Among infants, there is approximately 5.4 million under-5 mortality in the world, of which 2.5 million die during the neonatal period, and approximately two-third of neonates are born prematurely.1,2 Approximately 1 million deaths per year are caused by infection occurring in the neonatal period (0–28 days), accounting for over 25% of global neonatal deaths, and 99% of these deaths occur in the developing countries.2
Neonatal sepsis is a systemic infection that occurs in infants during the first 4 weeks of life and is a major cause of mortality and morbidity in preterm newborns.3 Neonatal sepsis is a severe problem affecting the neonates, especially if they are preterm and of low birth weight, with an incidence varying between 1% and 40%.4
Neonatal sepsis can be classified into 2 types based on the time of onset after delivery: Early onset sepsis (EOS) (infection occurring during the first 3 days of life) and late-onset sepsis (LOS), which manifests after 3 days and is mainly due to acquiring the pathogen from prolonged hospitalization, especially in preterm newborns.4,5 Early-onset neonatal sepsis (EONS) is often fatal and remains severe among preterm infants, especially newborn preterm infants, often for prolonged periods.6
Most early onset neonatal sepsis is associated with maternal and neonatal characteristics, with preterm being the cause of neonatal intensive care unit (NICU) admissions.7 Current evidence has revealed that healthcare systems are burdened due to prolonged hospital stays by neonates.8,9
The chance of survival for preterm babies in the low resource settings is very low,3 and sepsis accounts for 25% of all neonatal deaths in sub-Saharan Africa (SSA) and southern Asia.10 In this study area, most of the neonates died due to prematurity (31%) and neonatal sepsis (29.7%).11
Despite advances in healthcare to improve neonatal survival rates and reduce complications in preterm infants, preterm neonatal mortality due to sepsis remains high. According to a systematic review and meta-analysis report, the prevalence of neonatal sepsis was approximately 45% in Ethiopia,12 and based on the 2019 Ethiopian mini demographic health survey report, the neonatal mortality rate was 30 deaths per 1000 live births;13 prematurity accounts for 11% of under-5 mortality.14
Therefore, the third sustainable development goal for child health aims to end and reduce newborns and under-5 mortalities to as low as 12/1000 and 25/1000 by 2030: through better prevention and management of preterm births and severe infections.15 Although neonatal sepsis and preterm birth are the leading causes of mortality, the studies previously done were focused on either the prevalence or mortality rate of preterm neonates. To the best of our knowledge, limited studies have been conducted on the time-to-death of preterm neonates diagnosed with neonatal sepsis and predictors of mortality in Ethiopia. This study was conducted to fill the evidence gap and to enhance the utility of the evidence on time-to-death and predictors of mortality among preterm neonates with neonatal sepsis. Therefore, this study aimed to determine the time-to-death and predictors of mortality among preterm neonates diagnosed with neonatal sepsis and admitted to governmental hospitals, Southwest Ethiopia.
The study was conducted in government hospitals at the Southwest Region; officially the South West Ethiopia Peoples’ Region is a regional state in southwestern Ethiopia. It was split off from the Southern Nations, Nationalities, and Peoples’ Region (SNNPR) on November 23, 2021 after a successful referendum. It consists of Keffa, Sheka, Bench Sheko, Dawro, West Omo Zones, and Konta special woreda. The 3 hospitals are Mizan-Tepi University teaching hospital (MTUTH), Tepi general hospital, and G/tsaddik shewa general hospital. MTUTH is located 584 km far from Addis Ababa. The Tepi general hospital is in the Sheka administrative Zone, 622 km away from Addis Ababa. The G/tsaddik Shewa general hospital is in Keffa zone, 464 km away from Addis Ababa. Hospitals provide delivery and other maternal and newborn care including NICU services. The study was conducted between March 2021 and January 30, 2022 at the government hospitals.
A prospective cohort study was conducted among preterm neonates with neonatal sepsis admitted to the NICU wards of hospitals between March 2021 and January 30, 2022.
All preterm neonates diagnosed with neonatal sepsis and admitted in the NICU ward to government hospitals during the study period.
All selected neonates diagnosed with neonatal sepsis and admitted in the NICU ward to government hospitals during the study period.
Live preterm neonates diagnosed with neonatal sepsis and admitted in the NICU were eligible for the study.
Preterm neonates diagnosed with neonatal sepsis that had an incomplete observation during follow-up, and unknown date of admission and date of death were excluded.
Power log rank estimated sample sizes for 2-sample comparison of survivor functions—Log-rank test; Freedman method was used to obtain representative samples of preterm neonates admitted to the NICU with diagnosed neonatal sepsis as follows:
Where:
z@1/2: z value at 95% confidence interval (CI) = 1.96;
ZB: the power of the study = 80%;
P = 50% cumulative mortality rate;
p = mortality rate;hazard ratio (HR) = 0.5;
Ɵ = ln (HR), i.e., HR = exp. (Ɵ) and then Ɵ = ln (HR).
The total sample size was calculated as
Adding a 10%, for incomplete data/missing data the final minimum sample size required was 363.
From 7 government hospitals in the southwest region, MTUTH, Tepi general hospital, and G/tsaddik Shewa general hospital were selected using the lottery method.
Proportional allocation was performed for each hospital based on the previous number of preterm neonates diagnosed with neonatal sepsis and admitted to the NICU. Thereafter, we included all preterm neonates diagnosed with neonatal sepsis who were admitted to the NICU. The study participants were selected from each hospital using a consecutive sampling technique. All recruited study participants were followed until the outcome of interest (i.e., either death or censure) appeared.
Dependent variable: Time-to-death and dichotomized into death or censored.
Independent variables: Include maternal and neonatal socio-demographic variables, medical, obstetric, surgical, and neonatal characteristic variables.
Median survival time: The median survival of time of 50% of neonates.
Survival status: The outcome of premature neonates diagnosed with sepsis, either death or censored.
Death/Event: Refers to the neonates that have died while in the therapeutic units and declared as dead in the treatment logbook by the physician.
Censored: Preterm neonates diagnosed with neonatal sepsis and admitted in the NICU. Those alive beyond 28 days of neonatal age, those left against medical advice, or discharged with improvement and referred.
Time origin: Specific time of admission of preterm neonates at NICU with diagnosis of neonatal sepsis.
Time of exit: Specific time of observation outcome (death or censored).
After reviewing the literature, the tool was adapted and prepared in English and translated into the local language, Amharic, and re-translated back into English (Supplementary File 1). Data were collected through face-to-face interviews with the mothers and neonatal chart reviews (primary and secondary). Secondary data were used to obtain baseline information that the mothers could not address. After excluding all baseline data on different related factors, data on factors that can occur starting from the first day of follow-up were collected during follow-up (i.e., from the time of admission to 28 days of neonatal age) or at the occurrence of an event of interest (i.e., death or censored). Only the first episode was included if the patients were admitted with >1 episode of neonatal sepsis over 28 days.
After coding, editing, and cleaning data were entered into Epi-data manager version 4.4.2.1 (The EpiData Association, Odense, Denmark) and exported to Stata version 14 (StataCorp LLC, Texas, USA) for analysis. The median survival time was estimated using Kaplan-Meier survival estimates. Predictors of mortality were identified using the Cox proportional hazards (CPH) model. The assumptions of the CPH model were assessed using the Schoenfeld residual/global test (0.2194). Multi-collinearity was assessed using the variance inflation factor (VIF) (1.21). Based on bivariate analysis, variables with P-value <0.25 were transferred to the multivariable analysis. Variables with P-value <0.05 at 95% confidence level in multivariable analysis were considered as independent predictors for mortality.
Pretest was conducted on 5% of sample size at Chena General Hospital, before actual data collection period and then editions and wording were made. Training was provided to the data collectors and supervisors on data collection techniques and ethical issues. Supervisors regularly checked the completed questionnaires.
In this study, the total sample of 363 preterm neonates with diagnosis of sepsis were reviewed. Of these, 9 (2.5%) were excluded since they had incomplete medical charts. The remaining 354 (97.5%) preterm neonates were included in the analysis making response rate of 97.5%. Each preterm neonate diagnosed with neonatal sepsis had a different length of hospital stay: a minimum of 1 day and a maximum of 28 days.
In this study, 178 neonates (50.28%) were male and 176 (49.72%) were female. A majority (97.46%) of the preterm neonates were in the age category of ≤7 days during admission. About 306 (86.44%) of women were found in the age range of 20–35 years with a median age of 25 years (interquartile range of 22–30) (Table 1).
Sociodemographic characteristics of preterm neonates diagnosed with neonatal sepsis admitted in NICU ward of Government Hospitals in Southwest Ethiopia, from March 2021 to January 30, 2022 (N = 354), N (%).
| Variables and category | Total | Outcome status | |
|---|---|---|---|
| Censored | Death | ||
| Age (days) | |||
| ≤7 | 345 (97.46) | 224 (64.93) | 121 (35.07) |
| 8–28 | 9 (2.54) | 9 (100.0) | - |
| Gender | |||
| Female | 176 (49.72) | 122 (69.32) | 54 (30.68) |
| Male | 178 (50.28) | 111 (62.36) | 67 (37.64) |
| Maternal age (years) | |||
| <20 | 22 (6.21) | 12 (54.55) | 10 (45.45) |
| 20–35 | 306 (86.44) | 204 (66.67) | 102 (33.33) |
| ≥35 | 26 (7.34) | 17 (65.38) | 9 (34.62) |
| Residency of mothers | |||
| Urban | 109 (30.79) | 81 (74.31) | 28 (25.69) |
| Rural | 245 (69.21) | 152 (62.04) | 93 (37.96) |
Note: NICU, neonatal intensive care unit.
A total of 116 (32.77%), 92 (25.99%), 164 (46.33%), and 42 (11.86%) preterm neonates with neonatal sepsis also had comorbidity of respiratory distress syndrome (RDS), hypoglycemia, hypothermia, and prenatal asphyxia, respectively (Table 2).
Medical/surgical comorbidity characteristics of preterm neonates diagnosed with neonatal sepsis admitted in the NICU ward of Government Hospitals in Southwest Ethiopia from March 2021 to January 30, 2022 (N = 354), N (%).
| Variables and category | Total | Outcome status | |
|---|---|---|---|
| Alive | Death | ||
| RDS | |||
| No | 238 (67.23) | 170 (71.43) | 68 (28.57) |
| Yes | 116 (32.77) | 63 (54.31) | 53 (45.69) |
| Jaundice | |||
| No | 313 (88.42) | 202 (64.54) | 111 (35.46) |
| Yes | 41 (11.58) | 31 (75.61) | 10 (24.39) |
| Anomaly | |||
| No | 342 (96.61) | 224 (65.50) | 118 (34.50) |
| Yes | 12 (3.39) | 9 (75.00) | 3 (25.00) |
| Hypoglycemia | |||
| No | 262 (74.01) | 187 (71.37) | 75 (28.63) |
| Yes | 92 (25.99) | 46 (50) | 46 (50) |
| Hypothermia | |||
| No | 190 (53.67) | 143 (75.26) | 47 (24.74) |
| Yes | 164 (46.33) | 90 (54.88) | 74 (45.12) |
| Asphyxia | |||
| No | 312 (88.14) | 208 (66.67) | 104 (33.33) |
| Yes | 42 (11.86) | 25 (59.52) | 17 (40.48) |
Note: NICU, neonatal intensive care unit; RDS, respiratory distress.
A total of 340 (96.05%) of the preterm neonates diagnosed with neonatal sepsis were born at health institutions. Most (85.59%) of the preterm neonates were born with low birth weight (<2500 g) with a median weight of 1950.00 g. A total of 303 (85.59%) preterm neonates were born with gestational age (GA) of 32–36 weeks with median GA of 34 weeks and interquartile range of 32–36 weeks; 238 (67.23%) preterm neonates had 1st-minute Apgar score range <7; 232 (65.54%) preterm neonates also had 5th-minute activity, pulse, grimace, appearance, and respiration (APGAR) of 37 and only 200 (56.50%) preterm neonates received kangaroo mother care (KMC) at the time of hospitalization in the NICU (Table 3).
Neonatal-related characteristics of preterm neonates diagnosed with neonatal sepsis admitted in the NICU of Government Hospitals in Southwest Ethiopia from March 2021 to January 30, 2022 (N = 354), N (%).
| Characteristics and category | Total | Outcome status | |
|---|---|---|---|
| Censored | Death | ||
| Where delivery was conducted | |||
| Health institution | 340 (96.05) | 225 (66.18) | 115 (33.82) |
| Home | 14 (3.95) | 8 (57.14) | 6 (42.86) |
| Neonatal Wight (g) | |||
| <2500 | 303 (85.59) | 189 (62.38) | 114 (37.62) |
| ≥2500 | 51 (14.41) | 44 (86.27) | 7 (13.73) |
| GA (weeks) | |||
| 28–31 | 51 (14.41) | 24 (47.06) | 27 (52.94) |
| 32–36 | 303 (85.59) | 209 (68.98) | 94 (31.02) |
| First minute APGAR score | |||
| <7 | 238 (67.23) | 142 (59.66) | 96 (40.34) |
| ≥7 | 116 (32.77) | 91 (78.45) | 25 (21.55) |
| 5th minute APGAR | |||
| <7 | 122 (34.46) | 53 (43.44) | 69 (56.56) |
| ≥7 | 232 (65.54) | 180 (77.5) | 62 (22.41) |
| Application of KMC | |||
| Yes | 154 (72.73) | 112 (72.73) | 42 (27.27) |
| No | 200 (56.50) | 121 (60.50) | 79 (39.50) |
| Weight for GA | |||
| LGA | 17 (4.8) | 13 (76.47) | 4 (23.53) |
| AGA | 271 (76.55) | 193 (71.22) | 78 (28.78) |
| SGA | 66 (18.64) | 27 (40.91) | 39 (59.09) |
| Breathing status at birth | |||
| Didn’t cry | 113 (31.92) | 36 (31.86) | 77 (68.14) |
| Cry | 241 (68.08) | 197 (81.74) | 44 (18.26) |
Note: AGA, appropriate for gestational age; APGAR, activity, pulse, grimace, appearance and respiration; GA, gestational age; KMC, kangaroo mother care; LGA, large for gestational age; NICU, neonatal intensive care unit; RDS, respiratory distress syndrome; SGA, small for gestational age.
A total of 330 women (93.5%) had a history of at least one antenatal care (ANC) follow-up during their current pregnancy. Only 42 (11.86%) women had a history of obstetric complications such as placental abruption, placenta previa, and pregnancy induced in current pregnancy. The majority (75.99%) were single tone type of pregnancy. Most preterm neonates were born from a multi-para mother, which was around 53.11% (Table 4).
Maternal medical and obstetrics-related characteristics of preterm neonates diagnosed with neonatal sepsis admitted in the NICU of Government Hospitals, in Southwest Ethiopia from March 2021 to January 30, 2022 (N = 354), N (%).
| Characteristics and category | Total | Outcome status | |
|---|---|---|---|
| Censored N (%) | Death N (%) | ||
| Chronic medical disease | |||
| No | 339 (95.76) | 218 (67.26) | 111 (32.74) |
| Yes | 15 (4.24) | 5 (33.33) | 10 (66.67) |
| Antenatal care | |||
| No | 23 (6.5) | 11 (47.83) | 12 (52.17) |
| Yes | 331 (93.5) | 222 (67.07) | 109 (32.93) |
| Obstetric complications | |||
| No | 312 (88.14) | 199 (63.78) | 113 (36.22) |
| Yes | 42 (11.86) | 34 (80.95) | 8 (19.05) |
| Mode of delivery | |||
| C/S | 73 (20.62) | 57 (78.08) | 16 (21.92) |
| Vaginal | 281 (79.38) | 176 (62.63) | 105 (37.37) |
| Pregnancy type | |||
| Single | 269 (75.99) | 188 (69.8) | 81 (30.11) |
| Multiple | 85 (24.01) | 45 (52.94) | 40 (47.06) |
| Febrile illness of the mother | |||
| No | 335 (94.63) | 221 (65.97) | 114 (34.03) |
| Yes | 19 (5.37) | 12 (63.16) | 7 (36.84) |
| Presentation | |||
| Cephalic | 440 (96.05) | 224 (65.88) | 116 (34.12) |
| Non-cephalic | 14 (3.95) | 9 (64.29) | 5 (35.71) |
| Parity | |||
| Para I | 166 (46.89) | 113 (68.07) | 53 (31.93) |
| Multi-para | 188 (53.11) | 120 (63.83) | 68 (36.17) |
Note: NICU, neonatal intensive care unit.
From 354 neonates, 121 (34.18%) (95% CI: 29.40–39.30) have died during the follow-up period and the remaining 233 (65.82%) were censored (Figure 1).
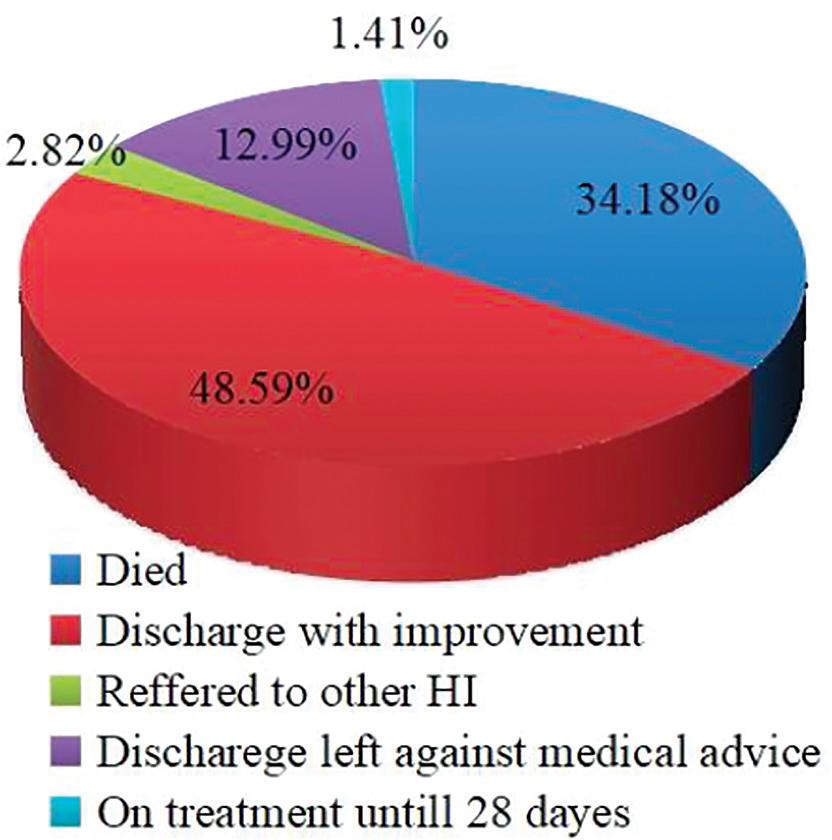
Treatment outcome among preterm neonates diagnosed with neonatal sepsis admitted in the NICU of Government Hospitals in Southwest Ethiopia from March 2021 to January 30, 2022 (N = 354).
Note: NICU, neonatal intensive care unit.
Overall median survival time of preterm neonates with sepsis was 15 days (95% CI: 10–28). The 50% cumulative survival functions of preterm neonates with neonatal sepsis died at a median of 15 days’ duration (Figure 2).
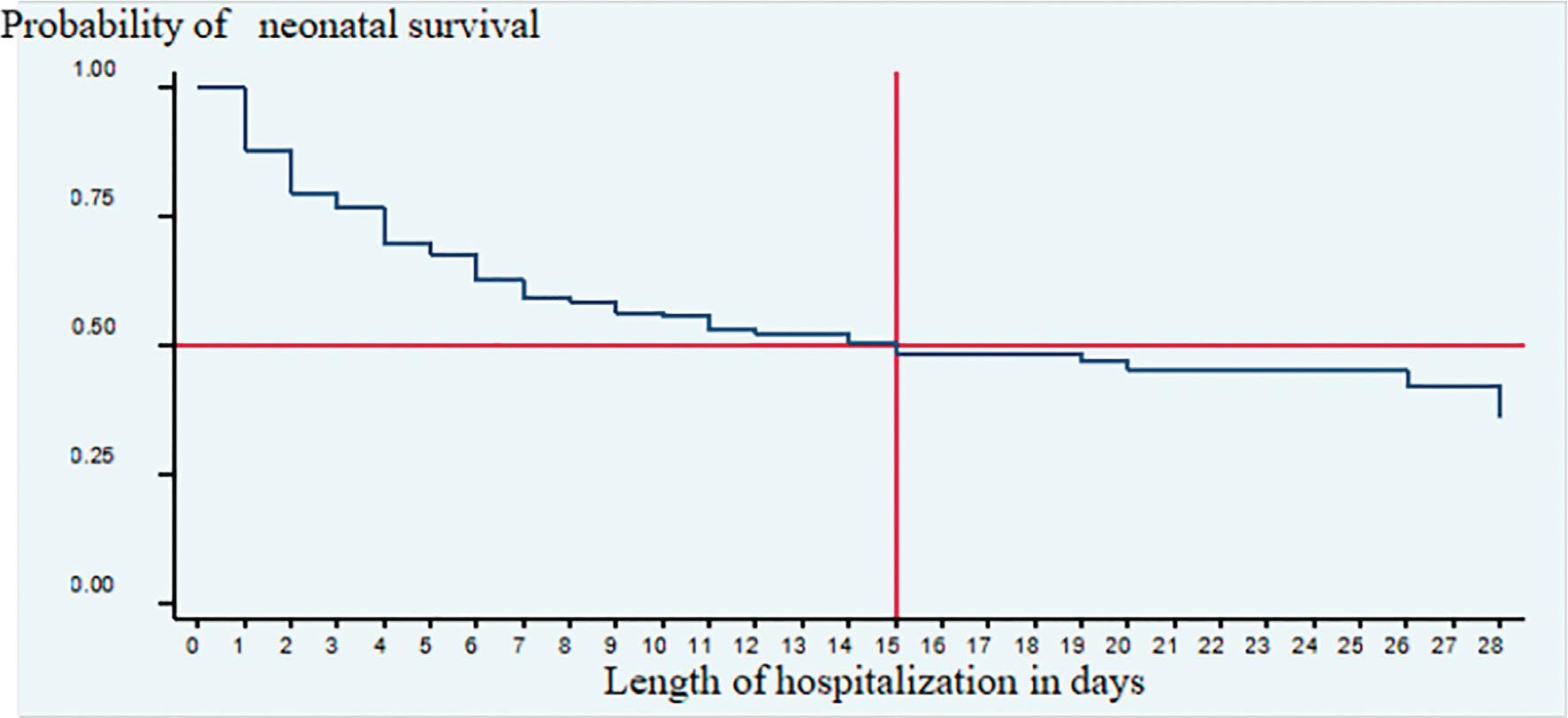
Kaplan–Meier survival estimate graph overall median survival time among preterm neonates diagnosed with sepsis admitted to Government Hospitals in Ethiopia, 2022 (N = 354).
The fitness of the final model was checked graphically using the Cox Snell residual, showing that the hazard function follows the 45° line closely confirming that the final model is a good fit (Figure 3).
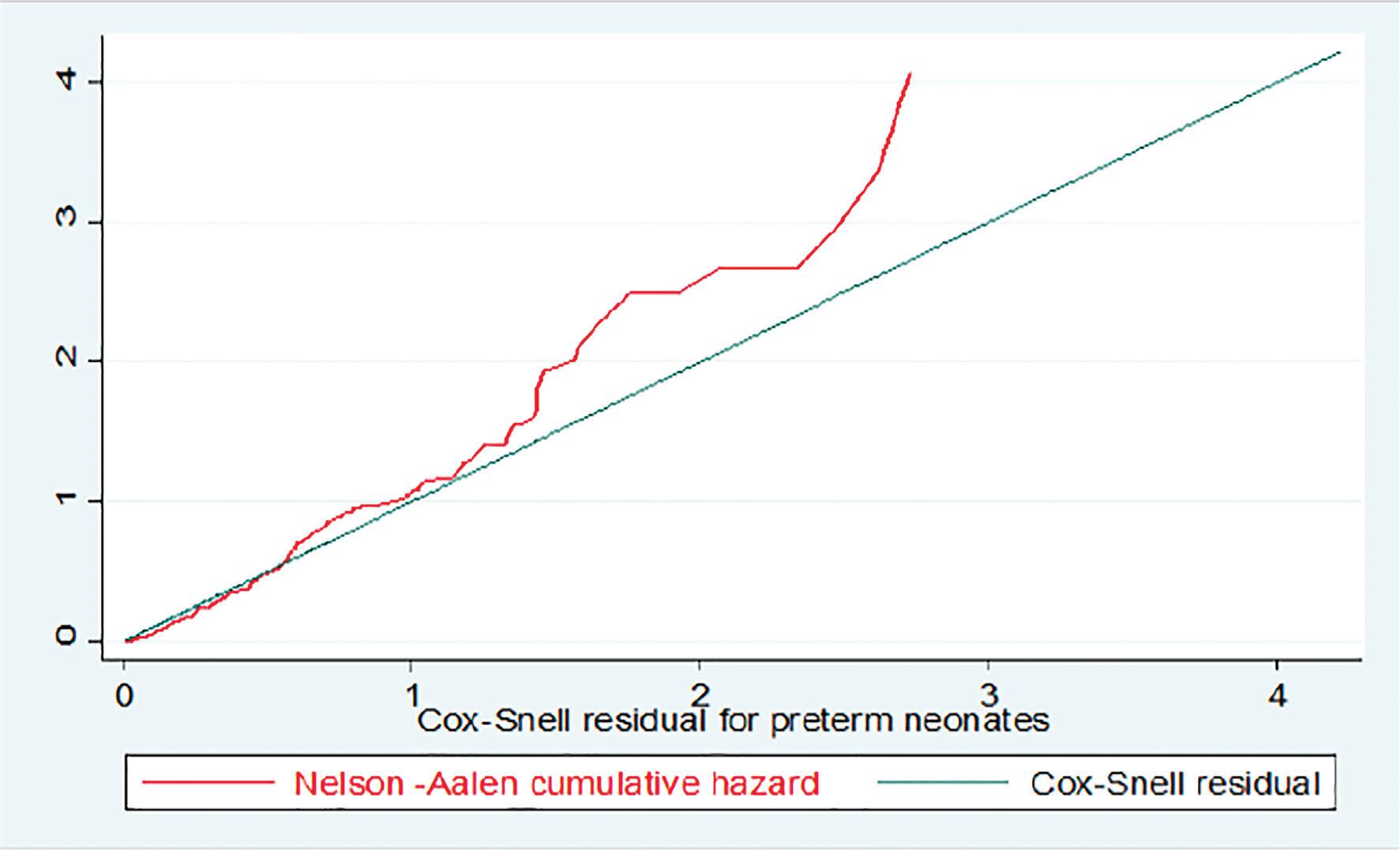
Cox-Snell residual, Nelson-Aalen cumulative hazard graph among preterm neonates diagnosed with sepsis and admitted to Government Hospitals in Southwest Ethiopia, 2022 (N = 354).
Bivariate analysis revealed the sex of the neonates, maternal residence, antenatal care status, pregnancy-related complications, RDS, jaundice, KMC, mode of delivery, breathing status, maternal parity, birth weight, hypoglycemia, hypothermia, GA, weight for gestational age (WFGA), type of pregnancy, APGAR 1st minute <7, and APGAR 5th minute <7 were significant at P-value <0.25, and were eligible for multivariate analysis. Significant variables in bivariate analysis were included in the multivariate analysis. Multivariate analysis covariates such as antenatal care status, RDS, jaundice, and APGAR score at 5 min were significant at P-value <0.05 and independent predictors of neonatal mortality.
Preterm neonates with neonatal sepsis who were born from mothers who did not attend at least one ANC had 2.5 times higher hazard of mortality than neonates born from mothers attending at least one ANC during the current pregnancy (adjusted hazard ratio [AHR] 2.5 [95% CI: 1.3–4.84]). Preterm neonates diagnosed with both neonatal sepsis and RDS had 1.5 times higher hazard of mortality than preterm neonates without RDS (AHR 1.50 [95% CI: 1.13–2.31]). Preterm neonates diagnosed with both neonatal sepsis and jaundice had 1.89 times higher hazard of mortality than preterm neonates without jaundice (AHR 1.89 [95% CI: 1.26–2.84]). In addition, preterm neonates diagnosed with neonatal sepsis who had 5 min APGAR scores <7 after birth had a 1.5 times higher hazard of mortality from neonatal sepsis than preterm neonates who had >7 APGAR scores after birth (AHR 1.5 [95% CI: 1.29–3.46]) (Table 5).
Bivariate and multivariate result of preterm neonates diagnosed with neonatal sepsis, admitted in the NICU of Governmental Hospitals, in Southwest Ethiopia from March 2021 to January 30, 2022 (N = 354).
| Variables and category | Outcome status | CHR (95% Cl) | AHR (95%CI) | P-value | |
|---|---|---|---|---|---|
| Alive | Death | ||||
| Gender | |||||
| Female | 122 | 54 | 1 | 1 | |
| Male | 111 | 57 | 1.38 (0.96–1.93) | 1.38 (0.94–2.02) | 0.098 |
| Residency | |||||
| Urban | 81 | 28 | 1 | 1 | |
| Rural | 152 | 93 | 1.48 (0.99–2.22) | 1.44 (0.89–2.33) | 0.132 |
| Antenatal care | |||||
| Yes | 222 | 109 | 1 | 1 | |
| No | 11 | 12 | 2.06 (1.13–3.80) | 2.5 (1.3–4.84) | 0.005* |
| Pregnancy complication | |||||
| No | 199 | 113 | 1 | 1 | |
| Yes | 34 | 8 | 2.43 (1.27–4.65) | 0.55 (0.22–1.39) | 0.209 |
| Respiratory distress | |||||
| No | 170 | 68 | 1 | 1 | |
| Yes | 63 | 53 | 1.57 (1.06–2.23) | 1.50 (1.13–2.31) | 0.045* |
| Jaundice | |||||
| No | 202 | 111 | 1 | 1 | |
| Yes | 31 | 10 | 3.08 (2.18–4.38) | 1.89 (1.26–2.84) | 0.002* |
| Application of KMC | |||||
| Yes | 112 | 42 | 1 | 1 | |
| No | 121 | 79 | 1.66 (1.15–2.40) | 0.97 (0.64–1.47) | 0.891 |
| Mode of delivery | |||||
| C/S | 57 | 16 | 1 | 1 | |
| Vaginal | 176 | 105 | 0.54 (0.32–0.92) | 0.56 (0.32–0.99) | 0.075 |
| Breathing status | |||||
| Cried | 197 | 44 | 1 | 1 | |
| Didn’t cry | 36 | 77 | 4.12 (2.88–5.90) | 2.9 (1.88–4.51) | 0.09 |
| Parity | |||||
| Para I | 113 | 53 | 1 | 1 | |
| Multi-para | 120 | 68 | 1.40 (0.98–2.02) | 1.75 (1.19–2.58) | 0.075 |
| Weight (g) | |||||
| ≥2500 | 189 | 114 | 1 | 1 | |
| <2500 | 44 | 7 | 2.76 (1.29–5.94) | 1.93 (0.83–4.47) | 0.125 |
| Hypoglycemia | |||||
| No | 187 | 75 | 1 | 1 | |
| Yes | 46 | 46 | 1.78 (1.24–2.55) | 1.54 (0.97–2.45) | 0.064 |
| Hypothermia | |||||
| No | 143 | 47 | 1 | 1 | |
| Yes | 90 | 74 | 1.89 (1.32–2.67) | 1.35 (0.86–2.12) | 0.194 |
| GA (weeks) | |||||
| >32 | 24 | 27 | 1 | 1 | |
| <32 | 209 | 94 | 0.60 (0.40–0.91) | 0.84 (0.52–1.37) | 0.494 |
| WFGA | |||||
| AGA | 193 | 78 | 1 | 1 | |
| LGA | 13 | 4 | 0.92 (0.34–2.51) | 0.94 (0.32–2.79) | 0.916 |
| SGA | 27 | 39 | 2.03 (1.3–2.96) | 1.24 (0.81–1.94) | 0.338 |
| Pregnancy types | |||||
| Single tone | 188 | 81 | 1 | 1 | |
| Multiple | 45 | 40 | 1.37 (0.94–1.99) | 1.08 (0.71–1.65) | 0.721 |
| APGAR 1st min. | |||||
| <7 | 142 | 96 | 0.56 (0.36–0.85) | 0.69 (0.39–1.24) | 0.216 |
| ≥7 | 91 | 25 | 1 | 1 | |
| APGAR 5th min | |||||
| <7 | 53 | 69 | 2.7 (1.91–3.93) | 2.11 (1.29–3.46) | 0.015* |
| ≥7 | 180 | 52 | 1 | 1 | |
Note: NB: significant at P-value < 0.05 in multi-variable analysis; 1, considered as reference category.
AGA, appropriate for gestational age; AHR, adjusted hazard ratio; APGAR, activity, pulse, grimace, appearance and respiration; CHR, crude hazard ratio; CI, confidence interval; GA, gestational age; KMC, kangaroo mother care; LGA, large for gestational age; NICU, neonatal intensive care unit; RDS, respiratory distress syndromerespirator syndrome; SGA, small for gestational age; WFGA, weight for gestational age.
In this study, the overall mortality rate of preterm neonates with neonatal sepsis was 121 (34.18%) 95% CI: 29.40–39.30). This study was in line with a study conducted at Jimma University Specialized Hospital,16 where the mortality rate was 34.9%. This similarity may be due to the similarity in sociodemographic status. On the other hand, this study was higher than the studies conducted in Iran,17 Pakistan,18 and the University of Gondar Comprehensive Specialized Hospital,19 where the overall proportion of deaths was 9.1%, 14%, and 28.8%, respectively. A possible explanation may that be in our study the participants were preterm neonates with a confirmed diagnosis of neonatal sepsis that would lead to higher mortality, whereas other studies were conducted on preterm neonates admitted to NICU. Another possible reason may be the differences in neonatal service provision.
The median survival time of neonates was 15 days (95% CI: 10–28) across the NICU during the hospitalization period. This result was lower than that reported in Ethiopia at the University of Gondar Hospital,20 in which the overall median survival time was 28 days. A possible reason for this marked difference may be the difference in inclusion criteria of the study subjects and differences in neonatal care provision. In this study, all the subjects were cases of neonatal sepsis, whereas in the study conducted at the University of Gondar Hospital, the study participants were all preterm neonates with/without neonatal sepsis that may have contributed to the longer median survival time.
Preterm neonates who were born to mothers who did not have ANC follow-up and who had neonatal sepsis had 2.5 times higher hazard of death than preterm neonates who were born to mothers who had ANC follow-up (AHR: 2.5 [95% CI: 1.3–4.8]). This study was supported by a study conducted in Ethiopia at the University of Gondar Hospital.20 A possible reason might be that lack of ANC visits may result in inadequate monitoring of pregnancy-related infections and may lead to neonatal complication during and after delivery, which may be associated with increased risk of neonatal death.
In this study, neonates diagnosed with both sepsis and RDS had 1.5 times hazard of mortality as compared with preterm neonates who had been diagnosed with only neonatal sepsis (AHR 1.50 [95% CI: 1.13–2.31]). This finding was supported by the studies conducted in Nigeria,21 and Tikur Anbessa Specialized Hospital, Ethiopia.22 The possible reason might be the fact that preterm neonates develop RDS, a prematurity-related surfactant deficiency mostly involving risk of lung collapse, which leads to difficulty of breathing and unable to survive, finally ending up with death. Many studies have confirmed an inverse relationship between RDS and GA.23
In this study, preterm neonates diagnosed with both neonatal sepsis and jaundice had 1.89 times higher hazards of mortality than preterm neonates without jaundice (AHR 1.89 [95% CI: 1.26–2.84]). A possible reason could be that increased risk of jaundice induced neurological injury in preterm neonates, leading to death. In addition, in this study, preterm neonates diagnosed with neonatal sepsis and 5th-minute APGAR score of <7 had a 2.1 times higher hazard of mortality than preterm neonates who had an APGAR score >7 (AHR: 2.11 [95% CI: 1.29–3.46]). This is supported by studies conducted in China,24 Brazil,25 Iran,17 and the University of Gondar Hospital.19 This might be due to that neonates who were born with 5th minute APGAR score of <7 were severely asphyxiated and may end up with death.
This study was conducted by considering censoring and time to event using survival analysis and it was easy to establish a temporal relationship between the dependent and independent variables. The study used prospective data, and the better quality of data on the primary exposure and exposures are assessed before outcomes occur, hence there is less likelihood for bias. In addition, the study was conducted in multicenter settings using prospective follow-up, which increases the reliability and generalizability of data. Finally, the study has novel findings on an important topic that has not been explored before.
We had a relatively small sample size, which is difficult to generalize to all preterm neonates diagnosed with neonatal sepsis. Second, since the study was conducted among preterm neonates diagnosed with neonatal sepsis and were admitted to only government hospitals, it cannot be generalized to the preterm neonates admitted to private hospitals and healthcare centers.
In this study, preterm neonates diagnosed with neonatal sepsis showed a higher incidence of mortality than in other national and local studies, and the median survival time of neonates was 15 days during the hospitalization period. Born from a mother who did not have ANC follow-up, 5th-minute Apgar score <7, and having comorbidities such as RDS and jaundice were the independent predictors of mortality among preterm neonates diagnosed with neonatal sepsis. Therefore, healthcare professionals and other stakeholders should encourage mothers to attend antenatal care, work hard to diagnose accurately and provide therapeutic interventions for comorbidities of preterm neonates with neonatal sepsis, all of which could reduce the high incidence of mortality among preterm neonates diagnosed with neonatal sepsis.