
Heart failure (HF) is a progressive chronic illness associated with high mortality rates and frequent hospitalizations.1 In addition to the physical symptoms, patients with HF often grapple with psychological challenges, including anxiety and depression, which arise from the uncertainty regarding their prognosis and the confrontation with mortality.2 Death anxiety refers to an intense or overwhelming fear of death or dying, frequently accompanied by feelings of dread and existential angst.3 In the context of HF, patients are often acutely aware of their life-threatening condition, which can lead to increased levels of death anxiety.4 Qualitative evidence indicates that more than half of patients with advanced HF experience fear when facing their future and the possibility of death.5 This fear can exacerbate stress, reduce quality of life (QoL), and impede effective self-management of HF.
Emerging research has begun to quantify death anxiety in patients with HF using standardized scales. Early studies suggest death anxiety is prevalent in this population. For instance, a study revealed that over 90% of patients with HF reported moderate to severe anxiety related to death.6 Similarly, clinical observations link advanced HF with significant fears about dying,7 comparable to those seen in terminal cancer patients.8 Despite these indications, the literature on death anxiety in HF remains limited and scattered. No prior review has systematically synthesized findings on how severe death anxiety is among patients with HF and what factors may influence it. An integrative review can provide a consolidated understanding, guiding clinicians in addressing this psychosocial dimension of HF care and identifying gaps for future research.
To date, no integrative review has methodically synthesized quantitative evidence on the prevalence and correlates of death anxiety among patients with HF. The primary objective of this review is to synthesize and critically evaluate observational studies of average levels of death anxiety in this population. This review targets observational methodologies explicitly—including cross-sectional, cohort, and case-control designs—due to their efficacy in uncovering patterns, correlates, and population-level trends while minimizing intervention-related biases. By synthesizing observational evidence, the review facilitates a comprehensive understanding of the manifestation of death anxiety across diverse patient demographics and clinical environments. By concentrating on studies that quantitatively assessed death anxiety, the author aims to determine “What are the average death anxiety scores in HF patients” and “what contextual factors or correlates have been identified?” This understanding can enhance both clinical assessment practices and psychosocial interventions, ultimately improving the holistic care for patients with HF.
This integrative literature review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9
Eligible studies were defined based on the following inclusion criteria: patients with HF (of any stage or in any setting); observational designs (including crosssectional surveys, cohort studies, or case-control studies) reporting original data; quantitative assessment of death anxiety; and reporting correlation coefficients or effect estimates for sociodemographic factors, disease-related elements, and psychosocial variables associated with death anxiety. The review focused on peer-reviewed articles published in English between January 2014 and March 2025, without restrictions on sample size or patient demographics. Studies were excluded if they failed to address HF-related death anxiety as a primary research question or outcome; were categorized as a conference report, case study, or editorial; or did not have a readily available full text.
A thorough review of the literature was conducted, encompassing 5 electronic databases: Scopus, PubMed, ScienceDirect, Embase, and ProQuest. The search strategy incorporated keywords related to HF (such as “heart failure” and “cardiac failure”) alongside terms associated with death anxiety (including “death anxiety,” “fear of death,” “death distress”). For instance, a sample query in PubMed was “heart failure” OR “cardiac failure” AND “death anxiety” OR “fear of death”. We applied date restrictions (January 2014 and March 2025) and utilized language filters (English) wherever feasible. In addition to database searches, the author manually reviewed three journals focusing on thanatology and health psychology: Death Studies, Psychological Reports, and OMEGA—Journal of Death and Dying. Recent issues of these journals from January 2014 and March 2025 were carefully examined for pertinent studies. Additionally, the reference lists of all included articles were scrutinized to uncover any further eligible studies.
To assess the methodological rigor of the studies included in this review, the strengthening the reporting of observational studies in epidemiology (STROBE) checklist was employed. Each study underwent a thorough evaluation based on various criteria, including sampling methodologies, measurement validity, clarity of reporting, and potential biases. This appraisal was utilized to enrich the narrative synthesis rather than to exclude studies, which is typical in integrative reviews. Overall, all 12 papers were found to have met the quality assessment according to the STROBE checklist.
All retrieved records were imported into reference management software (EndNote version 21), and the duplicates were eliminated. Figure 1 presents the PRISMA flow diagram that illustrates the study selection process. Initially, a total of 1782 records were identified, comprising 1668 from databases and 114 from manual journal searches. After removing duplicates and records not related to death anxiety, 106 unique records were screened based on their titles and abstracts, resulting in the exclusion of 62 as irrelevant. The author subsequently examined 32 full-text articles for eligibility, of which 20 were excluded for various reasons: they did not employ an observational design, lacked an abstract, failed to report mean death anxiety scores, or were in languages other than English. Ultimately, 12 studies met all criteria and were included in the review.
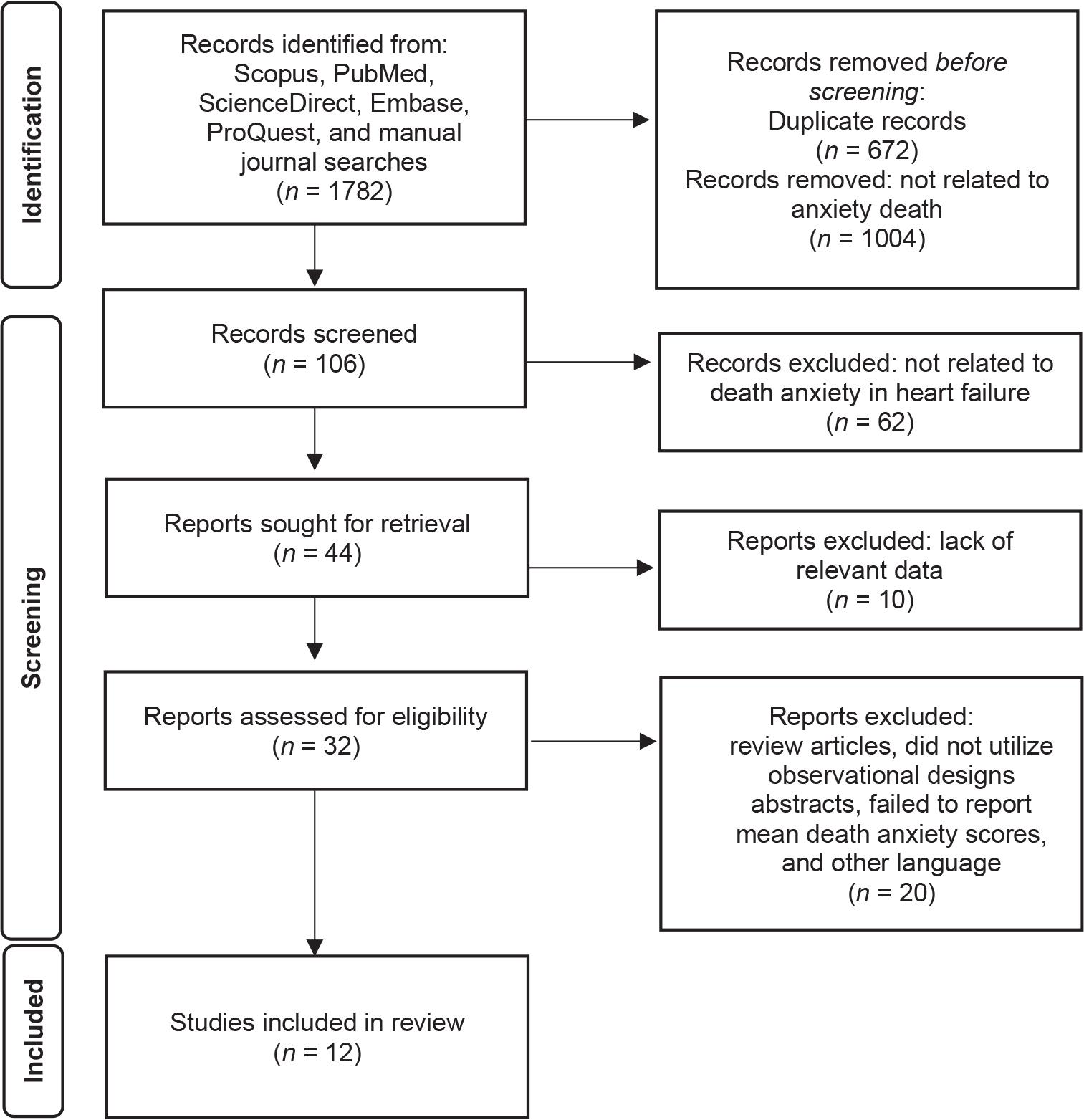
Literature search flowchart.
For each included study, the author extracted key data, including citation details (author and year), country and setting, study design, sample size and characteristics, the death anxiety measurement scale used, and the reported mean and standard deviation (SD) of death anxiety scores among patients with HF. These data were compiled into a summary table for comparison. The author compared death anxiety levels across studies, interpreting means within the context of their respective scale ranges, and noted relevant factors, such as clinical or demographic correlates. Each study was critically appraised on sample size, representativeness, measurement validity, and biases.
Table 1 provides an overview of 12 observational studies that met the inclusion criteria for this integrative review, covering the years from 2014 to 2025. The majority of these studies were conducted in Iran (58.33%),4,6,10–14 followed by Turkey (33.34%)7,15–17 and the USA (8.33%).18 Most utilized a cross-sectional design (75.00%),6,7,10,12–17 while others employed mixed-method longitudinal approaches (8.33%),18 quasi-experimental designs (8.33%),4 and a randomized controlled trial (8.33%).11 In terms of sample size, the majority consisted of 101–150 participants (41.67%),7,10–12,17,18 followed by those with more than 200 participants (33.33%),10,13–15 those with fewer than 100 participants (16.67%),4,6 and finally, those with 150–200 participants (8.33%).16
Characteristics of included studies.
| Characteristics of studies | Number of studies (n) | Percentage (%) |
|---|---|---|
| Country | ||
| Iran | 7 | 58.33 |
| Turkey | 4 | 33.34 |
| USA | 1 | 8.33 |
| Design | ||
| Cross-sectional | 9 | 75.10 |
| Mixed-method longitudinal | 1 | 8.33 |
| Quasi-experimental | 1 | 8.33 |
| Randomized controlled trial | 1 | 8.33 |
| Sample size | ||
| <100 | 2 | 16.67 |
| 101-150 | 5 | 41.67 |
| 150-200 | 1 | 8.33 |
| >200 | 4 | 33.33 |
Most studies (n = 7) used the original or culturally adapted Templer Death Anxiety Scale (DAS). The original DAS is a 15-item self-report tool with True/False response options, yielding a total score range of 0–15, where higher scores indicate greater fear of death. However, several included studies (n = 4) employed Likert-type adaptations (e.g., 1–5 scale), resulting in score ranges of 15–75. Severity levels (e.g., low, moderate, high) were interpreted based on predefined cutoffs or tertile splits reported by the study authors. One study conducted in Iran utilized the Death and Dying subscale from the World Health Organization Quality of Life (WHOQOL) measure.18 This variation in format was accounted for when comparing average death anxiety scores across studies (Table 2).
Summary of included studies on death anxiety in HF.
| Authors (years) | Purpose | DAS | Score range | Mean death anxiety (SD) | Severity interpretation | Main findings |
|---|---|---|---|---|---|---|
| Asgari et al. (2018)6 | To examine death anxiety and its relationship with demographics in patients with HF | Templer DAS (15-item) | 15–75 | 47.95 ± 6.91 | Moderate–high | Over 90% of patients experienced moderate to severe death anxiety |
| Çamcı et al. (2024)7 | To explore the relationship between religious coping and death anxiety in HF | Templer DAS (15-item) | 0–15 | 7.78 ± 3.91 | Moderate–high | Higher death anxiety associated with longer HF duration; weak positive correlation with religious coping |
| Ghorbani et al. (2023)12 | To compare spiritual experiences and death anxiety in HF vs angina patients | Templer DAS (15-item) | 15–75 | 43.15 ± 13.41 | Moderate–high | Significant negative correlation between spiritual experience and death anxiety |
| Merati et al. (2024)13 | To examine relationship between QoL and death anxiety in patients with HF | Templer DAS (15-item) | 15–75 | 7.54 ± 2.35 | Moderate–high | Higher death anxiety associated with poorer QoL (r = 0.329, P < 0.001) |
| Sacco et al. (2014)18 | To investigate psychosocial resources and well-being in HF | DAS/WHOQOL | 0–10 | 5.58 ± 2.62 | Moderate | Religious/spiritual support associated with lower death anxiety |
| Yildirim et al. (2024)17 | To explore associations between death anxiety, loneliness, and hope | Templer DAS (15-item) | 0–15 | 10.41 ± 3.94 | High | Death anxiety positively predicted by age and loneliness (R2 = 23.1%) |
| Sazak et al. (2025)15 | To examine spiritual orientation and frailty mediated by death anxiety | Templer DAS (15-item) | 0–15 | 8.03 ± 4.45 | Moderate–high | Death anxiety mediated the relationship between spiritual orientation and frailty |
| Soleimani et al. (2020)14 | To identify predictors of death anxiety among cardiac patients | Templer DAS (15-item) | 15–75 | 45.15 ± 8.44 | Moderate–high | Greater economic standing, reliance on friends as a primary income source, older age, stronger religious faith, and heightened hope were linked to reduced death anxiety. |
| Moradi et al. (2022)4 | To assess cognitive-behavioral therapy’s effect on death anxiety and depression in HF | Templer DAS (15-item) | 0–15 | 9.96 ± 1.69 | Moderate–high | Cognitive-behavioral therapy significantly reduced death anxiety in patients with HF (P < 0.001). |
| Aryafard et al. (2023)10 | To examine correlations of death anxiety with spirituality and resilience | Templer DAS (15-item) | 0–15 | 7.21 ± 2.22 | Moderate | Religious attitude and resilience inversely associated with death anxiety |
| Batı et al. (2024)16 | To explore self-care agency and death anxiety among elderly | Templer DAS (15-item) | 0–15 | 6.76 ± 3.25 | Moderate | Very weak positive correlation between self-care and death anxiety (r = 0.158, P = 0.004) |
| Babaei Vahed et al. (2022)11 | To evaluate illness perception training on death anxiety in HF | Templer DAS (15-item) | 0–15 | NR | Moderate | Training on illness perception significantly reduced anxiety about death, with a pre- to post-training change that was statistically significant (P < 0.001). |
Note: DAS, death anxiety scale; HF, heart failure; NR, not reported; QoL, quality of life; SD, standard deviation; WHOQOL, World Health Organization Quality of Life.
Most studies used the original or adapted Templer DAS, a 15-item tool with either a True/False (score range: 0–15) or Likert-type (score range: 15–75) format. Higher scores indicate greater death anxiety. Severity classifications were based on original scale thresholds or tertile splits defined by study authors.—Studies using modified or single-item versions of DAS/WHOQOL were evaluated using author-defined interpretation thresholds.—One study (Sacco et al.18) used a single item from WHOQOL; therefore, comparison is limited.
All 5 studies indicate that, on average, patients with HF experience moderate to high levels of death anxiety. However, numeric mean values are not directly comparable without considering the specific scale used. The current review of 12 studies revealed that death anxiety is a common psychological concern among patients with HF, often reaching moderate to high levels. Most of these studies utilized the Templer DAS, finding that various sociodemographic, disease-related, and psychosocial factors significantly influence death anxiety. For example, Asgari et al.6 reported that over 90% of patients with HF experienced moderate to severe levels of death anxiety, which were significantly predicted by older age and feelings of loneliness.17 Similarly, research by Merati et al.13 found that poorer QoL, prolonged disease duration, and lower economic status were strongly associated with increased death anxiety levels.14
Several studies also emphasized the protective roles of spirituality, religious coping, and resilience. Aryafard et al.,10 Ghorbani et al.,12 and Sazak et al.15 showed that a greater spiritual orientation and positive religious attitudes were significantly correlated with lower levels of death anxiety and, in some instances, mediated its effects on frailty and psychological outcomes. Additionally, intervention studies have provided encouraging evidence that psychosocial support can alleviate death anxiety. For instance, Moradi et al.4 found that cognitive-behavioral therapy (CBT) significantly reduced death anxiety post-treatment, while Babaei Vahed et al.11 observed a similar effect through illness perception education. Overall, these findings highlight the complex, multifactorial nature of death anxiety in patients with HF and support the integration of psychosocial and spiritual care into standard HF management.
This integrative review highlights that death anxiety is a significant psychological concern among patients with HF. Analyzing 12 observational studies conducted between January 2014 and March 2025, the average death anxiety scores in HF populations consistently fell within the moderate to high range, depending on the version of the measurement tool used.6 These findings indicate that many patients with HF experience existential distress due to the chronic, life-threatening nature of their condition.
The severity of illness appears to be linked to death anxiety. Patients with advanced HF who have lived with the condition for 3 or more years exhibited higher levels of death anxiety compared to those who were more recently diagnosed.5,7 To contextualize this, in literature, patients with HF demonstrate a greater fear of death on average than what has been reported among healthy adults and even in some other chronic illness groups. For instance, Asgari et al.6 found that the mean death anxiety score in patients with HF (mean = 47.95, SD ± 6.19) was higher than previously noted in patients undergoing hemodialysis. This suggests that HF may elicit a unique level of anxiety due to its unpredictable progression, characterized by acute exacerbations.2,19 This may seem counterintuitive, given the possibility of adaptation over time, but it likely reflects the cumulative burden of symptoms and frequent hospitalizations that serve as reminders of their mortality.20 These findings echo patterns seen in patients with advanced cancer8 but also align with evidence from other chronic conditions such as chronic obstructive pulmonary disease (COPD)21 and stroke,22 where disease-related disability and dependence also contribute to increased death anxiety. Future studies should explore how death anxiety evolves over time in relation to disease trajectory and symptom burden.18,23
Common predictors of higher death anxiety included older age, social isolation, lower socioeconomic status, and longer HF duration.14,17 For example, older individuals and those experiencing social isolation were more likely to exhibit elevated death anxiety, potentially due to a heightened awareness of mortality and limited support networks.24,25 Additionally, patients with a longer duration of HF or those in more severe disease stages were also more prone to report increased death anxiety,7 reinforcing the notion that disease progression raises existential concerns. These findings highlight the necessity for personalized psychological screening and support throughout the disease trajectory.
An important observation in this review is the geographical concentration of studies—with the majority conducted in Iran (58.33%),4,6,10–14 and Turkey (33.34%).7,15–17 This may reflect regional research priorities or cultural openness toward studying existential and spiritual phenomena. Additionally, religious and cultural attitudes toward death in these societies—where spiritual practices are more embedded in daily life—could influence both the prevalence and expression of death anxiety. However, this also raises concerns about generalizability, as findings may not fully translate to patients in Western or East Asian settings where death may be viewed differently. Future research should intentionally sample diverse populations to explore cultural variations in death anxiety.
Psychosocial and cultural factors play a significant role in death anxiety. Research consistently shows that spirituality and religious coping mechanisms can mitigate feelings of death anxiety. Patients with strong spiritual orientation, religious coping strategies, or higher resilience reported lower death anxiety.10,12,15 For instance, Ghorbani et al.12 identified a notable negative correlation between spiritual experiences and death anxiety, while Sazak et al.15 found that death anxiety acted as a mediator in the relationship between spiritual orientation and frailty. These findings resonate with existential theories positing that spirituality helps individuals find meaning, alleviate the fear of death, and build resilience in the face of illness.26 This is also consistent with the Terror Management Theory,27 which posits that cultural worldviews and self-esteem buffer individuals from death-related fears. Incorporating spiritual care and resilience-building into psychosocial interventions could be particularly beneficial for patients with HF, especially in multicultural care settings.28
Encouragingly, 2 studies demonstrated that targeted psychosocial interventions could reduce death anxiety. For instance, Moradi et al.4 found that CBT significantly reduced levels of death anxiety and depression among patients with HF. Similarly, Babaei Vahed et al.11 reported that an educational protocol designed to enhance illness perception led to statistically significant decreases in death anxiety. These findings indicate that structured psychosocial support—particularly when centered around cognitive reframing and patient education—can be valuable elements of HF care. Future intervention studies should include multicomponent strategies that address cognitive, emotional, and spiritual domains.
This review followed a systematic methodology; however, it is essential to recognize its several limitations. The search was limited to published studies in English, which raises concerns about potential publication bias, as studies with significant findings are more likely to be available in this language. Additionally, the review included only 12 studies, reflecting the nascent stage of research in this area. As a result, our ability to draw detailed conclusions, such as identifying specific predictors of high death anxiety, is limited. Furthermore, the majority of the studies originated from Middle Eastern countries, which may restrict the applicability of the findings to other cultural contexts. It remains uncertain whether Western patients with HF would report higher or lower levels of death anxiety, given the diverse cultural attitudes toward death. Future research should emphasize longitudinal designs, the inclusion of multiethnic samples, and mixed-method approaches to capture both the quantitative and the experiential dimensions of death anxiety. Despite these limitations, the consistency of the results bolsters confidence in the overarching message. The variability in death anxiety measures and scoring systems, all based on the Templer DAS, complicated direct comparisons of severity across studies. Additionally, it is advisable to consider theoretical frameworks such as Terror Management Theory or palliative care models to inform the development of interventions, and to evaluate the integration of spiritual assessments and resilience-enhancing strategies within HF care.
This integrative review demonstrates that death anxiety is a prevalent and impactful psychological concern among individuals living with HF. Across diverse observational studies, patients consistently reported moderate to high levels of death anxiety, which were influenced by a combination of demographic, clinical, and psychosocial factors. Key contributors included older age, loneliness, low socioeconomic status, and longer duration of illness, while spirituality, religious coping, resilience, and psychosocial interventions served as important protective factors. These findings underscore the need to routinely assess death anxiety in clinical practice and to develop multidisciplinary strategies that address patients’ emotional, existential, and spiritual needs. Incorporating evidence-based psychological interventions, such as CBT and illness perception training, alongside spiritually supportive care, may enhance the overall QoL and emotional well-being of patients with HF. Future research should expand to include more diverse geographic and cultural settings, adopt longitudinal and theory-driven designs, and further explore intervention effectiveness. Importantly, any efforts to reduce death anxiety must be culturally sensitive, respecting patients’ values, beliefs, and worldviews to ensure meaningful and equitable care across settings.