
Angiotensin II type 2 receptors (AT2Rs) are found in most organs. The expression of AT2Rs was detected with the use of immunochemistry in the human kidneys (vessels and glomeruli, Mifune et al. 2001).
Even though angiotensin II type 1 receptor (AT1R) shows vasoconstrictive activity, AT2R has vasodilatation activity (Savoia et al. 2011). The activity of AT2R is revealed after AT1R blockade. AT2R also dilates microvasculature, which is notably expressed in diabetic mice (Begorre et al. 2017). It was found that AT2Rs are also a factor engaged in the regulation of the kidney glomerular capillary wall permeability (Suzuki et al. 2007) and interactions between leukocytes and endothelium through a mechanism connected with P-selectin (Piqueras et al. 2000). AT2Rs are also involved in the control of cellular differentiation, hypertrophy, and proliferation (through regulation of SM 20; Wolf et al. 2002) and nitric oxide production. The function of AT2R is contrary to AT1R activity in these areas (Siragy 2000). AT2R activation also has a positive effect on fibrosis (Naito et al. 2010) and improves lipid metabolism (Nag et al. 2019) and insulin resistance (Shum et al. 2013). The AT2R enables flow-mediated remodeling of arteries through interleukin (IL)-17 produced by T cells (Caillon et al. 2016). Another process influenced by AT2R regulation is angiogenesis. Regulation is connected with the heparin-binding epidermal growth factor-mediated epidermal growth factor receptor (Yahata et al. 2006), angiopoietin 2 (Houston et al. 2017), and the vascular epidermal growth factor (Mishra et al. 2022). Moreover, AT2Rs are engaged in the regulation of NaCl absorption in the thick ascending limbs of the loop of Henle (Hong and Garvin 2012), bicarbonate absorption (Haithcock et al. 1999), and ammonia production and secretion in proximal tubules (Nagami et al. 2014). AT2R controls natriuresis together with the Mas receptor and the NaH exchanger (Zhuo and Li 2019). A positive correlation between levels of estrogens and AT2R expression was found; therefore, sex seems to influence AT2R expression (Sampson et al. 2008). AT2R is also associated with the regulation of apoptosis (Suzuki et al. 2002).
AT2Rs present in the nucleus of rat kidney glomerular and tubulointerstitial cells are associated with the control of nitric oxide production. This mechanism may be connected with blood pressure regulation (Gwathmey et al. 2009).
AT2R activation also preserves megalin and prevents proteinuria in high-salt diet-fed rats (Kulkarni et al. 2023). G protein-coupled receptor kinase 4 causes AT2R dysfunction and induces sodium retention and hypertension in a rat model (Zhang et al. 2022). AT2R also influences the development of the kidneys (Yanofsky et al. 2021). AT2R deficiency was connected with podocyte loss and impaired glomerulo-genesis in a mouse model (Liao et al. 2017).
AT2R activity resulted in a reduction in extracellular signal-regulated kinase protein and mRNA of monocyte chemoattractant protein (MCP)-1 in a model of anti-glomerular basement membrane mice nephritis (Okada et al. 2006).
The AT2R activation induces Treg cells in the late phase of the model of kidney injury and ameliorates kidney injury in this model through an increase in IL-10 and an amelioration of IL-6 and MCP-1 (Ali et al. 2021).
The AT2R also has a positive effect on lipopolysaccharide-induced acute kidney injury through the activity of tumor necrosis factor (TNF)-α (Fatima et al. 2023).
The AT2R shows some anti-inflammatory properties through its influence on lipopolysaccharide-activated acute monocytic human leukemia (THP-1) macrophages via IL-10 (Dhande et al. 2015).
The activation of AT2Rs ameliorates podocyte injury in a model of focal and segmental glomerulosclerosis in mice (Liao et al. 2022).
Specific polymorphisms of the AT2R were found in Egyptian children with lupus. The serum level of angiotensin-converting enzyme (ACE) was higher in these patients compared to a control group, but there was no association between this level and AT2R polymorphisms (Shoaib et al. 2019).
The arteries in nasal lesions of patients with granulomatosis with polyangiitis (antineutrophil cytoplasmic antibodies [c-ANCA] positive vasculitis) had a reduced expression of AT2Rs (Dimitrijevic et al. 2011).
Orally active compound 21 is an agonist of AT2R. Compound 21 had a renoprotective effect in treated rats: it ameliorated glomerulosclerosis, interstitial fibrosis, visceral epithelial cell hypertrophy, and tubular atrophy (Patel et al. 2016). The activation of the AT2R by compound 21 decreased IL-6 and TNF-α renal levels and increased nitric oxide and cyclic guanosine monophosphate (cGMP) levels (Matavelli et al. 2015). Compound 21 also had an anti-inflammatory effect through an increase of IL-10, a decrease of CD 68+ (Dhande et al. 2013) and CD 11b+, and an amelioration of increased levels of IL-6 and MCP-1 (Patel et al. 2019). Relaxin also attenuates kidney fibrosis through the AT2R pathway (Barsha et al. 2021). Roxadustat has a positive effect on hypertension through its influence on AT1Rs and AT2Rs (Yu et al. 2021). Another newly developed agonist of the AT2R, beta pro7 angiotensin III, reveals a positive effect on the cardiovascular system through the limitation of fibrosis, reduction of inflammation, and decrease of superoxide levels (Li et al. 2023). Also, vitamin D seems to influence AT1Rs and AT2Rs. This action is connected with positive results in metabolic syndrome (Mohater et al. 2023). Olodanrigan is another drug acting specifically on the AT2R receptor (Huerta et al. 2023). The possibility of a specific treatment strengthened the significance of the evaluation of AT2R and AT2R antibodies in a variety of diseases. Specific investigations should help to find indications for these drugs and to identify groups of patients and diagnoses for which this treatment will be the most accurate.
AT2R antibodies were first described by Liles et al. (2015) as an autoantibody in rabbits immunized with fragments of AT2R. The AT2R antibody did not change the blood pressure of these animals, but their presence diminished the vasoconstrictive reaction after angiotensin II infusion. The same group found that people with primary hyper-aldosteronism had higher AT2R antibody levels than healthy people. AT2R antibodies were also detected in healthy people. There, the origin of these antibodies is unknown.
Next, it was found that people with chronic heart failure had higher AT2R antibody levels than healthy people (Zweck et al. 2023).
Currently, there is no data about the levels of these antibodies in kidney diseases.
This study evaluates AT2R antibody levels in serum samples from patients with different types of primary and secondary glomerular diseases. This study aimed to check if AT2R antibody levels differed between glomerular diseases and a healthy control group. Moreover, we planned to check the differences in AT2R antibody levels among specific glomerular diseases. We also planned to make an observation of the clinical parameters after the evaluation of the AT2R antibody to check if the level of this antibody has some influence on the clinical course of specific glomerular diseases. AT2R antibodies could potentially be a marker for a worse or better prognosis. Moreover, high-basic AT2R antibodies could potentially influence treatment with ACE inhibitors and other drugs that act on the renin-angiotensin-aldosterone system. Additionally, we would like to compare AT2R and AT1R antibody levels in specific diseases because the authors had data about AT1R antibody levels from the same patients from their previous study (Szymczak et al. 2022). These antibodies may mutually influence each other.
The anti-inflammatory properties of AT2R suggest that high levels of AT2R antibodies may be found in active inflammatory processes, so we assumed that there would be higher AT2R antibody levels in lupus nephritis and systemic vasculitis.
A total of 136 patients with various glomerular diseases were included in this study. All the patients had histopathologically proven glomerulopathy on kidney biopsies. The included patients were divided into separate groups: 18 patients had membranous nephropathy (Group 1: 6 patients with positive and 12 patients with negative anti-phospholipase A2 receptor antibodies), 25 patients had focal and segmental glomerulosclerosis (Group 2), 17 patients had systemic lupus erythematosus (Group 3), 14 patients had IgA nephropathy (Group 4), 6 patients had mesangial proliferative non-IgA glomerulonephritis (Group 5), 40 patients had c-ANCA vasculitis (Group 7), and 16 patients had p-ANCA vasculitis (Group 8). We included 22 healthy people as a control group (Group 6). Patients with other glomerulopathies were not included. All patients had proteinuria in the last available urine sample before collecting the material to perform this study. Declarations of informed consent were obtained from all the recruited patients before their inclusion in the study. Serum and urine samples were collected from recruited patients. There was no randomization in this study. Patients were hospitalized because of an initial manifestation of glomerulopathy. The samples were collected before the start of immunosuppressive treatments.
The exclusion criteria included dialysis, kidney transplantation, malignant neoplasms in the period of material collection, before the moment of material collection and during 2 years after its collection, and active infection around the time of sample collection. Procalcitonin levels of all patients were lower than 0.1 ng/mL, and the C-reactive protein of all the patients with glomerulonephritis was lower than 5 mg/L. We found 138 patients eligible for inclusion into the study, but 2 of them were disqualified because of the malignant neoplasm diagnosis shortly after material collection.
The Bioethics Committee at Wroclaw Medical University was permitted to perform this study (No. KB-221/2023 and KB-546/2012). All persons from Groups 1–8 were consecutively included in this study between 2013 and 2020.
Blood samples were collected during routine blood evaluations without additional venous punctures. Additional tubes were added to the standard number of tubes. Samples with a volume of 2.7 mL were required. Nurses performed the venous punctures in the morning. The patients were not required to fast that morning. After collection, the researchers waited for 10 min to ensure that the centrifugation of all the samples started at the same time after the venous puncture. After that, the blood was centrifuged at 1500 g. This process took 10 min. The material was collected only when the temperature in the laboratory and hospital was between 20°C and 28°C. The obtained serum was frozen at −80°C.
CellTrend GmbH, Luckenwalde, Germany, performed the analysis of the serum levels of autoantibodies against the AT2R. The levels of AT2R-Abs were measured using a commercially available sandwich enzyme-linked immunosorbent assay (ELISA) kit. Microtiter plates made from polystyrene were used. Every plate had 96 wells. These plates were precoated with receptors in the form of full-length proteins. To every buffer, 1 mM calcium chloride was added to maintain the conformational epitopes of the receptors. The samples were diluted (1:100) and incubated for 2 h at 4°C. All the samples were duplicated. Next, sample washing was performed. After that, the plates were incubated for 1 h using a 1:20,000 dilution of horseradish-peroxidase labeled goat anti-human IgG for detection. Next, 3,3′,5,5′-tetramethylbenzidine was used to present the results as a color spectrophotogram. Measurements were performed at a 450 nm wavelength with a correction at 630 nm. The standard curve was obtained through incubation of the plates with the test serum from a patient who was AT2R autoantibody-positive. Antibody assays were validated. No significant cross-reaction was found with other lupus antibodies. The validation of ELISA evaluations was performed according to the Bioanalytical Method Validation from the Food and Drug Administration Guidance for Industry.
Clinical data from the patients were collected. This data included basic serum creatinine, albumin, total protein levels, proteinuria, and age.
Serum concentrations of creatinine, total protein, albumin, and proteinuria were checked after 1 month, 3 months, 6 months, 12 months, and 2 years after the basic sample collection in prospective observation.
The levels of AT2R antibodies and clinical data (serum creatinine, albumin, total protein, proteinuria, and age) were compared in specific glomerulopathy patient groups and the control group using Dunn’s test with Bonferroni correction and analysis of variance (ANOVA).
A correlation analysis of quantitative variables was performed. Data distribution was checked using the Shapiro– Wilk test. Depending on the kind of distribution in the specimens—normal or non-normal—adequate rank correlation coefficients (Pearson’s or Spearman’s) were used. The significance of the correlations was checked using a t-test. The results of the analyses were positive when the p-value was <0.05. Correlations between AT2R antibody levels and clinical data (serum creatinine, albumin, total protein, proteinuria, and age) were checked. An evaluation was also performed for correlations between levels of antinuclear antibodies (ANAs) in patients with systemic lupus erythematosus, c-ANCA antibodies in granulomatosis with polyangiitis patients, p-ANCA antibodies in the group of patients with vasculitis, and AT2R antibody levels.
What followed was an analysis of the variability of clinical factors (creatinine level, albumin level, total protein level, and proteinuria) for 2 years of observation depending on basic AT2R antibody levels using:
- -
trend evaluation: Spearman’s correlation between AT2Rs and time (months);
- -
statistical range evaluation using Spearman’s correlation;
- -
standard deviation evaluation using Spearman’s correlation; and
- -
coefficient of variation evaluation using Spearman’s correlation.
Clinical parameter means for the patient groups with specific glomerular diseases were compared using Tukey’s test. Correlations between AT1R and AT2R antibodies were calculated for all groups.
The levels of AT2R antibody and clinical data (serum creatinine, albumin, total protein, proteinuria, and age) were compared between the specific groups. The analysis revealed higher AT2R antibody levels in the lupus nephritis group compared to the control group and the groups of patients with other types of glomerulonephritis. The mean and median values of AT2R antibodies in specific groups are presented in Table 1.
Median and mean AT2R antibody
| Median AT2R antibody levels (U/mL) | Mean AT2R antibody levels (U/mL) | |
|---|---|---|
| Systemic lupus erythematosus (Group 3) | 80.8 (range: 6.3–84.2) | 64.12 ± 26.95 |
| p-ANCA vasculitis (Group 8) | 8.55 (range: 3.3–57.6) | 12.28 ± 13.48 |
| c-ANCA vasculitis (Group 7) | 5.7 (range: 1.8–56.3) | 7.83 ± 8.70 |
| Mesangial proliferative (non-IgA) glomerulonephritis (Group 5) | 5.6 (range: 1.7–60.6) | 13.95 ± 22.93 |
| IgA nephropathy (Group 4) | 4.65 (range: 2–17.9) | 6.26 ± 4.39 |
| Membranous glomerulonephritis (Group 1) | 4.55 (range: 1.1–11) | 5.05 ± 2.95 |
| Focal segmental glomerulosclerosis (Group 2) | 4.5 (range: 1.3–16.4) | 5.71 ± 4.28 |
| Control group (Group 6) | 5.9 (range: 2.7–45.5) | 9.72 ± 11.88 |
Groups are ordered according to median AT2R antibody levels from highest to lowest apart control group.
±Standard deviation.
AT2R, angiotensin II type 2 receptor; c-ANCA, antineutrophil cytoplasmic antibodies.
The results of the AT2R antibody evaluations in the specific patients (represented as dots) are represented in Figure 1.
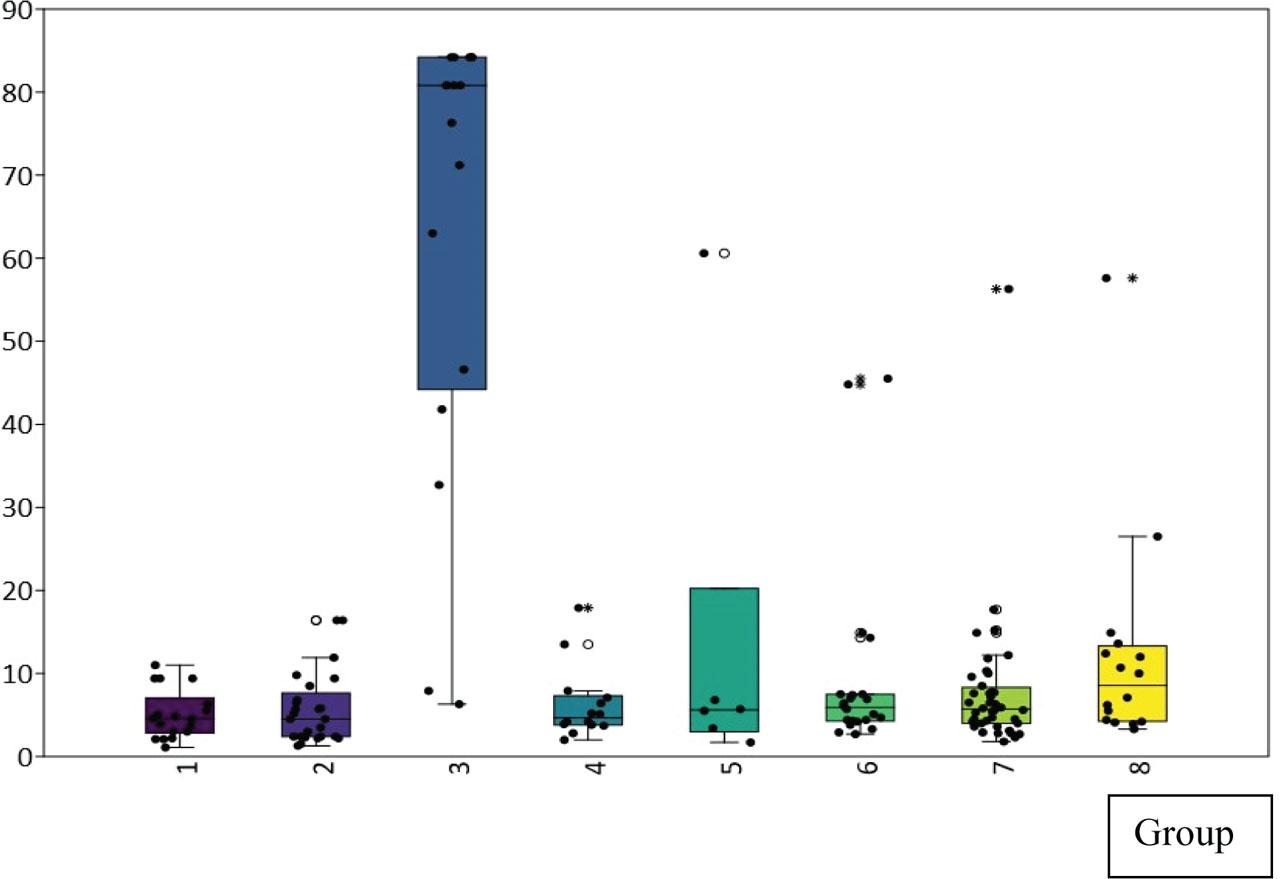
AT2R antibody values in specific groups of patients, axis y: AT2R antibody concentration (U/mL), axis x: particular groups of patients: 1 – membranous nephropathy, 2 – focal and segmental glomerulosclerosis, 3 – lupus nephritis, 4 – IgA nephropathy, 5 – mesangialproliferative (non-IgA) glomerulonephritis, 6 – control group, 7 – c-ANCA vasculitis, and 8 – p-ANCA vasculitis. AT2R, angiotensin II type 2 receptor; c-ANCA, antineutrophil cytoplasmic antibodies.
The comparison between the means of specific clinical parameters in the assessed patient groups is presented in Table 2.
Mean values of specific clinical parameters in the assessed patient groups
| Creatinine (mg/dL) | Proteinuria (g/24 h) | Total protein (g/dL) | Total albumin (g/dL) | Age (years) | |
|---|---|---|---|---|---|
| Membranous glomerulonephritis | 1.37 ± 0.57 | 4.23 ± 4.58 | 4.81 ± 0.70 | 2.79 ± 0.64 | 52.00 ± 12.00 |
| Focal segmental glomerulosclerosis | 1.32 ± 0.53 | 3.17 ± 3.11 | 5.20 ± 1.16 | 2.99 ± 0.91 | 46.36 ± 15.00 |
| Systemic lupus erythematosus | 1.21 ± 0.42 | 1.85 ± 1.70 | 5.60 ± 0.84 | 3.18 ± 0.59 | 37.82 ± 13.00 |
| IgA nephropathy | 1.19 ± 0.34 | 1.44 ± 1.29 | 5.57 ± 0.77 | 3.32 ± 0.64 | 43.86 ± 15.00 |
| Mesangial proliferative glomerulonephritis without IgA deposits | 1.01 ± 0.36 | 3.16 ± 2.54 | 4.68 ± 0.51 | 2.54 ± 0.61 | 31.50 ± 13.00 |
| c-ANCA vasculitis | 2.07 ± 1.54 | 1.72 ± 3.61 | 6.29 ± 0.44 | 3.63 ± 0.46 | 55.00 ± 18.00 |
| p-ANCA vasculitis | 3.93 ± 2.39 | 2.46 ± 3.08 | 6.09 ± 0.85 | 3.53 ± 0.42 | 62.00 ± 12.00 |
| Control group | 1.1 ± 0.25 | 0.00 ± 0.00 | 7.45 ± 0.85 | 4.40 ± 0.90 | 46.00 ± 13.00 |
±Standard deviation.
c-ANCA, antineutrophil cytoplasmic antibodies.
No significant correlations were found between AT2R antibody levels and clinical data (serum creatinine, albumin, total protein, proteinuria, and age). AT2R antibody levels did not correlate with ANA levels in patients with systemic lupus erythematosus, c-ANCA antibody levels in patients with granulomatosis with polyangiitis, or p-ANCA antibody levels in the group of patients with vasculitis. There was no correlation between AT2R antibody values and blood pressure. The groups were not statistically different in terms of mean blood pressure values.
There was no significant association between AT2R antibody levels and CH`50 (total complement activity) in the lupus nephritis group.
Trend evaluations, statistical range evaluations, standard deviation evaluations, and coefficient of variation evaluations did not reveal significant associations between basic AT2R antibody levels and clinical parameters (serum creatinine, albumin, total protein concentrations, and proteinuria) over time in prospective observations.
Correlations between AT1R and AT2R antibodies in specific glomerular diseases were also checked. The authors have data for AT1R antibodies from their previous study (Szymczak et al. 2022). Samples for both studies were collected from the same patients at the same time. It was found that these antibodies were positively correlated in the groups of patients with membranous nephropathy r = 0.66 (p = 0.003), IgA nephropathy r = 0.61 (p = 0.02), and c-ANCA vasculitis r = 0.63 (p = 0.00001). This data are presented in Figures 2–4.
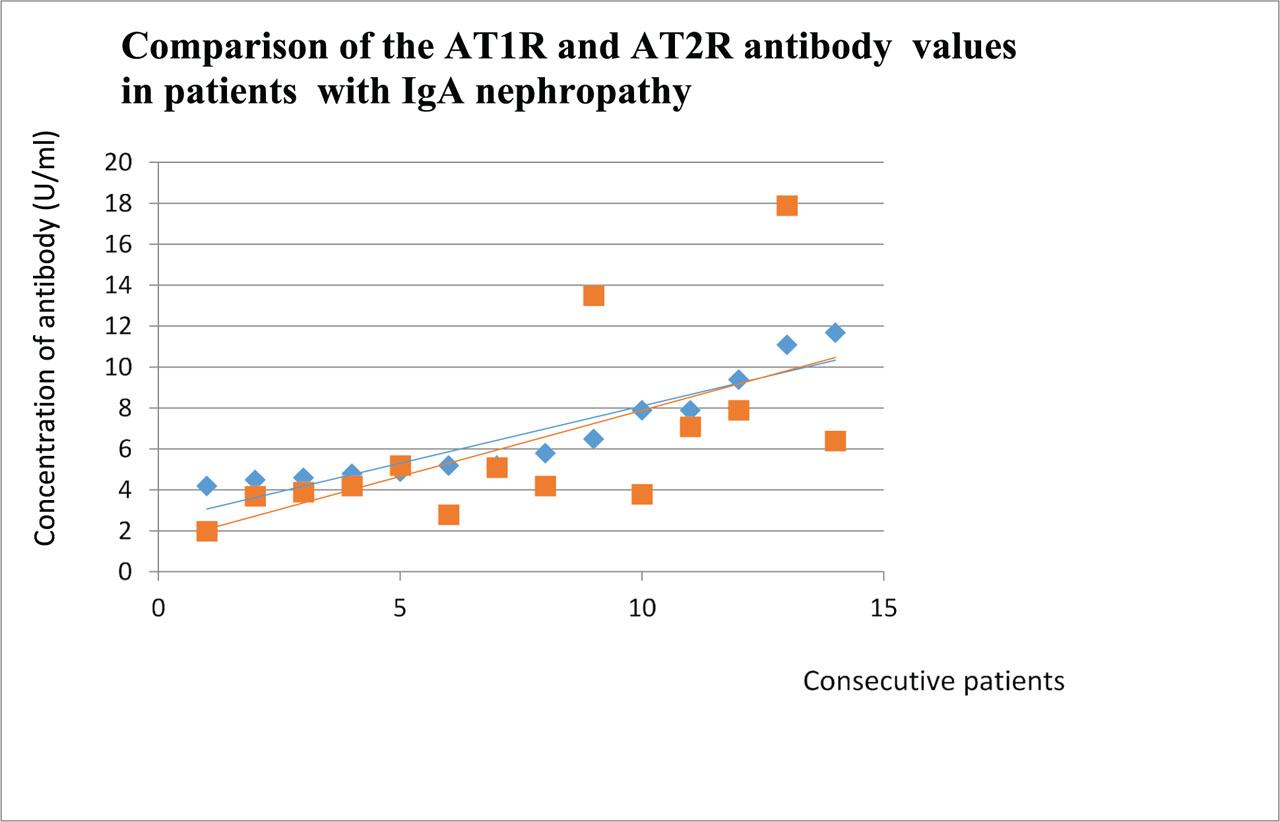
Comparison of the AT1R and AT2R antibody values in patients with IgA nephropathy. Patients are segregated according to the growing level of AT1R antibody. Blue dots represent values of AT1R antibody and red dots represent values of AT2R antibody. Blue line – trend line for the AT1R antibody and red line – trend line for the AT2R antibody. AT1R, angiotensin II type 1 receptor; AT2R, angiotensin II type 2 receptor.
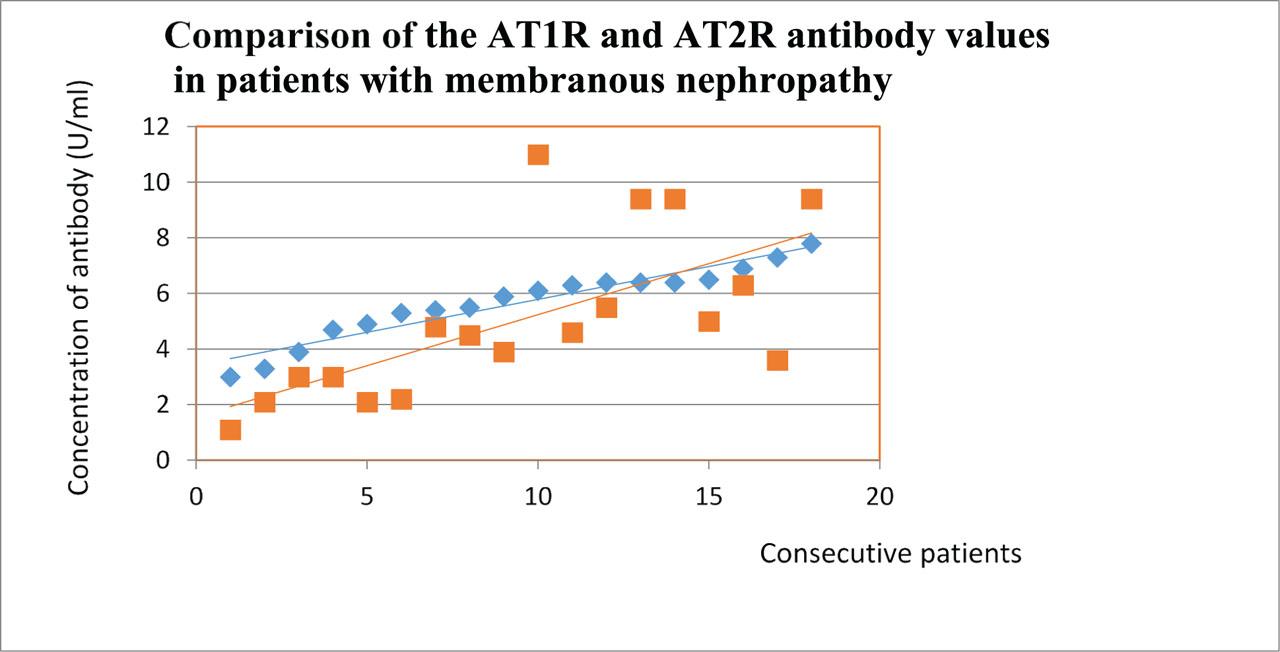
Comparison of the AT1R and AT2R antibody values in patients with membranous nephropathy. Patients are segregated according to the growing level of AT1R antibody. Blue dots represent values of AT1R antibody and red dots represent values of AT2R antibody. Blue line –trend line for the AT1R antibody and red line – trend line for the AT2R antibody. AT1R, angiotensin II type 1 receptor; AT2R, angiotensin II type 2 receptor.
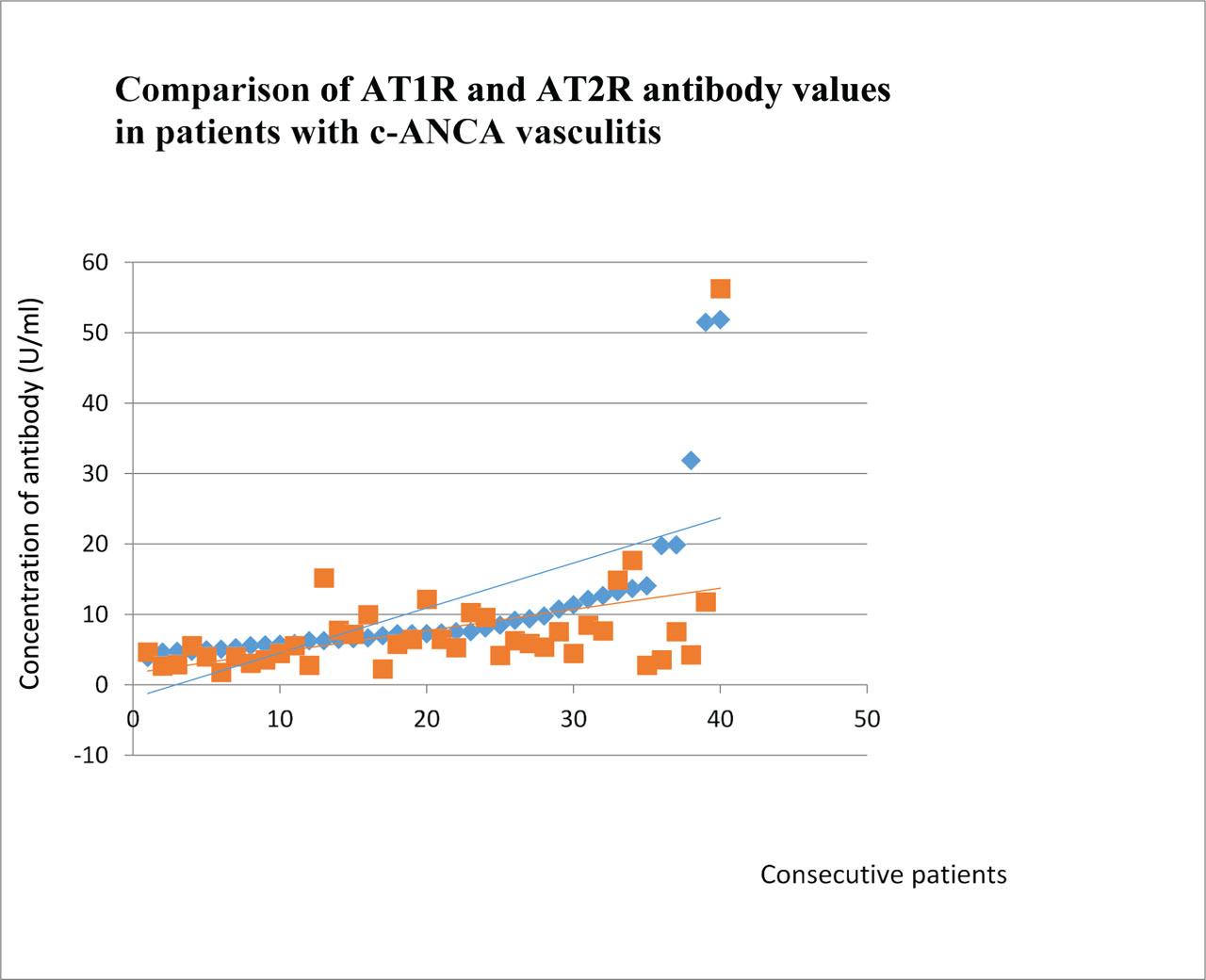
Comparison of the AT1R and AT2R antibody values in patients with c-ANCA vasculitis. Patients are segregated according to the growing level of AT1R antibody. Blue dots represent values of AT1R antibody and red dots represent values of AT2R antibody. Blue line –trend line for the AT1R antibody and red line – trend line for the AT2R antibody. AT1R, angiotensin II type 1 receptor; AT2R, angiotensin II type 2 receptor; c-ANCA, antineutrophil cytoplasmic antibodies.
The presented study revealed that AT2R antibody levels are higher in lupus nephritis than in other glomerulonephritis and the healthy control group. The results of AT2R antibody levels in the healthy control group were very similar to the levels of AT2R antibodies in the control group of a study about auto-antibodies in heart failure (Zweck et al. 2023). In that study, similarly to the study presented in this paper, AT2R antibodies were detected in healthy individuals (in low concentrations). This group used the tests from the same manufacturer for AT2R antibodies as our group. Taking into account the anti-inflammatory properties of AT2R activation (Okada et al. 2006), the authors hypothesized that higher levels of AT2R antibody would appear in immunologically active diseases such as lupus and systemic vasculitis, c-ANCA, and p-ANCA. This study confirmed higher AT2R antibody levels in patients with lupus nephritis, but patients with systemic vasculitis had low levels of AT2R antibodies. Systemic lupus erythematosus is a systemic disease (Koffler et al. 1967). Lupus nephritis usually occurs in active cases of systemic lupus erythematosus, so kidney involvement is also a sign of the systemic activity of lupus (Lech and Anders 2013). This study evaluated AT2R antibodies in the serum, and their high activity reveals their systemic effect. It was found that AT2R autoantibodies produced in immunized rabbits activate AT2R. This activation impairs AT1R-mediated vasoconstriction (Liles et al. 2015). This observation may suggest the production of AT2R antibodies as a control mechanism for vasoconstriction. However, there was no correlation between AT2R antibodies and blood pressure in our study (the same applies to lupus patients and other groups of patients). Our study shows that AT2R antibodies have some connection with the lupus nephritis diagnosis, but it does not prove their influence on lupus pathogenesis, course of disease, or prognosis. There was no connection between AT2R antibody levels and the clinical course of the disease.
To reveal the real influence of these antibodies on the course of lupus nephritis, AT2R antibody levels should be analyzed at many points in time in larger groups of patients. Progressive analyses evaluating the influence of markers on disease courses are biased by the treatment of the patients. There is no possibility of not treating patients for some years without having a negative influence on the course of the disease. Patients receiving comparable treatment in the progressive observation period still did not exclude the influence of treatment on the results. Standard treatment for membranous glomerulonephritis, focal and segmental glomerulosclerosis, and mesangial proliferative glomerulonephritis without IgA deposits was three boluses of 500 mg of methylpredniso-lone, followed by diminishing doses of prednisone starting at 1 mg/kg of body weight. IgA nephropathy patients received three bolus doses of 500 mg of methylprednisolone every 2 months (three times) and prednisone 0.5 mg/kg of body weight every other day for 6 months. Patients with lupus nephritis and vasculitis received six doses of 500 mg of cyclophosphamide every 2 weeks, followed by diminishing doses of prednisone starting at 1 mg/kg of body weight and azathioprine at 100 mg/day. Every patient may have a different genetic susceptibility to drugs, every disease may be better or less treatable with drugs, and every drug may influence biomarker levels and disease markers during prospective observations. Multifactorial analyses conducted in large trials should help to solve these problems.
Many antibodies appeared in the course of glomerulopathies, especially in lupus nephritis and membranous nephropathy. Their significance is still unknown, but they seem to be involved in the regulation of pathogenic processes. Sometimes, the combined analysis of these markers seems to be more efficient and facilitates the differentiation of patients with a worse prognosis. An analysis of anti-PLA2R antibodies, anti-enolase antibodies, and anti-superoxide dismutase antibodies revealed a worse prognosis in patients with membranous nephropathy with positive results from these evaluations. Moreover, positive results of the assessment of all three antibodies worsened clinical outcomes (Ghiggeri et al. 2020).
Lupus nephritis is connected with the appearance of many autoantibodies: ANA, anti-double-stranded deoxyribonucleic acid (DNA), anti-collagen IV, anti-collagen III, anti-laminin, anti-annexin II, anti-alfa-actinin, anti-heparan sulfate proteoglycans, anti-C1q, anti-ribosomal P, and anti-cardiolipin antibodies. Additionally, numerous autoantibodies against antigens derived from podocytes, glomerular mesangial cells, vascular capillary walls, and the proximal tubules can appear in lupus nephritis (Tsai et al. 2023). Lupus is indeed a very active disease, involving many potential targets for autoantibodies. Some of these antigens are connected with scaffolding function, and some of them are very active receptors essential for the function of the body. Angiotensin II receptors are known for their extensive influence on many factors. A detailed study of these receptor connections is very important.
AT2R antibodies diminish the vasoconstrictive reaction on angiotensin II during AT1R stimulation, AT2R stimulation, causing a vasodilation effect, so these antibodies are stimulatory. There was a lack of difference in blood pressure between animals with high AT2R antibodies and control animals in the original study that found these antibodies for the first time (Liles et al. 2015). Our observations indicate a lack of correlation between AT2R antibody levels and blood pressure. These observations together suggest the stimulatory and regulatory characteristics of these antibodies. They may reveal their influence as a kind of reaction to angiotensin II activity. Unfortunately, we have no data about aldosterone levels. Previous observations concerning high levels of the AT2R antibodies in primary aldosteronism (Liles et al. 2015) suggest a potential role of aldosterone in the regulation of these processes.
In their previous article about AT2R antibodies, the present authors found that AT1R antibodies were higher in lupus nephritis and vasculitis than in other forms of glomerulonephritis. Furthermore, the study found that AT1R antibodies were connected with the course of membranous nephropathy and p-ANCA vasculitis (Szymczak et al. 2022).
Material for that study was derived from the same cohort of patients, so the authors were able to analyze correlations between AT1R and AT2R antibodies. We found that these antibodies were positively correlated in the groups of patients with membranous nephropathy (r = 0.66), IgA nephropathy (r = 0.61), and c-ANCA vasculitis (r = 0.63). All these correlations were statistically significant (p < 0.05). Such correlations were possible to predict because AT1R and AT2R have opposite functions and can regulate each other (Suzuki et al. 2007). Such observations strengthened our previous conclusions about the significance of AT1R antibodies in membranous nephropathy (Szymczak et al. 2022), but for other diseases, the view is unclear.
AT1R and AT2R antibodies are correlated, so it is possible that both these antibodies influence each other, especially in pathologic conditions.
AT1R and AT2R act oppositely and regulate each other, creating equilibrium (Colin et al. 2023). The situation when AT1R antibodies correlate with AT2R antibodies may create a milieu of double equilibrium.
Real activation of the AT2R may be the result of all four factors interacting (AT1R, AT2R, AT1R antibodies, and AT2R antibodies). This is only a hypothesis that should be proved on molecular models.
Some observations indicate the influence of AT1R autoanti-bodies on AT2R expression, suggesting a relationship. This influence is connected with two axes and many concomitant factors (Sun et al. 2020).
Our observation (a positive correlation between AT1R antibodies and AT2R antibodies in some diseases and a lack of this correlation in other diseases) suggests the influence of the diseases on the functioning of this network of associations. This hypothesis should also be proved in molecular models and in larger groups of patients.
Nevertheless, this study is the first to assess AT2R antibody levels in lupus nephritis, in particular kinds of glomerulonephritis and a control group, and to assess this antibody’s significance in prospective observation. We proved that lupus nephritis levels were the highest in these groups.
Levels of AT2R antibody in systemic lupus erythematosus are higher compared to other types of glomerulonephritis, vasculitis, and a healthy control group. Levels of AT2R antibodies correlate with AT1R antibodies in the groups of patients with membranous nephropathy, IgA nephropathy, and c-ANCA vasculitis. These kinds of AT2R antibodies have a stimulative effect on AT2R, but we have not found the influence of these antibodies on the clinical course of glomerular diseases.