Adequate knowledge about neonatal resuscitation plays a major role in early diagnosis and management to provide appropriate neonatal resuscitation interventions and prevent complications.
A cross-sectional study design was conducted among 151 nurses from Hebron, Palestine.
Only 9.3% of participants had standardized level of knowledge, while 68.9% reported adequate skills for neonatal resuscitation.
Factors associated with standardized level of knowledge were age and supportive supervision.
Factors associated with the standardized practice level were the presence of hospital guidelines, previous training of nurses, and presence of supportive supervision.
Globally, about 4 million newborn deaths occur each year, with 99% of these deaths occurring in low- and middle-income countries.1 Neonatal asphyxia has been identified as a leading cause of neonatal death world-wide, accounting for around 23% of all neonatal deaths.2
Newborn resuscitation is an immediate and important interventions to help newborns who have breathing and circulatory problems. The first few moments of a newborn’s life are considered one of the most important and dangerous moments; therefore, healthcare providers must provide urgent care and effective resuscitation to the newborn to prevent complications.3
In patients experiencing cardiac arrest, effective cardiopulmonary resuscitation keeps essential organs perfused and is associated with a higher survival rate and better neurological outcomes.4 In contrast to adult resuscitation, where chest compressions are the most crucial component, pediatric and neonatal resuscitation prioritize on ventilation.5 Circulatory support with chest compressions is also necessary to achieve meaningful performance if the heart rate is <60 beats per minute.6
Effective neonatal resuscitation is a major factor in reducing neonatal mortality rates. Approximately 10% of newborns require some form of resuscitation intervention immediately after birth and <1% need advanced neonatal resuscitation; therefore, adequate neonatal resuscitation knowledge and practice play an important role in identifying neonates who need resuscitation interventions and, thus, prevent complications.7 Neonatal resuscitation training for healthcare providers is critical given the high number of neonates who need help to breathe.8 Moreover, nearly 1 in every 10 neonates needs some kind of assistance such as tactile stimulation, airway clearing, or positioning.9
Available evidence suggests that effective neonatal resuscitation provided by skilled healthcare providers can significantly reduce neonatal mortality rates.1 However, knowledge of neonatal resuscitation may not always be optimal among healthcare providers. In countries such as Kenya, Eastern Ethiopia, and Poland, the majority of healthcare providers including nurses had a substandard level of knowledge about neonatal resuscitation.10–12 In contrast, nurses in countries such as Tanzania and Nigeria showed adequate knowledge about neonatal resuscitation.13,14 There is a variation in the reported outcomes of knowledge and practice regarding neonatal resuscitation among healthcare providers across the world. In Palestine, to the best of our knowledge, there are no published studies available on the topic of neonatal resuscitation knowledge and practices and associated factors among emergency nurses. Therefore, this study aimed to fill this literature gap.
A cross-sectional design was considered appropriate to assess the level of knowledge and practices toward neonatal resuscitation among emergency nurses. These nurses were recruited from five governmental hospitals in Hebron, located in the West Bank, Palestine.
The study population included all registered nurses employed in the emergency departments of selected hospitals in Hebron city. The sample size was 161 nurses. Ten nurses participated in a pilot study which was substantial for conducting independent sample t-test and one-way ANOVA that were needed to test factors associated with knowledge and practice toward Neonatal Resuscitation among nurses in Palestine. It is generally recommended to have at least 15 participants per group if the data are normally distributed.15 Participants were recruited using a convenience sampling technique. The inclusion criteria were nurses who had worked in emergency departments for at least six months and who could read, speak, and write in English.
Ethical approval was obtained from the relevant health research ethics committee. This study was approved by the ethics committee of Arab American University (IRB approval number: R\2023\A86\N). Additionally, permissions were granted from all selected hospitals to access potential participants. The researcher explained the study to the potential participants, and if they were interested to take part in the study, written consent was obtained. Finally, the researcher provided the selected participants with the data collection instrument to fill out on their own.
The data collection instrument included three sections: The first section was demographic data which included two parts: (i) providers’ characteristics (age, gender, and receiving resuscitation training at workplace) and (ii) institutional characteristics (availability of neonatal resuscitation guidelines, availability of supportive supervision, availability of neonatal resuscitation equipment).
The second section included an assessment of knowledge using 20 multiple-choice questions related to neonatal resuscitation, with each question having four possible options. Knowledge questions were scored either 1 or 0 for correct and incorrect responses, respectively. Nurses who scored >80% were considered to have adequate knowledge, while those who scored <80% were considered to have inadequate knowledge.7,10,16
The third section included an assessment of practice section. Practice questions were scored as either 1 or 0 for the done\not done responses, respectively. Nurses who scored >80% were considered to have a standardized level of practice, while those who scored <80% were considered to have a substandard level of practice, which has been used in different studies.16
The knowledge and practice scales were adopted from previous research including the following: World Health Organisation guidelines; the Ethiopian Pediatric Association Guideline and Training manual.7,10,16 The reliability of the instrument (internal consistency between the items) was tested during the present study showing an acceptable level of internal consistency (Cronbach’s alpha = 0.73).
The data were analyzed using the SPSS version 25 software. A set of descriptive and inferential statistics were conducted. Numeric variables (knowledge score, practice score, age) were described by means, standard deviation, minimum, and maximum, while categorical variables (knowledge level, practice level, some socio-demographic variables, and institutional variables) were described by frequencies and percentages. The relationships between knowledge score, practice score, and each of the institutional and socio-demographic variables were examined using two-independent samples test for dichotomous independent variables and one-way ANOVA for polytomous independent variables.
A total of 151 participants participated in this study with a response rate of 100%. Table 1 presents the demographics of the study participants.
Sociodemographic characteristics of the study participants.
| Variables and categories | Frequency (N) | Percentage (%) |
|---|---|---|
| Age (years), Mean = 29.08 ± 5.48, Range = (21–44) | ||
| Age categories in years | ||
| 20–29 | 94 | 62.3 |
| 30–39 | 51 | 33.8 |
| ≥40 | 6 | 4.0 |
| Gender | ||
| Male | 111 | 73.5 |
| Female | 40 | 26.5 |
| Educational level | ||
| Diploma | 25 | 16.6 |
| Bachelor | 105 | 69.5 |
| Master and higher | 21 | 13.9 |
| Resuscitation Training | ||
| Yes | 108 | 71.5 |
| No | 40 | 26.5 |
| Type of hospital | ||
| Private hospital | 29 | 19.2 |
| Referral hospital | 43 | 28.5 |
| Public hospital | 79 | 52.3 |
| Full resuscitation material | ||
| Yes | 132 | 87.4 |
| No | 19 | 12.6 |
| Resuscitation guideline | ||
| Yes | 90 | 59.6 |
| No | 61 | 40.4 |
| Supportive supervision | ||
| Yes | 105 | 69.5 |
| No | 46 | 30.5 |
This study showed that 137 (90.7%) participants had a substandard level of knowledge toward neonatal resuscitations. The mean of the correct answers across 20 questions was 9.6. Figure 1 shows the distribution of answers to neonatal resuscitation knowledge questions.
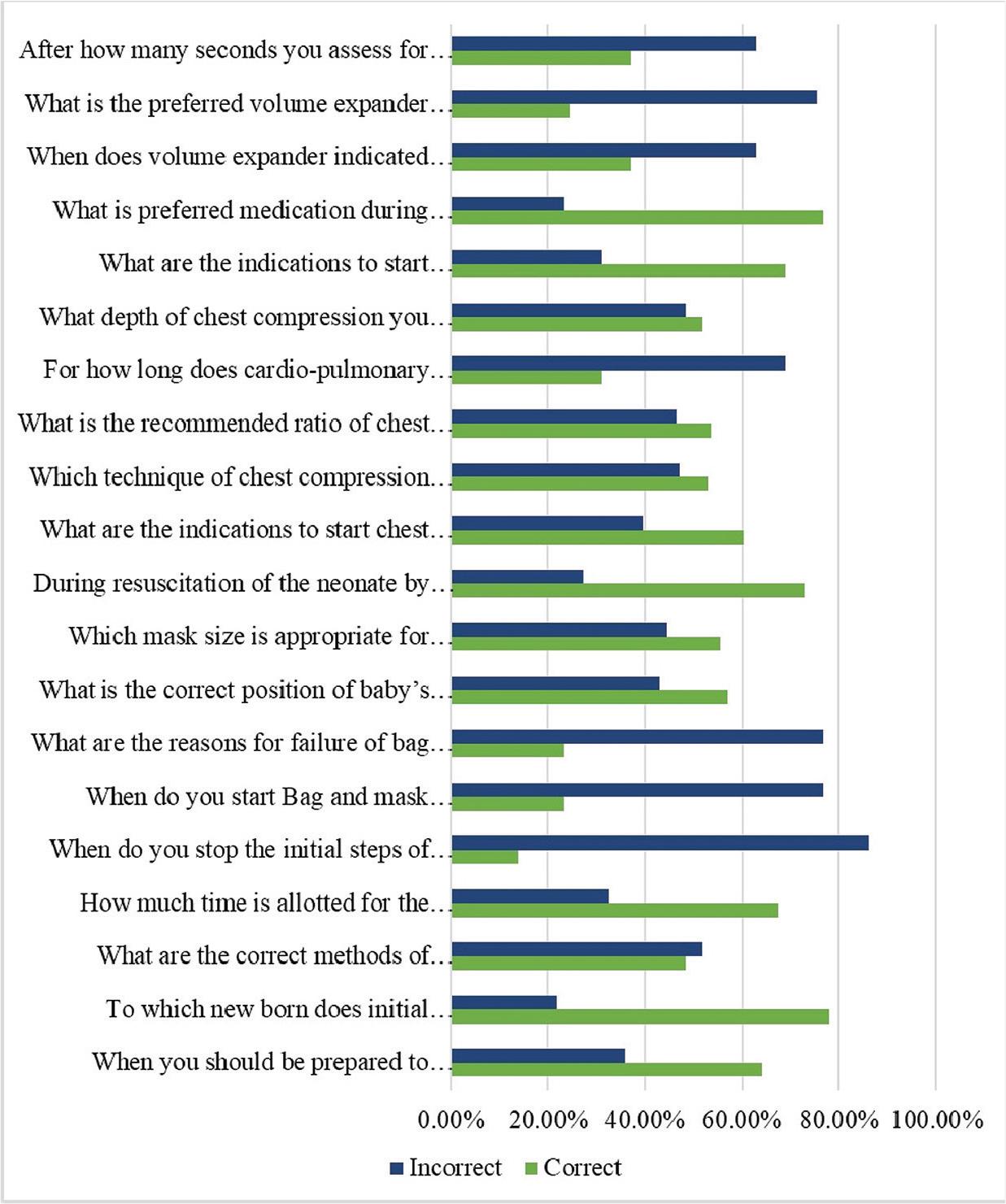
Distribution of answers to neonatal resuscitation knowledge questions.
This study also revealed that the majority of participants (68.9%) had a standardized level of practice toward neonatal resuscitation. The mean of the overall practice score was 84.76%. Figure 2 shows the mean practice scores (%) toward neonatal resuscitation practice questions.
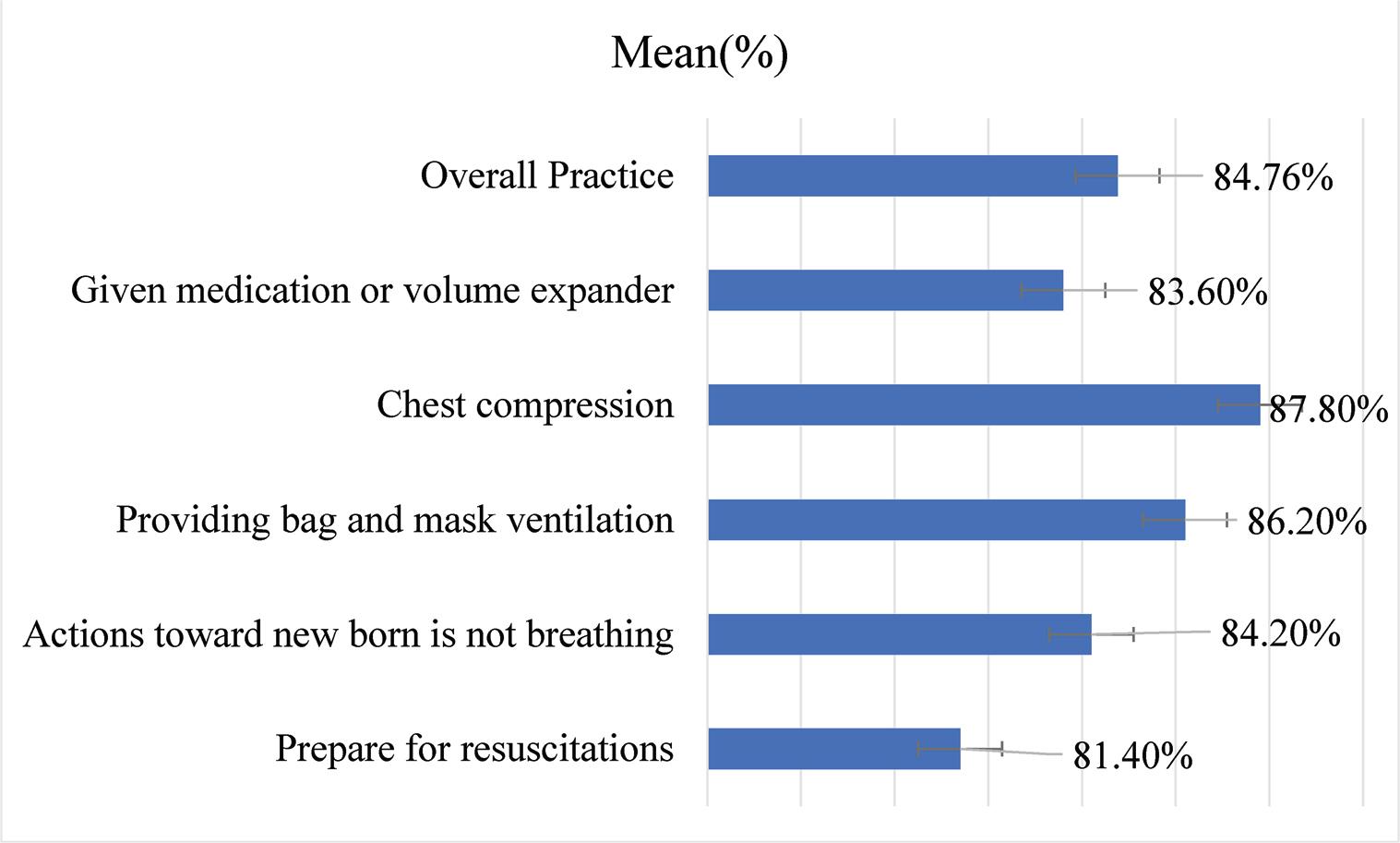
Mean practice scores (%) for neonatal resuscitation.
Bivariate testing showed that age and supportive supervision were associated with a higher level of knowledge (both p< 0.05), while the availability of either guidelines or supervision was associated with standardized practice (both p< 0.05; Tables 2 and 3).
Factors associated with participants’ knowledge toward neonatal resuscitation.
| Variables and categories | Mean (%) | SD (%) | T/F value | p-Value | Test used |
|---|---|---|---|---|---|
| Provider characteristics | |||||
| Age, R = 0.47 | 0.001* | Bivariate correlation | |||
| Age categories in years | 7.868 | 0.001* | One Way-ANOVA | ||
| 20–29 | 43.56 | 17.89 | |||
| 30–39 | 55.39 | 18.99 | |||
| ≥40 | 58.33 | 18.88 | |||
| Gender | 1.41 | 0.16 | Independent T-Test | ||
| Male | 49.45 | 18.15 | |||
| Female | 44.50 | 21.41 | |||
| Educational level | 1.87 | 0.15 | One Way-ANOVA | ||
| Diploma | 51.80 | 23.49 | |||
| Bachelor | 46.19 | 17.34 | |||
| Master and higher | 53.57 | 21.22 | |||
| Resuscitation training | –0.10 | 0.91 | Independent T-Test | ||
| Yes | 48.37 | 19.53 | |||
| No | 48.75 | 17.78 | |||
| Institutional characteristics Type of hospital | 1.04 | 0.35 | One Way-ANOVA | ||
| Private hospital | 45.34 | 19.86 | |||
| Referral hospital | 51.51 | 21.67 | |||
| Public hospital | 47.34 | 17.29 | |||
| Full resuscitation Material | 1.63 | 0.10 | Independent T-Test | ||
| Yes | 49.24 | 19.19 | |||
| No | 40.93 | 18.72 | |||
| Resuscitation guideline | 0.18 | 0.85 | Independent T-Test | ||
| Yes | 48.66 | 19.26 | |||
| No | 48.05 | 18.61 | |||
| Supportive supervision | 0.29 | 0.007 | Independent T-Test | ||
| Yes | 48.80 | 18.62 | |||
| No | 44.79 | 19.94 | |||
Note: Statistically significant difference at α ≤ 0.05.
Factors associated with participants’ practice toward neonatal resuscitation.
| Variables and categories | Mean (%) | SD (%) | T/F value | p-Value | Test used |
|---|---|---|---|---|---|
| Provider characteristics | |||||
| Age, R = 0.13 | 0.10 | Bivariate correlation | |||
| Age categories in years | 0.72 | 0.48 | One way-ANOVA | ||
| 20–29 | 83.74 | 14.83 | |||
| 30–39 | 86.11 | 14.82 | |||
| ≥40 | 89.33 | 14.67 | |||
| Gender | 0.63 | 0.52 | Independent t-test | ||
| Male | 85.22 | 14.35 | |||
| Female | 83.50 | 16.08 | |||
| Educational level | 0.81 | 0.44 | One way-ANOVA | ||
| Diploma | 83.04 | 14.34 | |||
| Bachelor | 84.45 | 14.77 | |||
| Master and higher | 88.38 | 15.58 | |||
| Resuscitation training | 0.58 | 0.011 | Independent t-test | ||
| Yes | 88.44 | 15.24 | |||
| No | 77.22 | 13.01 | |||
| Institutional characteristics Type of hospital | 1.28 | 0.28 | One way-ANOVA | ||
| Private hospital | 85.24 | 14.34 | |||
| Referral hospital | 87.53 | 12.59 | |||
| Public hospital | 83.08 | 15.96 | |||
| Full resuscitation material | 1.95 | 0.06 | Independent t-test | ||
| Yes | 86.00 | 14.64 | |||
| No | 78.50 | 12.97 | |||
| Resuscitation guideline | -0.08 | 0.028 | Independent t-test | ||
| Yes | 87.71 | 15.64 | |||
| No | 76.67 | 13.72 | |||
| Supportive supervision | 0.27 | 0.000 | Independent t-test | ||
| Yes | 88.43 | 15.26 | |||
| No | 67.33 | 13.51 | |||
This study aimed to assess the level of knowledge and practice toward neonatal resuscitation among emergency nurses in Hebron hospitals in the West Bank. The results of this study showed that the reported knowledge levels by the majority of nurses was inadequate –90%, and –70% of nurses reported adequate skills for neonatal resuscitation. The suboptimal level of knowledge among the study population indicates an urgent need for providing continued professional development and training about neonatal resuscitation for emergency nurses in Hebron.
The results of the current study mirrored the results of previous studies. Several studies also reported a substandarized level of knowledge among healthcare providers Kenya, Baghdad, Parsa District and Ethiopia.10,16–18 Similarly, studies from Ethiopia and India found low knowledge scores (49.3% and 57%) respectively.16,19
The study results also showed a significant association between the knowledge score and age of the participants. A previous investigation by Gauro et al. (2018) conducted in Parsa District did not find a significant association between knowledge score and age, while total working experience was a significant factor.18 Therefore, the currently available evidence shows that age and duration of working experience seem to be important factors that contribute to enhancing the level of knowledge among nurses.
The mean practice score of nurses was 84.7% in the current study. This was a higher level than the results of a study from Gondar Teaching Hospital 55.8%.16 Another study from Nigeria also reported a much lower level of neonatal resuscitation practice, with only 10% of nurses had a high level of practice.14 Similarly, a study from Iran showed that 84.6% of participants had a substandard level of skills in neonatal resuscitation.20 The inconsistency in performance and levels of practice toward neonatal resuscitation could be due to differences in the quality of training, supportive supervision, and availability of neonatal resuscitation guidelines.
The study results also showed a significant relationship between practice scores and receiving previous resuscitation training at the workplace. A previous study that was conducted in Addis Ababa reported similar results to the current study, in which a significant relationship between practice score toward neonatal resuscitation and previous training was also found (p = 0.011).3 We recommend continuous professional development, including providing adequate training for emergency nurses about neonatal resuscitation.
The results also showed that the availability of neonatal resuscitation guidelines or supportive supervision was significantly associated with a higher level of resuscitation practice among nurses in Hebron hospitals. The availability of resuscitation guidelines in the workplace can help nurses to adhere to these guidelines during routine practice, and this may result in standardized neonatal resuscitation practice. Supportive supervision, on the other hand, can improve the practice level of nurses progressively by reducing the gap between time and practice.
Finally, this study showed an interesting observation that is worth highlighting. Although the study participants reported high scores of knowledge about neonatal resuscitation guidelines, the reported level of practice was low. This contradiction between knowledge and practice demonstrates the complexity of nurses’ practice behaviour, this can be impacted by a complexity of several personal or environmental factors and nurses’ knowledge might not predict their practices. However, a recent systematic review found that nurses’ knowledge can be a significant predictor of their practice, and this is not in line with our findings in which the study participants had high knowledge and low scores of practice.21 We recommend future research to test the association between nurses’ knowledge and their practice.
This study has the following strengths. First, we believe that the provided data present the first available evidence about the levels of knowledge and practice towards neonatal resuscitation guidelines among emergency nurses in Palestine. Second, the sample size was substantial to test the factors associated with the main outcome of this study. Lastly, data were collected from five hospitals, delivering a more representative sample of the emergency nurses’ population in Palestine. However, this study is not exempt from some limitations. First, the assessment of practice used an interview guide rather than an observational checklist. Second, knowledge was assessed using self-administered questionnaires which may result in information bias. Third, the sample size was relatively small to represent the target population. Fourth, the study tool was used without official testing of validity, and it is recommended to validate this tool in future research.
The majority of emergency nurses in Hebron hospitals demonstrated a low level of knowledge of neonatal resuscitation, but most of them had an adequate level of practice. Offering resuscitation training programs, supervision, and neonatal resuscitation guidelines for nurses can be promising to improve the knowledge and practice of neonatal resuscitation.