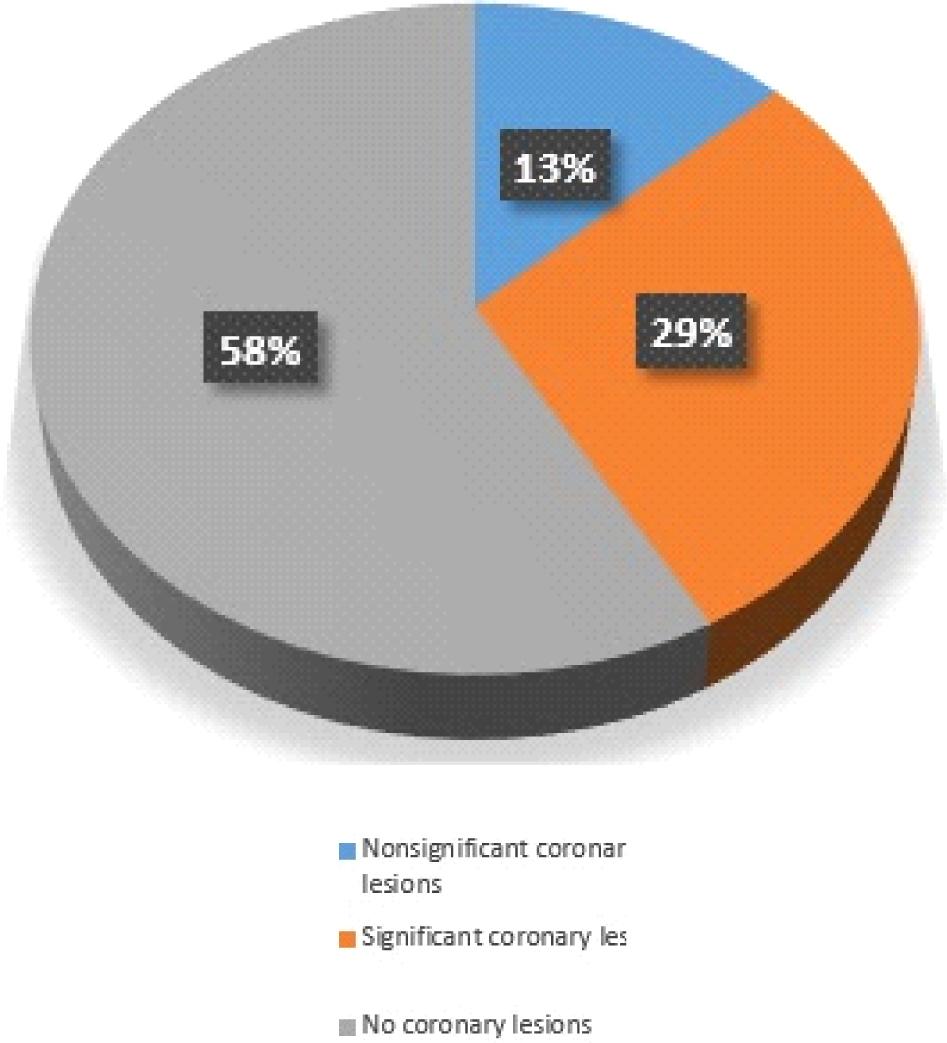
Types of coronary lesions between patients with coronary artery anomalies.

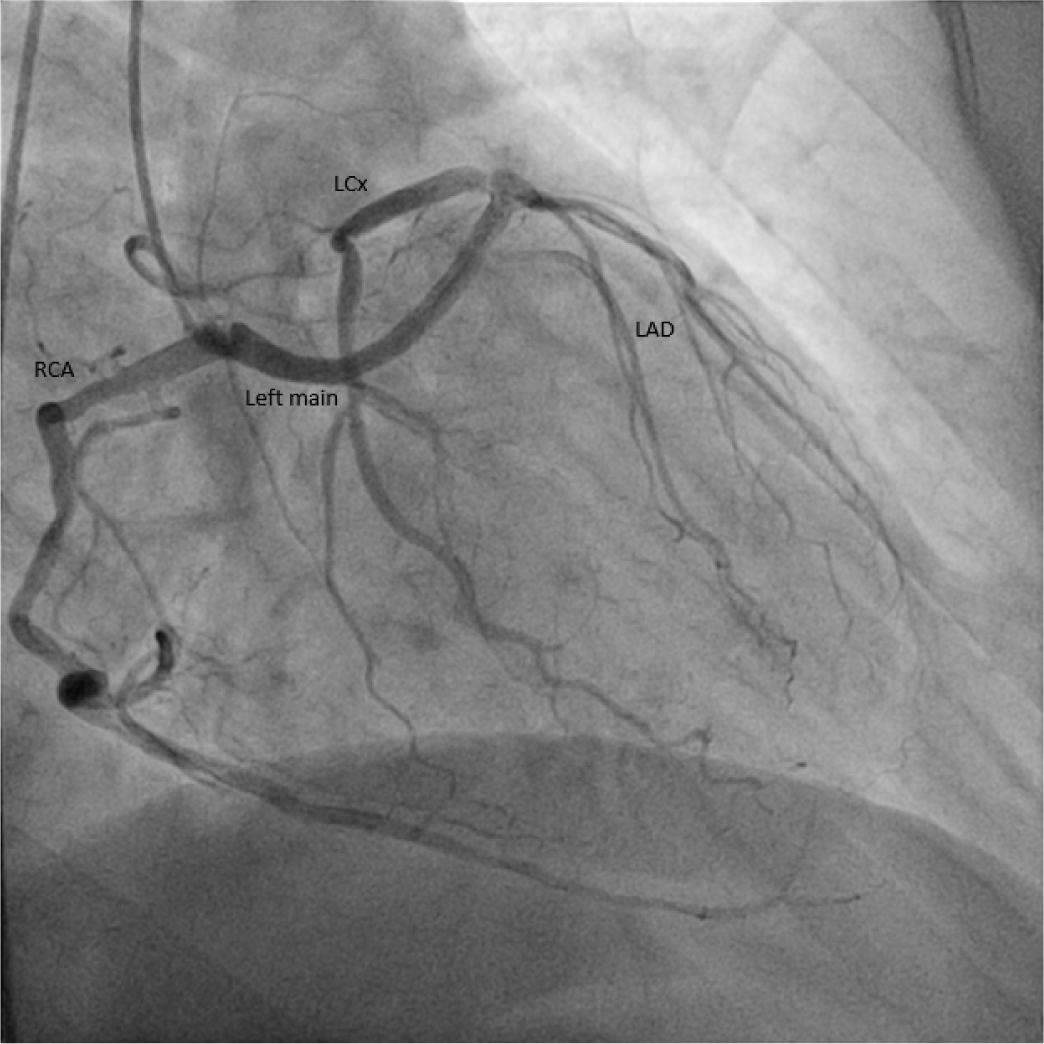
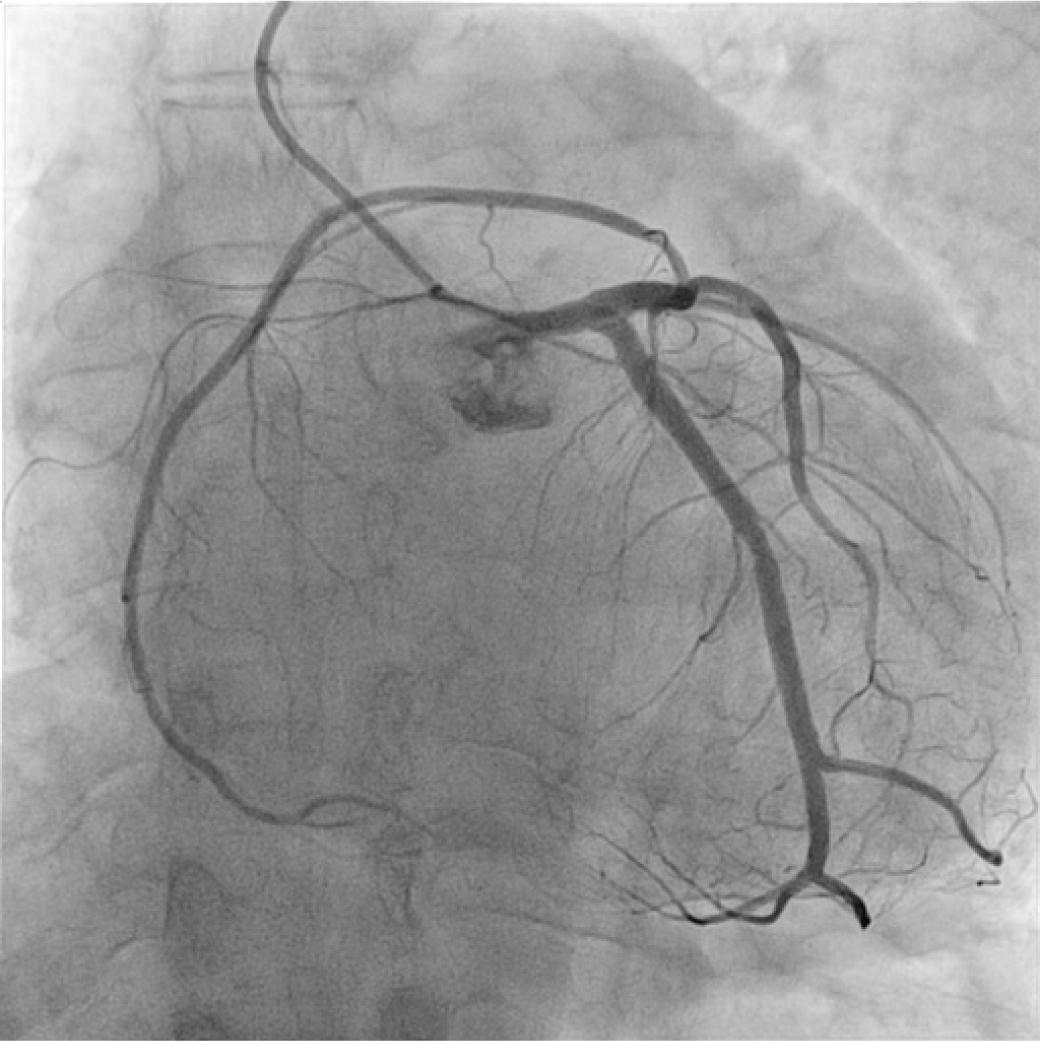
Anomalous origin of left circumflex artery from the right coronary artery.
Anomalous origin of left coronary artery from right coronary sinus of Valsalva [8].
Anomalous origin of right coronary artery from the left anterior descending artery.
Annuary incidence of different types of coronary artery anomalies
| Type of coronary artery anomaly | Number | Incidence among 5832 (%) | |
|---|---|---|---|
| Anomalous origin of LCx from the RCA | 12 | 0.205% | |
| Anomalous origin of RCA from right coronary sinus of Valsalva | 6 | 0.102% | |
| Anomalous origin of RCA from left coronary sinus of Valsalva | 3 | 0.051% | |
| Anomalous origin of LCA from right coronary sinus of Valsalva (figure 4) | 1 | 0.017% | |
| Fistulas | LCx to left atrium | 1 | 0.017% |
| LCx to pulmonary artery | 2 | 0.034% | |
| LAD to pulmonary artery | 1 | 0.017% | |
| Anomalous origin of marginal branch from right coronary sinus of Valsalva | 1 | 0.017% | |
| Anomalous origin of RCA from the LAD | 1 | 0.017% | |
| Anomalous origin of LAD from right coronary sinus of Valsalva | 1 | 0.017% | |
| Anomalous origin of LAD from the RCA | 1 | 0.017% | |
| Anomalous origin of LCx from right coronary sinus of Valsalva | 1 | 0.017% | |
LCx – left circumflex artery, RCA – right coronary artery, LCA – left coronary artery, LAD – left anterior descending artery
Among patients undergoing diagnostic coronary artery angiography, we found an overall incidence of congenital anomalous aortic origin of the coronary artery of 0.53%; this is in agreement with the 0.16–1.3% incidence reported in other series [3,4,5,6,7,8]. There was a slightly more male patients with coronary artery anomalies, possibly because the diagnostic coronary angiograms are performed more often in male patients compared to females.
In most studies, the most prevalent coronary artery anomaly was anomalous origin of right coronary artery, ranging from 31% to 79% depending on study population [3,4,5,6,7,8]. This is different from our study where the most common coronary artery anomaly was the anomalous origin of left circumflex artery from the right coronary artery (38.71%). The anomalous origin of right coronary artery was encountered in 19.35% of cases.
Garg et al. found that only 28% of their patients had evidence of atherosclerosis (significant stenosis of proximal vessel in 21% of the patients) [3]. Our study agrees with others; twenty-nine percent of the patients had a significant coronary artery stenosis of the anomalous artery or of a normal artery.
Most coronary artery anomalies are a benign finding during coronary angiogram. Although in some cases severe ischemia with sudden death can occur to the frank compression of the anomalous vessel between the aorta and pulmonary artery [9]. Hemodynamic changes during exercise may exacerbate disturbances in flow. In adults, ischemia may also be a consequence of atherosclerotic lesions within either normal or anomalous vessels. In our study 29% of the patients had significant coronary artery disease. Although the significant number of patients with coronary lesions, previous myocardial infarction, and myocardial revascularization, at five-year folllow-up no deaths were recorded. This in accordance with the principle that most coronary anomalies have a good prognosis.
The prevalence of coronary artery anomalies in this study was slightly lower but still similar to that of previous studies [5]. Different from others reports, the most common coronary artery anomaly was the anomalous origin of left circumflex artery from the right coronary artery. Angiographic recognition of these vessels is important because of their clinical significance and importance in patients undergoing coronary angioplasty or cardiac surgery. Most patients presented with atypical symptoms, and only a minority had coronary artery disease. In the context of no death or significant complication at 5-year follow-up highlights the benign prognosis of most coronary artery anomalies.