Physical assessment is a fundamental skill that nurses use to evaluate and monitor patients with diverse medical conditions. Assessment is the initial step in the nursing process, playing a crucial role in delivering nursing care1,2 and serving as the primary standard of critical care nursing practice.3 This is a fundamental and dynamic method for collecting and analyzing patient information. The key to develop a dependable nursing care plan lies in the precise collection of data through physical assessments. As part of their routine, nurses are required to conduct a comprehensive assessment of their patients when receiving them from shift nurses. This step is of utmost importance in identifying the nursing requirements of the patient and assumes greater significance in critical care units, which are characterized by patients with multiple and intricate health conditions. The escalating acuity of care and rapid progression of technologies have posed novel challenges for the nursing profession.
The National Health Service (NHS) plan emphasizes the necessity of changes to address these demands, particularly in the domain of physical assessment.4 To effectively address patients’ needs, thorough and proficient physical assessment is essential. Furthermore, it aids in identifying and resolving the underlying health issues in patients. Nurses spend more time to patients compared to any other healthcare provider, thereby shouldering greater responsibility. Therefore, higher expectations are placed on nurses. The evolving responsibilities of nurses have introduced numerous challenges, particularly within the intricate setting of critical care units.5 A study conducted among cardiac nurses highlighted the crucial influence of professionalism, personal characteristics, organizational structure, professional relationships, and the role of health assessment in the utilization of physical assessment skills.6,7
A descriptive study revealed that only 29% of acquired health assessment skills were implemented on daily or weekly basis.8 These findings raise concerns regarding the provision of safe and high-quality patient care. Therefore, the diligent and thoughtful application of assessment skills is paramount. It is essential to acknowledge the significance of patient data, as it forms the foundation for treatment and care planning. A lack of comprehensive patient information is problematic. When providing care to elderly patients with chronic illnesses, nurses may encounter challenges in comprehending the relationship between the diagnosis, unfavorable or uncertain prognosis, and treatment plans.9,10 This lack of understanding can affect clinical outcomes, which not only places a financial burden but also imposes significant stress on patients, family members, and nurses. Furthermore, the study highlighted that inappropriate physical assessment in critical care units may result in the overestimation or underestimation of survival rates. This, in turn, can lead to nurses feeling responsible for causing unnecessary suffering in patients who they believe will not survive hospitalization.11
Insufficient attention to detailed physical assessments can result in substandard care and negatively impact the patient’s pathophysiological adaptation. Therefore, the availability of comprehensive and trustworthy patient information is crucial, with physical assessment serving as a fundamental source for building a robust database to inform treatment decisions and interventions. Acquiring this skill is vital for all nurses to enhance patient care.5 A previous study has suggested that analyzing the utilization of physical assessment in the respiratory unit could potentially enable earlier recognition of pre-arrest symptoms.12,13 Therefore, the primary objective of this study was to assess physical assessment practices among critical care nurses, while the secondary objective was to determine any differences based on nurses’ educational levels.
A descriptive cross-sectional research design was employed for this study, which was conducted at a private internationally accredited tertiary care hospital in Islamabad, Pakistan, from March to October 2021. The hospital has a total inpatient capacity of >550 beds and 26 operating rooms. The critical care unit includes 100 beds and accommodates medical, surgical, neurosurgical, and coronary care patients.
This study included nurses who were directly involved in the patients’ care in critical care units. Nurses in management positions were excluded from the study as they did not provide direct patient care. Additionally, nurses in their probationary period were excluded because they were new to the critical care units and may not have been fully acquainted with the policies and procedures.
The sample was calculated with the OpenEpi calculator with a finite population correction factor of N = 150, and the hypothesized % of outcome factor in the population P=50% and 95% confidence interval determined the sample of 109 nurses using the following formula: n = [DEFF × Np(1-p)]/[(d2/Z21-α/2 × (N-1) + p × (1-p)].
Simple random sampling was used for participant selection. First, a list of eligible participants was created and assigned a unique serial code. Next, a list of 109 participants was generated using the (=RANDBETWEEN) formula in Microsoft Excel.
The instrument used in this study included demographic information such as gender and professional degree. The second section of the instrument consisted of a standard comprehensive physical assessment checklist. This checklist includes components such as hand washing, introduction to the patient, general survey, vital signs, orientation, pupils, neck veins, skin, peripheral edema, bilateral checks, Homan’s signs, pain assessment, breath sounds, heart sounds, bowel sounds, and closure. Each item on the checklist was rated on a 3-point Likert scale, with a rating of 1 indicating correct performance, a rating of 0.5 indicating incorrect performance, and a rating of 0 indicating nonperformance.
The data were collected by 2 research team members. Before data collection, inter-rater reliability was established and calculated to be 0.82 using the Fleiss’ Kappa, ensuring consistency in data collection.14 Data collection took place in a simulated environment of the nursing education services department’s skills lab, which was chosen to prevent any interference with routine activities in the patient care unit. The nurses were given a real-life case from the critical care unit and asked to perform a comprehensive physical assessment.
Data were coded and entered into the Statistical Package for Social Sciences (SPSS v25.0, IBM Corporation, Armonk, New York, United States) for analysis. Demographic information is presented as frequencies and percentages. The performance checklist was scored as a percentage on a Likert-type scale. For inferential statistics, chi-squared and Fisher’s exact tests were applied to compare performance in health assessment skills among nurses based on their gender and type of education.
Of the 109 eligible critical care nurses, 101 participated in the study, resulting in a response rate of 92.6%. Among the total sample, 56.4% were female and 43.6% were male. Furthermore, 71.0% of the nurses held a diploma and 29.0% had obtained a Bachelor of Science in Nursing (BSN).
There were varying percentages of correctly performed health assessment components, and none of the skills achieved 100% accuracy. However, the assessment of vital signs, orientation, and skin showed correct performance rates of ≥90% for the 16 components. On the contrary, the majority of nurses (≥60%) did not perform assessments of neck veins, Homan’s signs, breath sounds, heart sounds, or bowel sounds. Only ≤10% of the nurses who performed these components executed them correctly, whereas the rest performed them incorrectly (Table 1).
Descriptive evaluation of physical assessment by critical care nurses (n = 101).
| Components | Correct (%) | Incorrect (%) | Not performed (%) |
|---|---|---|---|
| Hand washing | 69.1 | 12.7 | 18.2 |
| Introduction to patient | 80.0 | 5.5 | 14.5 |
| General survey | 81.8 | 12.7 | 5.5 |
| Vital signs | 96.4 | 3.6 | 0.0 |
| Orientation | 92.7 | 7.3 | 0.0 |
| Pupils (PERRLA) | 81.8 | 9.1 | 9.1 |
| Neck veins | 3.6 | 20.0 | 76.4 |
| Skin | 94.5 | 3.6 | 1.8 |
| Peripheral edema | 89.1 | 7.3 | 3.6 |
| Bilateral checks | 74.5 | 10.9 | 14.5 |
| Homan’s signs | 10.9 | 16.9 | 72.7 |
| Pain | 65.5 | 29.1 | 5.5 |
| Breath sounds | 1.8 | 7.3 | 90.9 |
| Heart sounds | 1.8 | 1.8 | 96.4 |
| Bowel sounds | 23.6 | 16.4 | 60.0 |
| Closure | 67.3 | 7.3 | 25.5 |
Note: PERRLA, Pupils Equal Round Reactive to Light Accommodation.
Chi-squared and Fisher’s exact tests were performed to compare the proportions of health assessment components among the different sex and nursing degree groups. Statistical significance was set at P < 0.05. The results revealed that only the pain component showed a significant difference in performance between male and female nurses, with females demonstrating better performance. The bilateral check component showed a moderate level of significance, while the remaining components did not show any significant differences between the sex groups. In terms of nursing degrees, the only significant component was the closure of the health assessment, where a difference was observed between nurses with diplomas and those with degrees in nursing. The vital sign component showed a weak correlation, while the other health assessment components showed no significant differences (Table 2).
Comparison of nurses’ physical assessment performance by gender and type of nursing degree (N = 101).
| Components | Sex | Professional qualification | ||||
|---|---|---|---|---|---|---|
| Male (%) | Female (%) | P-value | Diploma (%) | BSN (%) | P-value | |
| Hand washing | 58.3 | 77.4 | 0.129 | 69.2 | 68.8 | 0.972 |
| Introduction to patient | 70.8 | 87.1 | 0.180 | 79.5 | 81.3 | 1.00 |
| General survey | 79.2 | 83.9 | 0.733 | 82.1 | 81.3 | 1.00 |
| Vital signs | 91.7 | 100.0 | 0.186 | 100.0 | 87.5 | 0.081 |
| Orientation | 91.7 | 93.5 | 1.00 | 92.3 | 93.8 | 1.00 |
| Pupils (PERRLA) | 79.2 | 83.9 | 0.733 | 84.6 | 75.0 | 0.453 |
| Neck veins | 4.2 | 3.2 | 1.00 | 2.6 | 6.3 | 0.501 |
| Skin | 91.7 | 96.8 | 0.575 | 97.4 | 87.5 | 0.200 |
| Peripheral edema | 91.7 | 87.1 | 0.686 | 87.2 | 93.7 | 0.660 |
| Bilateral checks | 62.5 | 83.9 | 0.071 | 71.8 | 81.3 | 0.734 |
| Homan’s signs | 4.2 | 16.1 | 0.216 | 12.8 | 6.3 | 0.478 |
| Pain | 50.0 | 77.4 | 0.034 | 66.7 | 62.5 | 0.768 |
| Breath sounds | 0.0 | 3.2 | 1.00 | 2.56 | 0.0 | 1.00 |
| Heart sounds | 0.0 | 3.2 | 1.00 | 2.56 | 0.0 | 1.00 |
| Bowel sounds | 25.8 | 20.8 | 0.667 | 20.5 | 31.5 | 0.395 |
| Closure | 58.3 | 74.2 | 0.214 | 62.2 | 37.8 | 0.041 |
Note: PERRLA, Pupils Equal Round Reactive to Light Accommodation; P < 0.05.
The average total score for nurses in health assessment skills was 9.4 ± 2.5. Female nurses (10.0 ± 2.3) obtained a significantly higher score (P=0.03) than male nurses (8.5 ± 2.5). On the contrary, nurses with a diploma in nursing (9.4 ± 1.8) achieved a slightly higher score, though not statistically significant (P=0.860), than nurses with a Bachelor of Science in Nursing (BSN) degree (9.3 ± 2.7) (Figure 1).
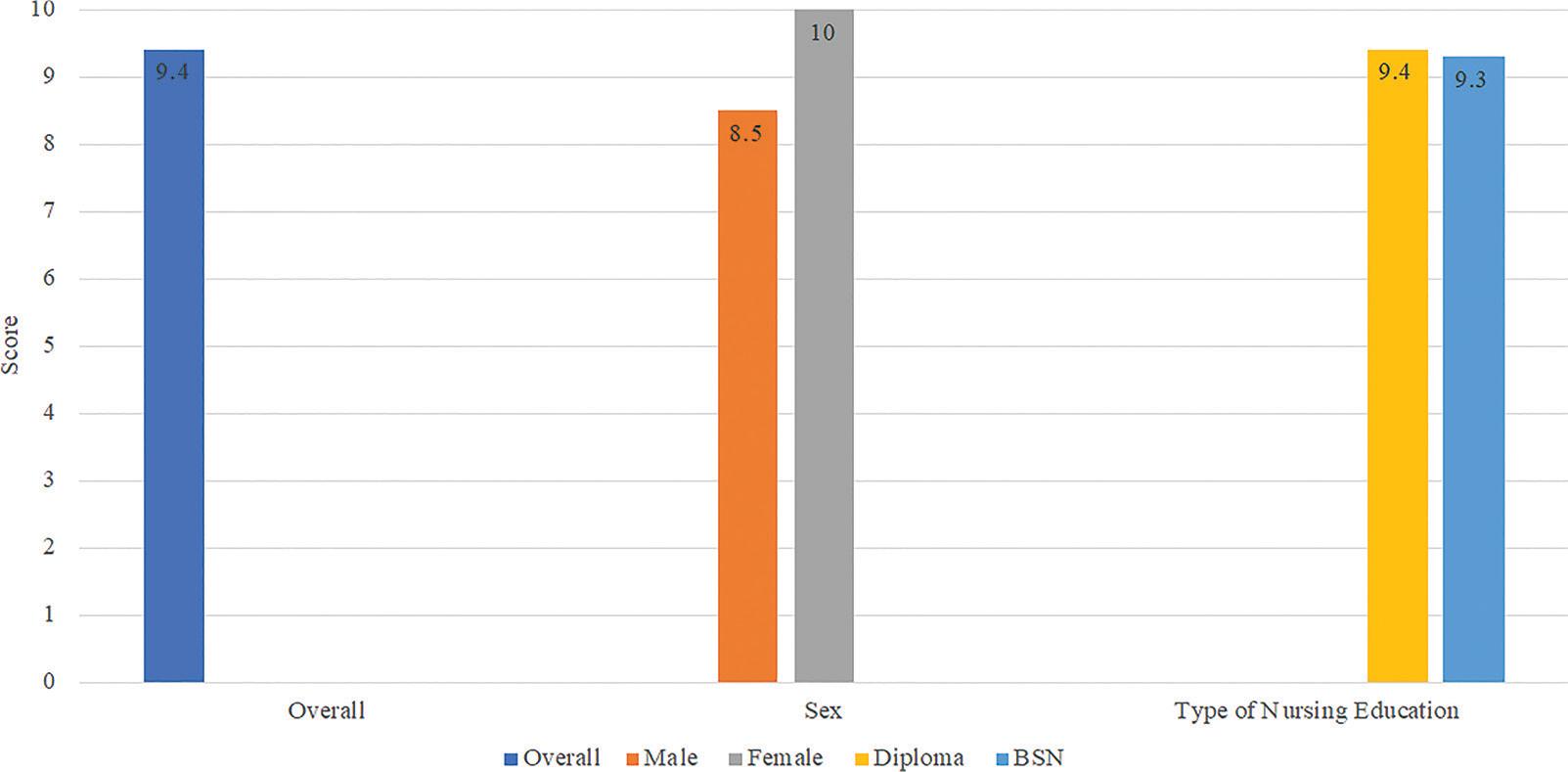
Average total physical assessment score of nurses by gender and education type.
The findings revealed that the majority of nurses demonstrated proficient performance in various components of health assessment, including hand washing, general surveys, vital signs, orientation, pupil assessment, skin evaluation, peripheral edema assessment, bilateral checks, pain assessment, and communication. These components are routinely recorded by nurses on an intensive care flow sheet, with assessments conducted every hour. The repetitive nature of these assessments may have contributed to the nurses’ high level of proficiency. Additionally, these components do not require specialized techniques for physical assessment, which likely enables the majority of nurses to perform them accurately.
A previous study discussed the importance of deliberate practice in improving participants’ task performance abilities.15 Nevertheless, it is worth noting that a small number of nurses experienced difficulties in accurately performing these physical assessment components.
The standard nurse-to-patient ratio in critical care units is typically 1:1. This ratio is based on the complexity of critical illness and the attention required by each patient. As a result, nurses have a significant level of accountability for the care they provide. It is essential for them to accurately assess patients’ needs for planning and delivering evidence-based care.16,17 Each piece of patient information plays a crucial role in understanding their condition and monitoring their progress. Insufficient information poses a risk to patients as it can lead to inadequate care, hinder problem identification, and impede the timely prevention of complications. To ensure safe and comprehensive care, it is vital to address gaps in patient information.
There were certain physical assessment components that the majority of nurses did not assess accurately, such as breath, heart, and bowel sounds; neck veins; and Homan’s signs. Perhaps, these assessment components are not routinely performed by nurses. As a result, nurses’ performance in these components was low. However, these components provide valuable information to nurses regarding their cardiovascular and respiratory systems. It is important to note that respiratory disorders are one of the most common reasons for admission to critical care units.18 Interestingly, the study findings indicate that only a minimal percentage (1.8%) of nurses performed assessments of breath sounds, which are often overlooked. This suggests that the nursing assessment of respiratory function is not given sufficient priority, and the implications of respiratory dysfunction may be underestimated.19 Another contributing factor to the omission of these components could be that house officer doctors perform auscultation as part of their physical assessment and management. As both nurses and doctors are involved in health assessments for patient monitoring and assessment, this may lead to role ambiguity in patient care. Clearly, a multidisciplinary collaborative physical assessment is needed for comprehensive and accurate physical assessment.
It is imperative to acknowledge that nurses need knowledge and training to improve their skills in areas where they score lower. Without proper training and ongoing education, it is challenging to accurately perform health assessments. The continuous evolution of technology has greatly impacted the nursing profession, necessitating nurses to stay updated with these changes, as they directly affect their patients’ outcomes. Therefore, it is the responsibility of every nurse to prioritize ongoing learning and remain updated to provide the best possible care to their patients.20 Failure to conduct a thorough and precise physical assessment may result in missed opportunities for nursing care interventions that are essential for patient well-being. Physical assessment serves as the foundation for identifying patient problems, formulating diagnoses, and planning appropriate care and treatment strategies. Hence, it is crucial to approach physical assessments with meticulousness, awareness, and a comprehensive perspective.
This study findings further revealed that female critical care nurses demonstrated superior performance in physical assessments compared with their male counterparts. This may be attributed to factors, such as heightened focus and experience among female nurses, resulting in elevated performance. It is important to note that providing collegial support to male nurses could contribute to improving their physical assessment skills. However, no statistically significant difference was found in the educational qualifications of the nurses. Despite variations in qualifications, all nurses served the patients at equal levels. Previous research highlights the impact of experiential learning and workplace environments on skills development.21 Additionally, it is plausible that nurses with a diploma in nursing have undergone professional development training, which could enhance their physical assessment abilities. Incorporating the teaching of physical assessment skills within a holistic health model has the potential to empower nurses to provide a more comprehensive health assessment for the purpose of planning and monitoring individuals’ healthcare.22,23
This study had a few limitations that need to be acknowledged. First, data collection was conducted solely in a private-sector hospital, which restricts the generalizability of the study findings to a broader population. Therefore, it is recommended to conduct a multihospital study involving both the public and private sectors, with a larger sample size, to enhance the generalizability of the results. Despite these limitations, this study provided valuable insights into the physical assessment practices of critical care nurses. The utilization of a simple random sampling methodology is a notable strength of this study, as it helps ensure an unbiased selection of participants and enhances the reliability of the findings.
The findings of this study have implications for nursing practice, competence development of nurses, nursing management, and future research. Insufficient physical assessment is a threat to patient safety and the provision of quality care. An interprofessional physical assessment course could improve physical assessment and collaboration between nurses and doctors. Nursing management should provide opportunities for professional development, and future research should focus on patient outcomes and strategies to improve physical assessment practices.
This study identified notable deficiencies in the physical assessment practices employed by critical care nurses. These gaps have significant implications with the potential to adversely affect patient outcomes. Consequently, it is imperative for nurses to enhance their physical assessment practices through targeted improvement. Nursing management plays a crucial role in this process as it should actively facilitate opportunities for professional development aimed at enhancing physical assessment skills. Nurses are urged to practice to the fullest extent possible, pursue higher levels of education and training, establish collaborative partnerships with other healthcare professionals, foster continuity of education, and implement effective workforce planning and policymaking strategies.