
Effective postoperative pain management is key to enhanced recovery after surgery. It directly influences patient satisfaction, morbidity, and overall outcomes. Despite advances in anesthesia and analgesia, postoperative pain remains common and distressing (1). Inadequate perioperative pain control triggers physiological stress, which can cause complications such as hemodynamic instability, delayed wound healing, pulmonary dysfunction, myocardial ischemia, and thromboembolic events (2,3). These issues prolong hospital stays, delay recovery, increase readmission, and raise healthcare costs.
Opioid analgesics have long been central to perioperative pain management. However, their use is limited by adverse effects such as nausea, vomiting, constipation, ileus, urinary retention, sedation, and respiratory depression. Concern about these side effects and dependency has led to the rise of multimodal analgesia. This approach combines different analgesics targeting distinct pain pathways to maximize relief and reduce opioid needs (4). Within this model, preemptive analgesia—administering agents before incision—has gained attention. By preventing central sensitization and reducing nociceptive amplification, preemptive analgesia can lower postoperative pain intensity and decrease the need for rescue opioids (5,6,7). This strategy enhances pain control, improves comfort, and limits the development of chronic pain (7). The best preemptive analgesic remains uncertain, despite studies of multiple regimens (8).
Tapentadol is a newer agent in multimodal and preemptive strategies. It works through two mechanisms: μ-opioid receptor agonism and norepinephrine reuptake inhibition. This provides strong pain relief with fewer typical opioid side effects. Tapentadol has about 32% oral bioavailability, acts within one hour, and has a half-life of 4 to 6 hours. These features make it suitable for short-term postoperative pain.
Clinical studies, including those conducted at the Mayo Clinic, have shown that tapentadol provides analgesia comparable to morphine but with superior tolerability and patient satisfaction. Moreover, multiple studies have confirmed its efficacy both as a preemptive analgesic and in managing moderate to severe acute and chronic pain (9, 10).
Despite its growing international use, local data on South Asian populations, particularly in Pakistan, remain scarce. To date, no randomized controlled trial has evaluated the efficacy of oral tapentadol as a preemptive analgesic in surgical oncology patients within this region. Understanding its role in local clinical practice is essential, given population-specific pharmacogenetics and variations in healthcare delivery. The present study was therefore designed to evaluate the analgesic efficacy and safety of preemptive oral tapentadol (75 mg) compared to placebo in patients undergoing conservative breast surgeries. The objective of this study was to assess postoperative pain intensity during the first four hours following surgery, the requirement for rescue opioid analgesia intraoperatively and postoperatively, and the incidence of adverse effects in the immediate postoperative period.
This prospective, double-blind, randomized controlled trial was conducted in Lahore from November 2024 to September 2025 by the Department of Anesthesia and Pain Management, Shaukat Khanum Memorial Cancer Hospital and Research Center. Ethical approval was obtained from the Institutional Review Board (IRB-23-20) before patient enrollment. Trial was registered on the online trial registry vide no. NCT07320781 (https://clinicaltrials.gov/).
Sample size was calculated using the data from Yadav et al.11 (2016). Their study reported postoperative analgesic needs of 13.3 ± 22.5 mg in the intervention group and 33.3 ± 33.0 mg in the control group. Allowing for a 10% dropout rate, 80% power, and 95% confidence, we needed 70 patients—35 in each group: Group A (tapentadol) and Group B (placebo). The trial followed CONSORT 2025 guidelines for transparency [Figure 1].
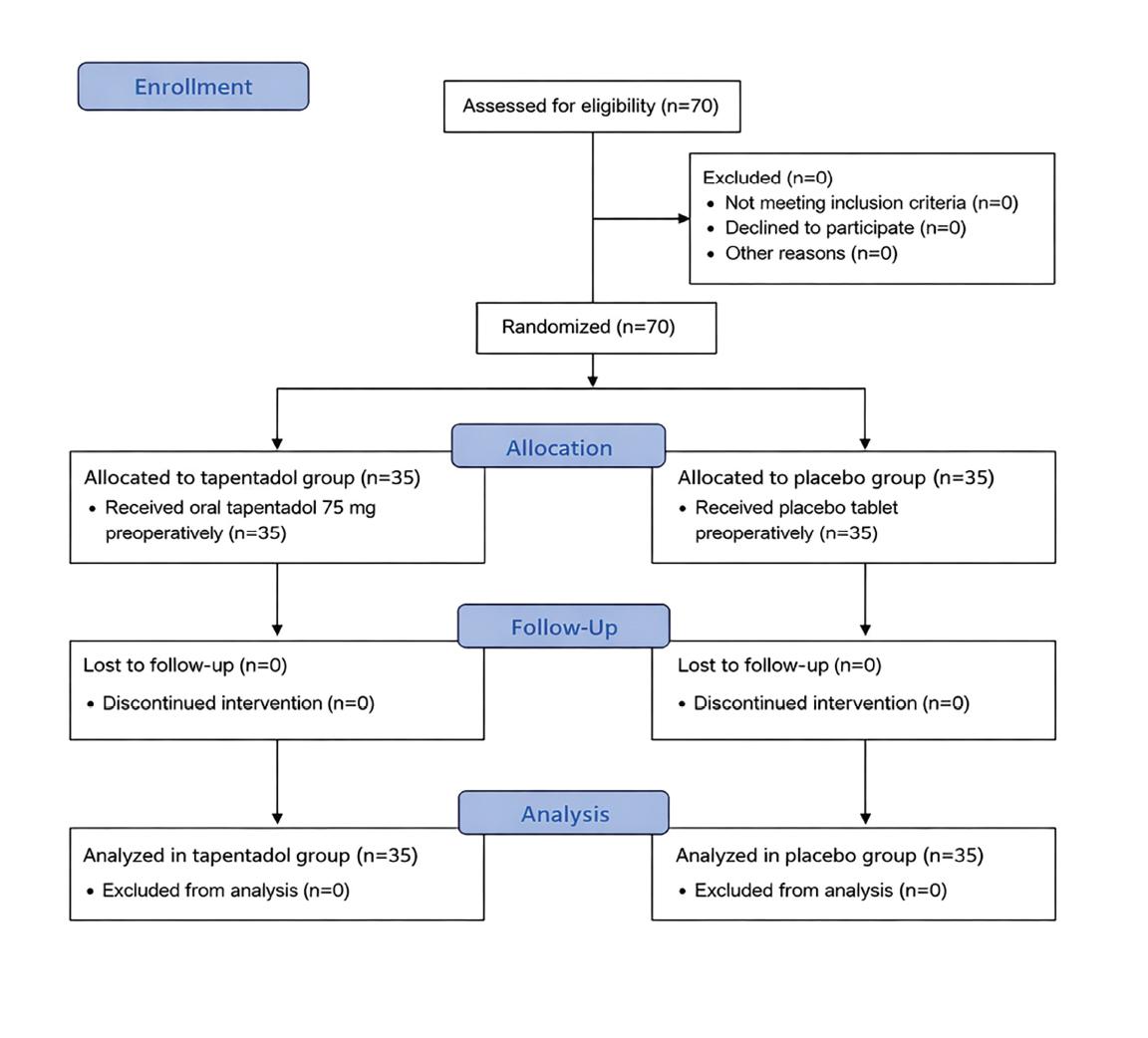
CONSORT flow diagram of participant enrollment, randomization, allocation, follow-up, and analysis in patients undergoing breast conservative surgery. Seventy participants were randomized equally to tapentadol and placebo groups, with no losses to follow-up.
A total of 70 female patients aged 18 to 60 years, classified as American Society of Anesthesiologists (ASA) physical status I or II, undergoing conservative breast surgery (lumpectomy or wide local excision) with or without axillary lymph node dissection, were enrolled through non-probability consecutive sampling. Patients with a body mass index greater than 35 kg/ m2, known drug allergies, or chronic kidney disease stage 3 or higher were excluded. A double-blind, two-operator technique was employed to ensure adequate blinding. Participants were randomly allocated into two equal groups using computer-generated randomization. Allocation concealment was achieved through sequentially numbered, sealed, opaque envelopes prepared by an investigator not involved in patient management. The study drugs were administered by an investigator who was not involved in subsequent intraoperative or postoperative assessment. Additionally, the anesthesiologist managing intraoperative care and the nursing staff in the post-anesthesia care unit (PACU) were blinded to treatment assignment.
One hour before induction of anesthesia, Group A received oral tapentadol 75 mg with a sip of water, while Group B received a placebo tablet containing sodium bicarbonate and peppermint oil 300 mg. The World Health Organization surgical safety checklist was completed upon entry to the operating room. Anesthesia was induced with intravenous midazolam 0.05–0.1 mg/kg and propofol 1 to 2 mg/kg. Sevoflurane was used for maintenance at a minimum alveolar concentration of 1.0–1.3. Airway management was achieved with a supraglottic device. Atracurium was used at the anesthetist’s discretion for muscle relaxation. All patients received intravenous diclofenac 75 mg and paracetamol 1 g unless contraindicated. Intraoperative morphine up to 0.1 mg/kg was administered for an increase in mean arterial pressure exceeding 20 percent from baseline and was documented.
After surgery, patients were transferred to the post-anesthesia care unit (PACU), which marked time zero. All patients remained in the PACU for four hours. Pain was assessed using the Numerical Rating Scale (0–10) at 1, 2, 3, and 4 hours postoperatively. Rescue analgesia consisting of intravenous morphine up to 0.1 mg/kg was administered when pain exceeded a score of 3. The time to first rescue dose, total morphine used intra and postoperatively (dose and number of patients), and side effects were documented.
Data were collected on a pre-designed pro forma and analyzed using Version 26 of the Statistical Package for the Social Sciences (SPSS). Continuous variables were assessed for normality using the Shapiro–Wilk test. Homogeneity of variances was evaluated using Levene’s test. Normally distributed variables were expressed as mean ± standard deviation (SD), and between-group comparisons were performed using the independent samples t-test. Welch’s t-test was applied, where the variance inequality was observed. Categorical variables were expressed as frequencies and percentages and compared using the Chi-square test or Fisher’s exact test, as appropriate. Effect sizes were calculated using Cohen’s d, with Hedges’ correction applied to adjust for small sample bias. Glass’s delta was reported where heterogeneity of variance was present. Ninety-five percent confidence intervals (95% CI) were reported where applicable. A p-value < 0.05 was considered statistically significant.
Patients in groups A and B had mean ages of 40.97 ± 9.10 and 45.83 ± 10.39 years, respectively. Group B’s mean BMI was 25.96 ± 3.43 kg/m2, while group A’s was 26.75 ± 4.73 kg/m2. The mean duration of surgery in group A was 64.57 ± 24.86 minutes, and in group B was 64.69 ± 24.06 minutes. Baseline characteristics were comparable between both groups for BMI, ASA score, and surgery duration [Table I]; the placebo group was slightly older (p = 0.041).
Baseline demographic and perioperative characteristics of study participants (Group A = Tapentadol, Group B= Placebo).
| Group A (n=35) | Group B (n=35) | p Value | |
|---|---|---|---|
| Age, years;mean(SD) | 40.97±9.10 | 45.83±10.93 | 0.041 |
| BMI, kg/m2;mean(SD) | 25.96±3.43 | 26.75±4.73 | 0.426 |
| ASA 2;n(%) | 34(97.1%) | 35(100%) | 0.314 |
| Duration of surgery, minutes;mean(SD) | 64.57±24.86 | 64.69±24.05 | 0.984 |
Continuous data expressed as mean±SD and categorical data expressed as frequency (percentage). P < 0.05 was considered significant. SD=Standard deviation, CI=Confidence Interval, BMI= Body Mass Index, ASA=American Society of Anesthesiologists Class.
The NRS was used in this study to record pain scores at 1, 2, 3, and 4 hours after surgery. Postoperative pain scores were lower in the tapentadol group at 1 hour (1.89 ± 0.83 vs 2.46 ± 1.15, p = 0.020) and 3 hours (1.06 ± 0.24 vs 1.23 ± 0.43, p = 0.042), with moderate effect sizes favoring tapentadol, as shown in Table II and Figure 2.
Postoperative pain scores measured by Numerical Rating Scale (NRS) at predefined time intervals following surgery (Group A = Tapentadol, Group B= Placebo).
| Time intervals (hours) | Pain score, Group A (n=35) Mean ± SD | Pain Score, Group B (n=35) Mean ± SD | Mean Difference in Pain scores. | 95%CI | p-value |
|---|---|---|---|---|---|
| 1 | 1.89 ± 0.83 | 2.46 ± 1.15 | −0.571 | −1.050 to −0.093 | 0.020 |
| 2 | 1.31 ± 0.63 | 1.66 ± 0.87 | −0.343 | −0.707 to 0.021 | 0.064 |
| 3 | 1.06 ± 0.24 | 1.23 ± 0.43 | −0.171 | −0.336 to −0.006 | 0.042 |
| 4 | 1.00 ± 0.00 | 1.03 ± 0.17 | −0.029 | −0.087 to 0.029 | 0.324 |
Data are presented as mean (SD). Mean difference calculated as Tapentadol group minus Placebo group. Negative values indicate lower pain scores in the tapentadol group. p<0.05 was considered significant. SD=Standard deviation, CI=Confidence Interval.
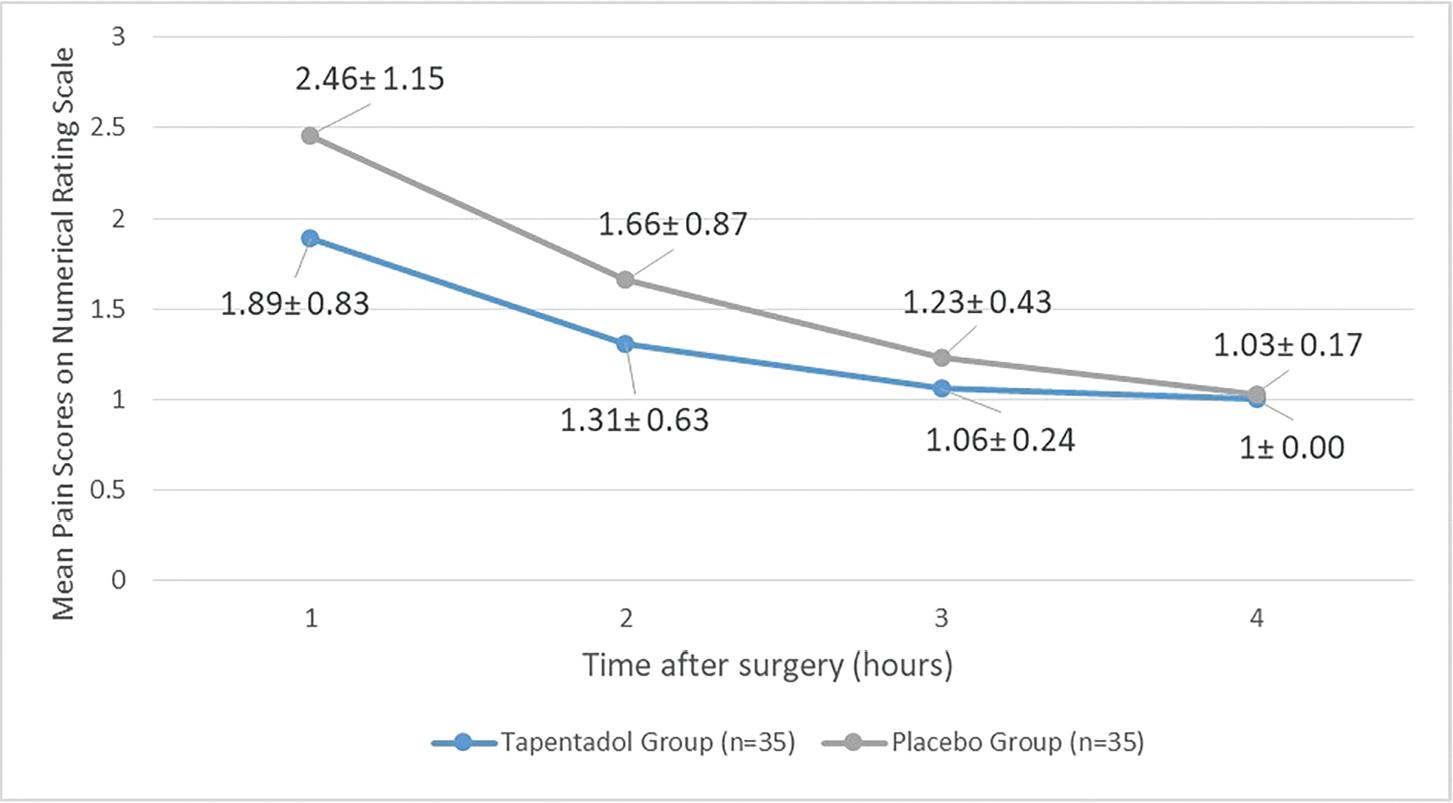
Mean postoperative pain scores measured using the Numerical Rating Scale (NRS: range 0–10) at 1, 2, 3, and 4 hours after surgery in patients receiving preoperative tapentadol (Group A) versus placebo (Group B). Data are presented as mean values and standard deviation (SD). Lower scores indicate less pain. Pain scores were significantly lower in the tapentadol group at 1 and 3 hours postoperatively (p < 0.05).
We found that the mean intraoperative morphine requirement was significantly lower in the tapentadol group (1.11 ± 1.53 mg) compared with the placebo group (3.36 ± 1.60 mg; p < 0.001) [Figure 3]. Time to first rescue analgesia was longer in Group A (58.0±21.7 min) than in Group B (43.5 ± 27.3 min), p = 0.290 (Table III). Only 13 (37.1%) patients in the tapentadol group required intraoperative morphine compared to 31 (88.6%) in the placebo group (p < 0.001). Rescue morphine use post op was lower in tapentadol group [5 (14.3%) vs.10 (28.6%), p = 0.145], as shown in Table IV.
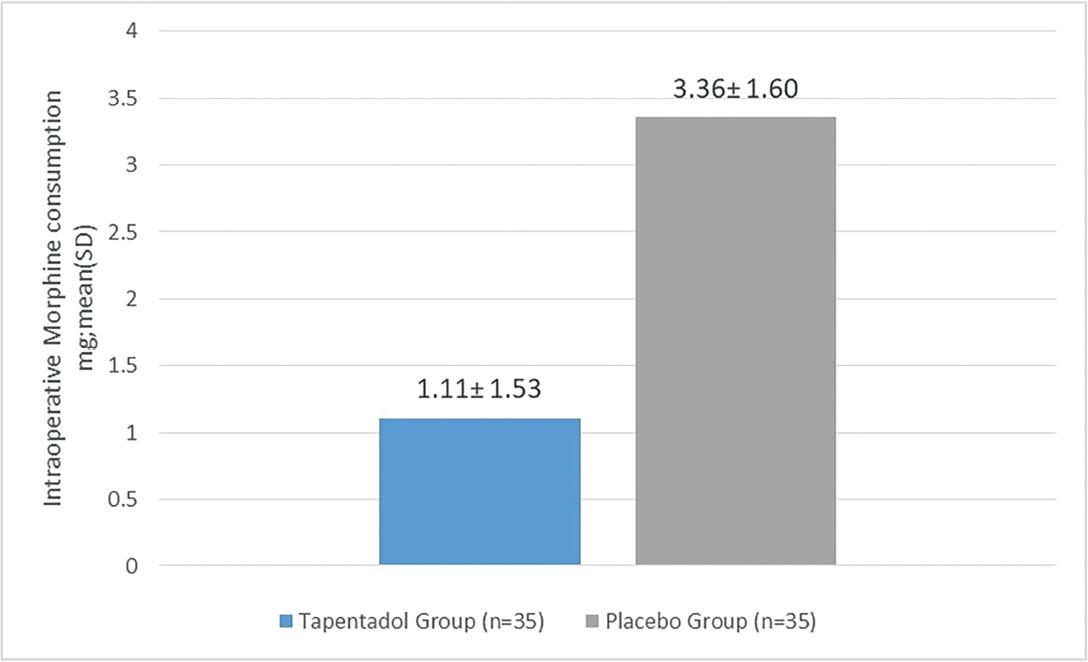
Mean intraoperative morphine consumption (mg) in patients receiving preoperative tapentadol (Group A) versus placebo (Group B) during breast conservative surgery. Data are presented as mean morphine dose in milligrams, with standard deviation (SD).
Comparison of intraoperative morphine consumption and time to first rescue analgesia between Group A: Tapentadol and Group B: Placebo.
| Group A (n=35) Mean ± SD | Group B (n=35) Mean ± SD | Mean Difference | 95%CI | p-value | |
|---|---|---|---|---|---|
| Intra-operative morphine consumption(mg) | 1.11 ± 1.53 | 3.36 ± 1.60 | −2.24 | −2.99 to −1.49 | <0.001 |
| Time to first rescue analgesia postoperatively(minutes) | 58.0 ± 21.7 | 43.5 ± 27.3 | 14.5 | −14.4 to 43.4 | 0.290 |
Data are presented as mean (SD). Mean difference calculated as Tapentadol group minus Placebo group. p < 0.05 was considered significant. SD=Standard deviation, CI=Confidence Interval.
Comparison between number of patients requiring rescue analgesia in each group. Group A: Tapentadol and Group B: Placebo.
| Group A (n=35) Frequency (%) | Group B (n=35) Frequency (%) | p-value | |
|---|---|---|---|
| Intra-operative | 13 (37.1) | 31 (88.6) | <0.001 |
| Post-operative | 5 (14.3) | 10 (28.6) | 0.145 |
Data expressed as frequency (percentage). P<0.05 was considered significant.
Altogether, this highlights that the greatest analgesic benefit occurred during the early post-operative phase, diminishing by the fourth hour after surgery.
Adverse effects were minimal and comparable; one case of vomiting (2.9%) occurred in each group.
The present study assessed the preemptive analgesic efficacy of tapentadol in reducing perioperative analgesic requirements among patients undergoing breast cancer surgery. Pain intensity was measured using the Numerical Rating Scale at 1, 2, 3, and 4 hours after surgery. A statistically significant difference in postoperative pain scores was observed between the groups at 1 and 3 hours, with Group A (tapentadol) consistently demonstrating lower mean scores. Although statistically significant differences in pain scores were observed at certain time points, the absolute differences were small and likely below the minimal clinically important difference for acute postoperative pain. Therefore, the clinical significance of these findings may be limited.
Mean intraoperative morphine consumption was lower in Group A (Tapentadol) as compared to Group B (placebo). The proportion of patients requiring rescue analgesia was also lower in the tapentadol group. These findings support the hypothesis that preemptive administration of tapentadol effectively reduces perioperative opioid consumption and improves early postoperative pain control.
The results are consistent with those reported by Yadav et al. (2016), who demonstrated that 75 mg of oral tapentadol given preoperatively significantly reduced perioperative pain and postoperative analgesic requirements in patients undergoing laparoscopic cholecystectomy (11) Similar conclusions were drawn by Kulkarni et al., who observed superior postoperative analgesia with tapentadol, both in quality and duration, in adult patients undergoing abdominal surgery, confirming the drug’s broad efficacy across different surgical contexts (12). Studies evaluating tapentadol extended-release formulations have also reported significant reductions in average pain intensity compared with placebo (13).
In another randomized controlled trial including 120 ASA I–II patients undergoing laparoscopic cholecystectomy, preemptive administration of 75 mg tapentadol resulted in longer rescue analgesia intervals and lower postoperative pain scores compared with both 50 mg tapentadol and placebo. 14 Comparable outcomes were also observed in a double-blind study in which tapentadol nasal spray, administered 30 minutes before induction of anesthesia, significantly reduced postoperative pain and the need for additional analgesics in breast surgery patients (15). These studies reinforce the analgesic potential of tapentadol across different routes of administration.
Several researchers have evaluated tapentadol’s efficacy using different doses ranging from 50 to 200 mg. (16,17). Kleinert et al. demonstrated that a single 75 mg oral dose of tapentadol effectively reduced moderate-to-severe dental pain and was better tolerated than morphine (18). Similarly, Hartrick et al. found that tapentadol immediate-release 50 mg and 75 mg, as well as oxycodone hydrochloride 10 mg, significantly reduced postoperative pain intensity after joint replacement surgery when compared with placebo (19) A Cochrane review further supported these findings (20), noting that tapentadol offers superior tolerability and a lower incidence of opioid-related side effects such as nausea, vomiting, and constipation. The improved safety profile of tapentadol is attributed to its dual mechanism of action, combining μ-opioid receptor agonism with inhibition of noradrenaline reuptake, which together produce effective analgesia with fewer adverse effects (21,22).
The current study’s findings align with this body of evidence and extend it to a local Pakistani population, where data on tapentadol use have been scarce. Despite encouraging results, several limitations should be acknowledged. The sample size was modest and limited to a single tertiary cancer center, potentially limiting generalizability. Variability in pharmacokinetics and individual pain thresholds may have influenced analgesic requirements. Standardized multimodal analgesia was used in all patients for ethical and clinical reasons, which may have attenuated between-group differences but enhanced real-world applicability. The presence of a statistically significant age imbalance between groups highlights a limitation of the study, as age may influence pain threshold. Although this likely reflects chance variation inherent to randomization and the difference was not clinically substantial, residual confounding cannot be excluded. Intraoperative opioid administration was guided by hemodynamic changes, which, although commonly used to guide intraoperative opioid administration, are non-specific indicators of nociception and may be influenced by multiple confounders. Objective nociception monitoring could allow for more precise analgesic titration in future studies. This study was designed to evaluate early postoperative analgesia within the initial 4 hours, based on the expected duration of action of tapentadol. As such, longer-term outcomes, including cumulative opioid consumption, functional recovery, and persistent postoperative pain, were not assessed. These endpoints remain important and should be explored in future large-scale, multicenter, dose–response studies with longer observation periods, which are warranted to establish optimal dosing strategies and validate these findings across diverse populations.
Nevertheless, the study has notable strengths. It was a randomized, double-blinded, controlled trial with standardized anesthetic and analgesic protocols, a clearly defined objective, and an adequately powered sample size. The use of objective pain measurements and rigorous statistical analysis in SPSS enhanced the reliability of the results. Overall, this study adds to the growing evidence supporting tapentadol as a safe and effective preemptive analgesic that can reduce perioperative opioid consumption and improve postoperative comfort without increasing adverse effects.
In conclusion, tapentadol was associated with lower postoperative pain scores at select time points and significantly reduced intraoperative morphine consumption, supporting its role in preemptive analgesia. However, reductions in postoperative opioid use and prolongation of time to rescue analgesia did not reach statistical significance and should be interpreted with caution. Within the limitations of the present study, tapentadol appears to be a viable option for preemptive analgesia with a favorable safety profile. Nevertheless, the pursuit of an optimal multimodal perioperative analgesic regimen that maximizes efficacy while minimizing adverse effects remains an area of ongoing investigation.