
Today, invasive procedures that spare the lives of many patients with life-threatening diseases are a common part of treatment options.1 Bone marrow aspiration (BMA) is one of the procedures commonly used for both diagnoses and treatments. BMA is the main method for detection of solid tumors, and has a pivotal role in the diagnosis of many hematological disorders.2 Developed in the early 19th century, the procedure made it possible for doctors to diagnose various marrow disorders for the first time.3 BMA has become increasingly utilized not only for diagnostic purposes but also in the realm of regenerative medicine.4
While BMA offers valuable clinical insights and therapeutic applications, it is inherently associated with patient discomfort, including both pain and psychological stress. Several studies have revealed that patients undergoing BMA frequently experience symptoms such as fatigue, pain, and anxiety.5 For this reason, BMA is known as a painful procedure involving the insertion of a needle into the bone and inducing stress and pain.6 Many studies have made great strides in offering viable approaches to mitigate pain and reduce stress.7 Treatment modalities include both pharmaceutical and non-pharmaceutical interventions.8 The most commonly used pharmacological approach uses anesthetic drugs to reduce the medical procedure-related anxiety and pain. Pharmacologic treatment approaches have many complications, including drowsiness, respiratory depression, prolongation of hospitalization, and high medical costs.
Recent literature on managing BMA-related distress highlights various non-pharmacological methods, from distraction-based techniques like music therapy to physiological interventions like deep breathing. While distraction can be effective, interventions such as the deep breathing technique (DBT) are of particular interest as they may directly target the autonomic nervous system to induce a state of relaxation.9 Furthermore, DBT is highly practical, being simple for patients to learn without extensive time or equipment.10 Despite these theoretical benefits, the specific efficacy of DBT in the high-stress, acute-pain context of BMA remains underinvestigated, representing a key gap that the present study aims to address.
Therefore, the present study aimed to investigate the effects of DBT on procedural pain and anxiety in a population of Iranian patients with knee and ankle osteoarthritis or avascular necrosis (AVN) undergoing BMA for cell therapy.
This study employed a parallel randomized clinical trial design to investigate the impact of a DBT intervention on pain, anxiety, and physiological parameters in patients undergoing BMA. Ethical considerations were prioritized, with written informed consent obtained from all 60 adults between the age range of 35 and 60. Subjects were randomly allocated to either an intervention group or a control group using random number tables to ensure unbiased group assignment.
The sample size of the study was determined by Power Analysis. On the basis of the previous research11 conducted with a large effect size (0.80) to achieve a power of 0.80%, confidence interval 95%, and α = 0.05, the total sample size was estimated to be 60 subjects (each group required 30 subjects). To determine the sample size, we used G-Power software version 3.1.9.2 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany).
The study population consists of 35 to 60-year-old subjects with osteoarthritis knee, hip, and AVN. The subjects underwent BMA for stem cell therapy. The patients were American Society of Anesthesiologists (ASA) physical status I and II, able to read and write. Exclusion criteria were Patients with skin diseases at or around the BMA site, scars, psoriasis, active dermatitis or eczema, infection, sedative or alcohol abuse, chronic consumption of analgesics, history of peripheral neuropathy, difficulty in communication, chronic pain, prior experience of BMA, and Chronic respiratory problems. A total of 98 patients were evaluated for eligibility, and 38 subjects were excluded from the study because 30 patients weren’t able to read and write, 3 were affected with respiratory problems, 3 were addicted, and 2 had chronic pain. Finally, 60 patients were selected and divided into 2 study groups (Figure 1).
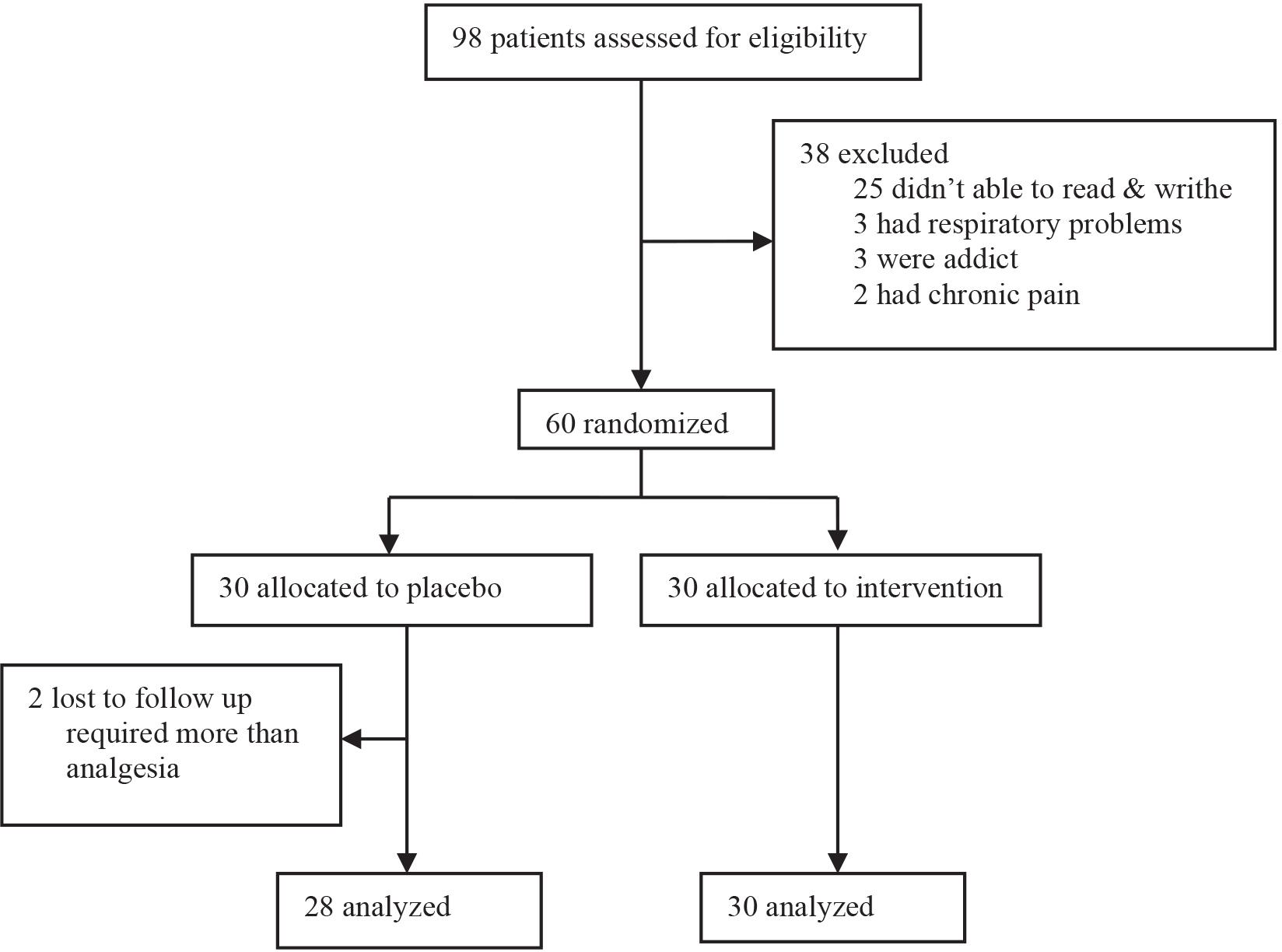
The PRISMA diagram describing the selection of included literature. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyzes.
The study was approved by Review Board of researcher’s institution (IRB; NE.REC.1394.550) and performed in compliance with the Helsinki protocol. The target patients were oriented about the methods of this survey. They are allowed to quit the study at any phase if they tend to. The confidentiality of all the relevant documents of the participants was guaranteed.
The measures used in this study, including the Spielberger State Anxiety Inventory (SAI)12 were recruited for the measurement of anxiety in adults. The inventory assesses the present feeling of the respondents.13 The validity and reliability of the study for the Iranian version of the SAI were conducted by Mahram in 1998.14 The Cronbach alpha value was calculated to be 0.945. The SAI is composed of 20 items asking individuals to explain their feelings of calmness or anxiety at that time. It is categorized into a 4-point intensity scale ranging from not at all (1) to very much (4). The SAI sum score is between 20 and 80 and is composed of 20 items. The anxiety level between 20and 39 shows the mild, 40–59 indicates moderate, 60–80 points out severe anxiety, and >60 denotes that the patients need professional help.13 The SAI was filled in by the patients who were in the waiting room adjacent to the operating room prior to and after DBT, about 30 min before admission to the operating room. Pain intensity was assessed using the visual analog scale (VAS), a validated tool for subjective pain measurement, with scores ranging from 0 (no pain) to 10 (worst imaginable pain). VAS scores were recorded immediately following the completion of the BMA procedure. Furthermore, physiological parameters were monitored using pulse oximetry, which provided measurements of systolic blood pressure and diastolic blood pressure (SBP, DBP), heart rate (HR), and oxygen saturation (O2sat).
Prior to admission to the operating room, patients of target groups were directed to 2 separate waiting rooms with the temperature of 23 ± 1°C with minimal distraction.
Both groups are requested to fill in the SAI, and vital signs were recorded (including: SBP, DBP, HR, O2Sat). Afterward, the intervention group was trained about DBT so that they could keep their mouth closed and inhale deeply through the nose by moving their stomach muscle to inhale, and then exhale through Pursed lip breathing. They had to regulate inhale and exhale so that the latter can roughly take twice as long as the former. All the processes were supervised by an expert nurse. The control group was not required to take the training program. After 30 min, both groups of patients were requested to refill the SAI, and their vital signs were checked once again. Later on, the patients were transferred to the operating room and were placed in the lateral position for BMA. All patients underwent BMA from the left iliac crest using a Jamshidi biopsy needle (BD, Franklin Lakes, NJ, USA). Localized anesthesia was done for all patients using 10cc lidocaine 2%. The case group patients were asked to do DBT before using the Jamshidi biopsy needle. The control group was not subject to these instructions. The patients were asked to report the pain intensity just after BMA, and the pain was assessed by using a visual analog scale (VAS). Furthermore, VS were measured before and after BMA. Throughout the process, right hand of the patients was used for measurement of blood pressure (BP), and the left hand was used for measurement of O2Sat and HR. To reduce operational bias and control confounding factors, all these steps were performed by an oncologist and a trained professional nurse (Figure 2).
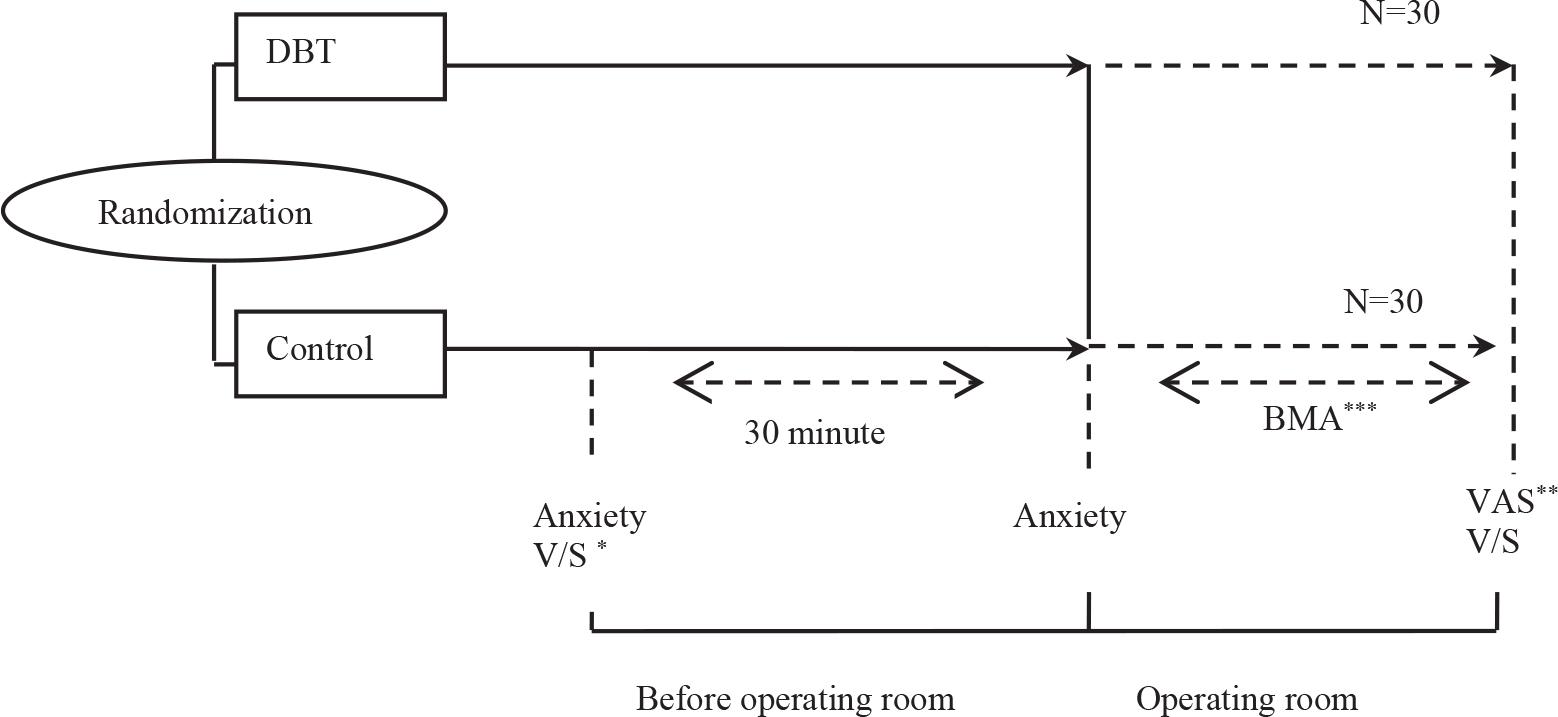
Study design of the intervention and control groups.
Note: Vital sign; **Visual analog scale; ***Bone marrow aspiration. DBT, deep breathing technique.
Statistical analysis was conducted using SPSS version 16 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was employed to assess the normality of data distribution. Baseline data across study groups were compared using t-tests and chi-square tests, as appropriate. Analysis of covariance (ANCOVA) was utilized to compare post-intervention anxiety scores between the groups, using the baseline (pre-intervention) anxiety score as a covariate to control for any initial differences. Between-group comparisons of Visual Analog Scale (VAS) scores were performed using t-tests. Paired t-tests were employed to evaluate the effect of DBT on SBP, DBP, O2sat, and HR before and after the intervention. All variables represent mean ± standard deviation (SD) (for ANCOVA, data represent mean ± standard error). A significant level was set at 0.05 for all tests.
Following random assignment to intervention and control groups, 2 participants in the control group were excluded due to the requirement of analgesia during BMA. The final sample comprised 28 participants in the control group and 30 in the intervention group, yielding a participant retention rate of 96.6%. No adverse effects were observed during the study. Complete data sets were obtained for all measures, ensuring no missing values. All quantitative variables exhibited a normal distribution. The mean age of the participants was 50.63 years (SD = 9.8), with a female-to-male ratio of approximately 2:1 (70.7% female, 29.3% male). Table 1 presents the demographic and baseline characteristics of the sample. Independent samples t-tests revealed no statistically significant differences between the intervention and control groups at baseline (P > 0.05).
Demographic details of the study population, n (%).
| Parameter/group | Breathing group (n = 30) | Control group (n = 28) | P |
|---|---|---|---|
| Age (years) | 51.8 ± 8.6 | 49.3 ± 10.8 | 0.353 |
| Female | 23 (56.1) | 18 (43.9) | 0.301 |
| Margie, yes | 27 (52.9) | 24 (47.1) | 0.857 |
| Weight, kg (M ± SD) | 74.2 ± 10.9 | 77.1 ± 9.8 | 3.359 |
| ASA class | 0.512 | ||
| I (%) | 18 (60) | 19 (67.9) | |
| II (%) | 12 (40) | 9 (32.1) | |
| Diagnosis | 0.504 | ||
| Osteoarthritis knee | 25 (83.3) | 21 (75) | |
| Osteoarthritis hip | 5 (16.7) | 6 (21.4) | |
| AVN | 0 | 1 (3.6) |
Note: Data are mean ± SD or number (%); Use t student and Chi-square test to comparison between studies group; Significance level was 0.05; AVN, avascular necrosis; SD, standard deviation.
A comparative analysis of anxiety levels between the 2 groups revealed a statistically significant difference in mean anxiety scores. The intervention group exhibited a significantly lower mean anxiety score compared to the control group (P = 0.018). Similarly, mean VAS scores were significantly lower in the intervention group than in the control group (P < 0.001). (Table 2).
Comparison anxiety and pain between study groups.
| Variable | Intervention | Placebo | Mean difference | P |
|---|---|---|---|---|
| Anxiety | 19.81 ± 0.75 | 22.45 ± 0.77 | −2.64 ± 1.08 | 0.018 |
| VAS | 1.30 ± 1.51 | 3.4 ± 2.04 | −2.34 ± 0.46 | <0.001 |
Note: Data for anxiety variable represented mean ± standard error and for VAS represented mean ± SD. Mean difference is (Intervention - Placebo). Significance level was 0.05; SD, standard deviation; VAS, Visual Analog Scale.
Analysis of vital signs before and after the intervention revealed significant decreases in both SBP (P < 0.001) and DBP (P < 0.001) within the intervention group. The effect of DBT on SBP reduction was more pronounced than its effect on DBP. Conversely, no significant changes in SBP or DBP were observed in the control group. Furthermore, the intervention group exhibited significant decreases in HR (P < 0.001) and O2sat (P = 0.044) following DBT. No significant changes in HR or O2sat were detected in the control group. (Table 3).
Comparison variables before and after intervention in different study groups.
| Groups and variable | Before | After | Mean difference | P |
|---|---|---|---|---|
| Intervention | ||||
| SBP | 132.2 ± 22.2 | 114.3 ± 19.4 | 17.8 ± 14.02 | <0.001 |
| DBP | 85.4 ± 13.9 | 73.2 ± 11.9 | 12.17 ± 10.5 | <0.001 |
| HR | 80.6 ± 12.5 | 68.5 ± 7.9 | 12.03 ± 8.98 | <0.001 |
| O2sat | 97.03 ± 1.15 | 96.17 ± 1.78 | 0.867 ± 2.25 | 0.044 |
| Control | ||||
| SBP | 126.2 ± 17.01 | 116.3 ± 26.5 | 9.96 ± 26.16 | 0.064 |
| DBP | 81.7 ± 12.7 | 79.7 ± 11.5 | 1.96 ± 9.2 | 0.289 |
| HR | 78.7 ± 14.05 | 78.3 ± 13.1 | 0.462 ± 8.17 | 0.776 |
| O2sat | 96.92 ± 1.38 | 97.04 ± 1.31 | −0.115 ± 1.33 | 0.664 |
Note: Data represented as mean ± SD. Mean difference is (before - after); Used paired t test for comparison before and after intervention. Significant level was 0.05; DBP diastolic blood pressure; HR, heart rate; O2sat, oxygen saturation; SBP, systolic blood pressure; SD, standard deviation.
The experience of pain during medical procedures can cause significant stress, fear, and anxiety in patients.15 While the type of procedure can influence physical pain and anxiety levels, this discomfort is also affected by individual factors that may contribute to this discomfort, such as emotional status, cultural background, and previous unpleasant experiences of hospitalization and individual variability of pain threshold.16
In addition to Pharmaceutical methods, nonPharmaceutical methods could be used to reduce the pain and anxiety in patients who were subject to invasive procedures.17 The American Society for Pain Management Nursing (ASPMN) points out that surgery procedures inducing pain and anxiety should be controlled before and during procedures.18 For invasive procedures such as BMA, local or general anesthesia is highly recommended to manage or alleviate pain.2
Due to the potential complications of pharmacological approaches, non-pharmacological methods like distraction are widely applied. Several studies have been launched into the effect of non-pharmaceutical methods on the reduction of pain and anxiety in patients with similar results in most cases. These studies have shown that the use of non-Pharmaceutical methods can be helpful in reducing pain and anxiety.19–21
Non-pharmaceutical methods can affect the nervous system to induce relaxation. Therefore, these methods can lead to a reduction in both anxiety levels and the severity of perceived pain in patients.22 The present study showed that using DBT, one of the non-pharmaceutical methods for the reduction of pain and anxiety, in patients who are BMA candidates. The mean score of pain and anxiety in the intervention group was less than that of the control group.
Our finding that DBT significantly reduced anxiety aligns with the work of Martínez-González, which demonstrated similar effects in a general population of older adults. Our study critically extends these findings by confirming the efficacy of DBT in a younger, procedurally-stressed patient cohort. Furthermore, our research adds a new dimension by linking the subjective reduction in anxiety to objective physiological markers of relaxation (i.e., reduced HR and BP).23 This connection, supported by Basaranoglu et al.’s24 work on the Vagus nerve stimulation mechanism of DBT, suggests that the technique’s benefits are not merely psychological but are underpinned by measurable physiological responses. The function of DBT as a distraction technique further explains its effectiveness in reducing pain.
In the present study, it is observed that average O2Sat decreased in intervention group, whereas no change in the control group was detected. Although this achievement is similar to the study conducted by Ghasemi et al.,25 other studies showed an increase in O2 saturation after DBT. Normally, it is expected that when DBT is performed, O2 saturation increases or shows no change because DBT improves arterial oxygenation by increasing alveolar volume and gas exchange at the alveolar capillary membrane level.26 This decrease, while unexpected when compared to literature reporting an increase in O2 saturation, merits closer examination. The modest reduction (from 97.03% to 96.17%) remained well within safe clinical limits and could be attributable to transient physiological shifts from the prolonged exhalation technique or minor measurement variability. While this complex response warrants further investigation, it does not detract from the significant benefits of DBT observed for pain and anxiety.
Accordingly, our study showed a reduction in SBP and DBP in patients who performed DBT. However, no change was observed in HR, SBP, and DBP in the control group. DBT has known hemodynamic effects, including the prevention of increases in systemic blood pressure.27 Given this evidence, it is understood that DBT can also reduce elevated BP in hypertensive patients.
Another study that reveals DBT effect on the parasympathetic autonomic nervous system and subsequently stimulates the baroreceptors to cause BP and HR reduction.28 This study also focused on the anxiety of BMA candidates prior to their admission to the operating room. This study also evaluated the patients’ postprocedural pain experience. Pain and anxiety are side effects of the BMA. This study demonstrates that the DBT intervention significantly reduced anxiety scores compared to the control group. Furthermore, the intervention group experienced a significant reduction in pain severity compared to the control group. It is thought that it is important for candidate patients for invasive procedures with no need for general anesthesia, such as BMA, to adapt themselves to relaxation methods to relieve anxiety and pain.
In general, the patients refer to the hospital from different walks of life and various cultural, social, and academic backgrounds. For this reason, relaxation methods should be simple and easy for patients to adopt, such as the deep breathing method that patients can perform with ease anytime and anywhere.
The findings of this study, demonstrating that DBT significantly reduces both pain and anxiety, hold considerable practical implications. To translate these results into standard clinical practice, healthcare institutions should move beyond mere acknowledgment of the technique’s efficacy. A crucial next step involves developing standardized, brief training protocols for nursing staff to ensure consistent and effective patient instruction prior to procedures like BMA. Such protocols, complemented by patient-facing materials like illustrated leaflets, could be seamlessly integrated into pre-procedural checklists. These low-cost, high-impact measures can empower patients and substantially improve their procedural experience.
Despite the significant findings, this study has several limitations that must be acknowledged. First, the BMA procedures were performed by a single oncologist, which introduces a potential for operational bias. Although this ensures consistency in technique, involving multiple practitioners could have enhanced the generalizability of the findings. Second, while randomization was employed, patients’ psychological expectations were not formally assessed or controlled. The mere act of receiving a novel intervention could have created a placebo effect, contributing to the observed reductions in pain and anxiety. Future studies would benefit from including a placebo control group to isolate the specific effects of DBT.
Furthermore, the study was conducted at a single center in Iran, which may limit the cultural generalizability of the results, as pain perception and expression can be culturally influenced. Finally, the sample size, while statistically adequate for the primary outcomes, was relatively small. Larger, multi-center trials are needed to confirm these findings and explore the technique’s efficacy across diverse patient populations.
DBT was found to be the most effective method for the appeasement of pain and relief of anxiety in patients’ candidate BMA. Nurses require a comprehensive understanding of procedural anxiety and pain management in the context of BMA.