
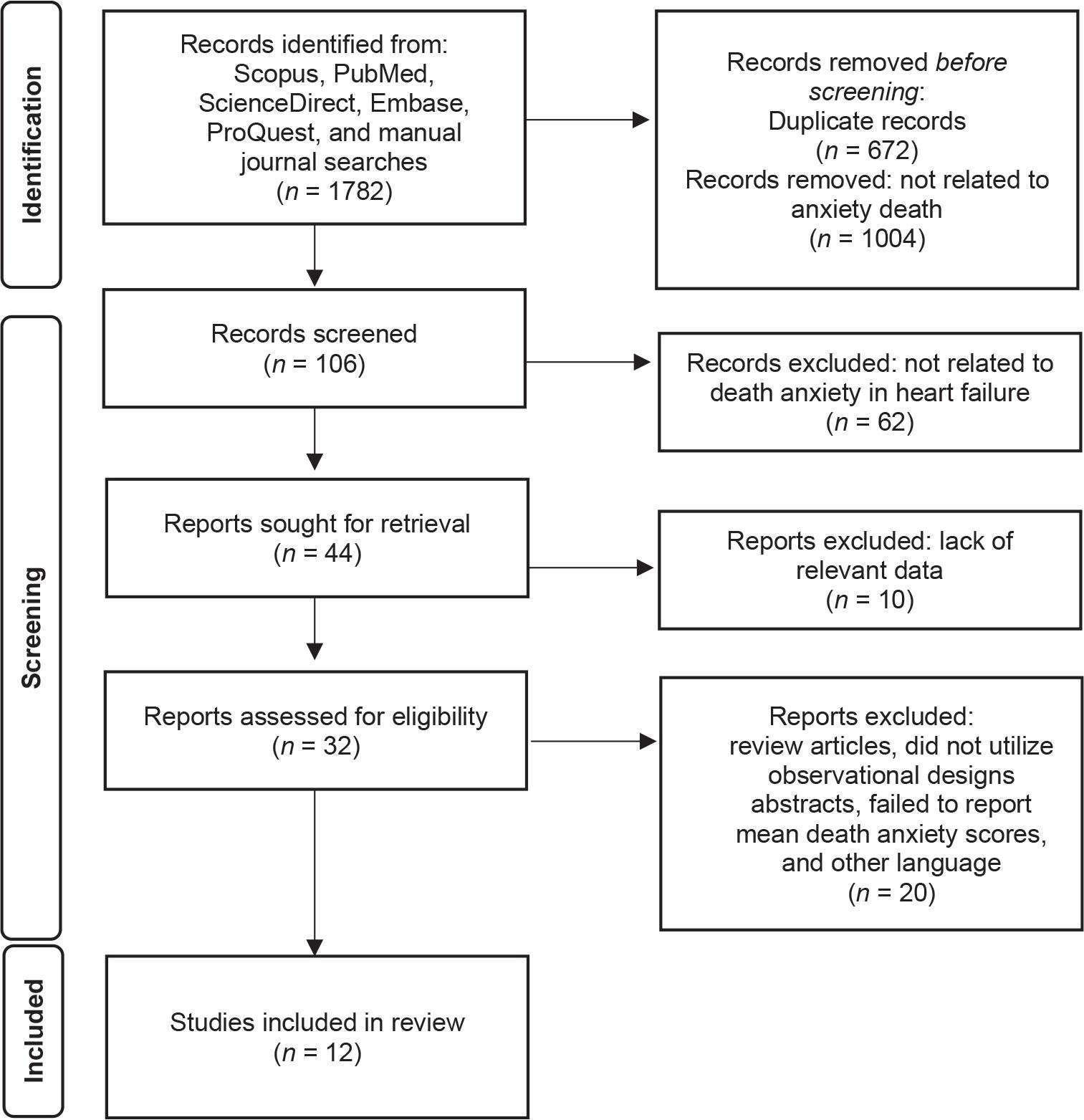
Figure 1.
Characteristics of included studies_
| Characteristics of studies | Number of studies (n) | Percentage (%) |
|---|---|---|
| Country | ||
| Iran | 7 | 58.33 |
| Turkey | 4 | 33.34 |
| USA | 1 | 8.33 |
| Design | ||
| Cross-sectional | 9 | 75.10 |
| Mixed-method longitudinal | 1 | 8.33 |
| Quasi-experimental | 1 | 8.33 |
| Randomized controlled trial | 1 | 8.33 |
| Sample size | ||
| <100 | 2 | 16.67 |
| 101-150 | 5 | 41.67 |
| 150-200 | 1 | 8.33 |
| >200 | 4 | 33.33 |
Summary of included studies on death anxiety in HF_
| Authors (years) | Purpose | DAS | Score range | Mean death anxiety (SD) | Severity interpretation | Main findings |
|---|---|---|---|---|---|---|
| Asgari et al. (2018)6 | To examine death anxiety and its relationship with demographics in patients with HF | Templer DAS (15-item) | 15–75 | 47.95 ± 6.91 | Moderate–high | Over 90% of patients experienced moderate to severe death anxiety |
| Çamcı et al. (2024)7 | To explore the relationship between religious coping and death anxiety in HF | Templer DAS (15-item) | 0–15 | 7.78 ± 3.91 | Moderate–high | Higher death anxiety associated with longer HF duration; weak positive correlation with religious coping |
| Ghorbani et al. (2023)12 | To compare spiritual experiences and death anxiety in HF vs angina patients | Templer DAS (15-item) | 15–75 | 43.15 ± 13.41 | Moderate–high | Significant negative correlation between spiritual experience and death anxiety |
| Merati et al. (2024)13 | To examine relationship between QoL and death anxiety in patients with HF | Templer DAS (15-item) | 15–75 | 7.54 ± 2.35 | Moderate–high | Higher death anxiety associated with poorer QoL (r = 0.329, P < 0.001) |
| Sacco et al. (2014)18 | To investigate psychosocial resources and well-being in HF | DAS/WHOQOL | 0–10 | 5.58 ± 2.62 | Moderate | Religious/spiritual support associated with lower death anxiety |
| Yildirim et al. (2024)17 | To explore associations between death anxiety, loneliness, and hope | Templer DAS (15-item) | 0–15 | 10.41 ± 3.94 | High | Death anxiety positively predicted by age and loneliness (R2 = 23.1%) |
| Sazak et al. (2025)15 | To examine spiritual orientation and frailty mediated by death anxiety | Templer DAS (15-item) | 0–15 | 8.03 ± 4.45 | Moderate–high | Death anxiety mediated the relationship between spiritual orientation and frailty |
| Soleimani et al. (2020)14 | To identify predictors of death anxiety among cardiac patients | Templer DAS (15-item) | 15–75 | 45.15 ± 8.44 | Moderate–high | Greater economic standing, reliance on friends as a primary income source, older age, stronger religious faith, and heightened hope were linked to reduced death anxiety. |
| Moradi et al. (2022)4 | To assess cognitive-behavioral therapy’s effect on death anxiety and depression in HF | Templer DAS (15-item) | 0–15 | 9.96 ± 1.69 | Moderate–high | Cognitive-behavioral therapy significantly reduced death anxiety in patients with HF (P < 0.001). |
| Aryafard et al. (2023)10 | To examine correlations of death anxiety with spirituality and resilience | Templer DAS (15-item) | 0–15 | 7.21 ± 2.22 | Moderate | Religious attitude and resilience inversely associated with death anxiety |
| Batı et al. (2024)16 | To explore self-care agency and death anxiety among elderly | Templer DAS (15-item) | 0–15 | 6.76 ± 3.25 | Moderate | Very weak positive correlation between self-care and death anxiety (r = 0.158, P = 0.004) |
| Babaei Vahed et al. (2022)11 | To evaluate illness perception training on death anxiety in HF | Templer DAS (15-item) | 0–15 | NR | Moderate | Training on illness perception significantly reduced anxiety about death, with a pre- to post-training change that was statistically significant (P < 0.001). |