
Upper crossed syndrome is a postural syndrome with myofascial imbalance within the shoulder girdle and the cervical spine. It is manifested through increased cervical lordosis and thoracic kyphosis as well as excessive shoulder protraction [1]. This condition developed in the course of human evolution from active to sedentary lifestyle.
The disorder of muscle structure balance is the main cause of the above-mentioned myofascial imbalance. It is accompanied by tonic muscle hyperactivity as well as phasic muscle inhibition and improper control of the central nervous system over muscle coordination. A starting point of this dysfunction is the formation of an improper body posture which leads to uneven joint loads that affect a stable and proper body posture. Joint receptors send afferent information which leads to the reconstruction of movement patterns in cortical memory. A stereotype of improper body posture is formed and muscle balance is disturbed [2]. Its consequences in terms of particular muscles are shown in figure 1.
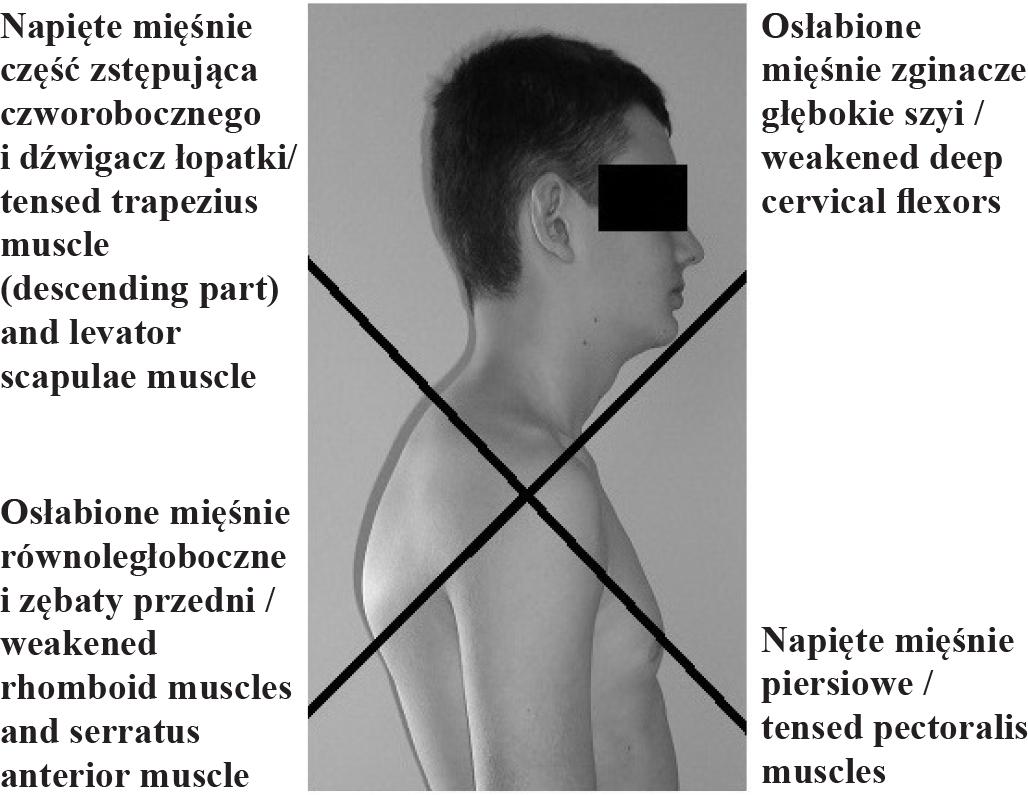
Upper crossed syndrome
It is important to start correcting upper crossed syndrome early because postural overload that lasts too long results in the progression of symptoms that have already occurred. As a result, tissue fibrosis and a permanent abnormal posture may occur [3]. It shows that fibroblasts of overloaded muscles (muscles with eccentric loading) increase collagen production within and around these muscles in order to create better conditions for bearing increased loads. It is accompanied by the reduced hydration of the extracellular matrix ground substance. When excessive loading occurs, piezoelectric discharge takes place that spreads along the fascia and around muscles. Consequently, the created collagen fibres start to run along acting forces which create overloading. Afterwards, adjacent fibres are connected via hydrogen bonds made of interfibrous glue. In this way, non-elastic structures are formed around eccentrically loaded muscles [4]. Dysfunctions of myofascial complex lead to restricted ranges of motion in particular joints. In the case under discussion, restricted cervical and thoracic ranges of motion occurred [5].
In physiotherapy, myofascial dysfunctions are treated with myofascial techniques and massage [1,3,6]. However, the effectiveness, dynamics of changes as well as retention period of these therapy forms in the treatment of asymptomatic postural syndrome have not been fully explored as yet. The aim of this work was to indicate which therapy form (myofascial techniques or massage) is more effective in terms of myofascial release in persons with upper crossed syndrome.
The study included 18 individuals (12 females and 6 males) with upper crossed syndrome who were randomly assigned to one of the two groups. The research, which lasted for 2 months, was carried out in the rural environment in winter. Group 1 (n=9) consisted of 8 females and 1 male, while group 2 (n=9) included 4 females and 5 males. The description of the study groups is presented in table 1. The analysis performed with the Mann-Whitney U test revealed that the groups under investigation did not differ significantly in age and body height. However, the participants from group 2 demonstrated significantly higher body weight values than the subjects from group 1 (p<0.05).
Description of the study groups
| Zmienna/ | Grupa I/ | Grupa II/ | ||
|---|---|---|---|---|
| Śr.±SD/ | min-maks/ | Śr.±SD/ | min-maks/ | |
| Wiek [lata]/ | 32±12,77 | 17-51 | 36±12,52 | 21-55 |
| Masa ciała [kg]/ | 55±9,90* | 46-76 | 72±13,80* | 52-98 |
| Wysokość ciała [cm]/ | 163±8,19 | 155-176 | 170±6,27 | 160-178 |
| BMI [kg/m2]/ | 20,1±4,00* | 17,2-29,7 | 24,8±3,78* | 19,4-30,9 |
variable values differ significantly between the groups (p<0.05)
The occurrence of upper crossed syndrome diagnosed on the basis of body posture point evaluation according to Kasperczyk was the study inclusion criterion [7]. The following aspects were analysed: position of the head, shoulders, scapulae and abdomen as well as the degree of thoracic kyphosis and lumbar lordosis in the sagittal plane in a standing position. Each element under evaluation was given points according to the following scale: 0 points – proper posture, 1 point – slight deviation from the proper posture, 2 or 3 points – considerable deviation from the proper posture [7]. The total number of points obtained by each study participant was recorded in the evaluation form and it constituted the basis for upper crossed syndrome assessment. It was assumed that an overall score of at least 6 points was considered as the study inclusion criterion. The orthopaedic assessment of each subject was performed by the same examiner.
The exclusion criteria were as follows: over 60 years of age at the time of the examination, neurological, cardiovascular and oncological diseases and as well as dermatological conditions of the back and the back of the nape. Moreover, individuals who experienced pain during cervical movements or when reaching the limit of the cervical range of motion were excluded from the study.
The study participants were randomly assigned to one of the two therapy groups. In group 1, myofascial techniques were applied, while subjects from group 2 received massage. In both groups, the therapy consisted of five 30-minute daily sessions. During the sessions, therapeutic interventions were performed on the following body parts: the nape (descending part of the trapezius muscle, the levator scapulae muscle), the skull base (suboccipital muscles), the anterior part as well as both lateral parts of the chest (pectoralis major, pectoralis minor, external intercostal muscles), lateral areas below costal arches and the anterior part of the neck (the sternocleidomastoid muscle). In group 1, myofascial techniques were applied to make soft tissues more elastic. They were performed in the following order: I) Myofascial release through stretching connective subcutaneous tissue. Methodology: a therapist held a skinfold between his thumbs which he moved closer until tissue resistance was felt. This tensed position was maintained for 5 seconds. Then, the thumbs were moved to adjacent area within a given structure, i.e. the descending part of the trapezius muscle and the pectoralis major muscle. The next step involved removing the restriction of the diaphragm. Methodology: 1) placing both thumbs under the costal arch and increasing pressure after expiration, repeated 5 times on each side; 2) holding both costal arches simultaneously and pulling them towards the head during expiration, repeated 3 times. The techniques were performed every day. II) Trigger point compression release by means of progressive pressure. Methodology: after finding a trigger point in particular muscles, i.e. suboccipital muscles, the levator scapulae muscle and the pectoralis minor muscle, constant pressure that evoked pain was applied. When pain subsided, the pressure was increased. The procedure was repeated 3 times, i.e. on the 1st, 3rd and 5th day of the therapy. III) Post -isometric muscle relaxation. Methodology: hypertonic muscle was passive until tissue resistance was felt. Afterwards, the participant tensed a particular muscle as a result of resistance put up by the therapist (20% of maximum tension value). The tension was maintained for 10 seconds and then, at expiration, the muscle was extended until tissue resistance was felt again. The procedure was repeated 5 times. After that, 5-second isometric tension of the antagonistic muscle group was applied. It was performed on both sides of the trapezius muscle (descending part), the levator scapulae muscle, the sternocleidomastoid muscle, suboccipital muscles and the pectoralis major muscle. The technique was used every day. IV) Active release technique. Methodology: the therapist applied vertical pressure on a given structure, while the patient performed movements in the direction this structure extended in the maximum possible range of motion at a given moment (the pressure applied by the therapist limited the range of motion). The procedure was repeated 3 times in each area. The technique was performed on both sides on the trapezius muscle (descending part) and the pectoralis minor muscle [8–10]. Group 2 underwent the therapy with the use of massage. In this case, the sequence of techniques was the same during each session but the pressure was gradually increased. At the beginning, longitudinal stroking with medium force was performed (for 1 minute along each structure). Then, deep longitudinal rubbing was performed (for 2 minutes along each structure) followed by longitudinal kneading (for 2 minutes along each structure) and thumb kneading (for 2 minutes along each structure). The above techniques were applied on both sides of such areas as the nape, upper anterior chest and the costal arch area [11]. The therapies in both groups were performed in a supine and prone position. During the therapy and for the 2 weeks after its completion, the participants did not undergo any physical therapies or rehabilitation procedures.
In order to assess the effects of selected techniques on the myofascial complex, chest mobility and cervical spine mobility were measured on the 1st day of the therapy (before and immediately after the session), on the 5th day of the therapy (immediately after the session) and 14 days after the therapy completion. All the measurements were performed by the same person. To assess chest mobility, suprasternale height was measured at maximum inspiration in a standing position. The participant performed maximum inspiration and sustained it for 3 seconds. Each of the measurements was repeated 3 times, and a mean of the obtained results was used in the analysis. Suprasternale height was measured with the use of an anthropometer whose pointer was placed at the suprasternal notch [12]. The measurement of cervical range of motion was performed with the use of a measuring tape (in centimetres) in a standing position [13]. The following directions of the cervical spine range of motion were measured: forward flexion (the distance between external occipital protuberance and spinous process of C7), right and left side bending (the distance between mastoid process and acromion) and left and right rotation (the distance between the tip of the chin and acromion).
Statistical analysis was performed with the use of STATISTICA version 10 software (StatSoft Inc. 2011). Statistical significance of differences between mean values obtained in the measurements was evaluated with the Wilcoxon signed-rank test. The same test was applied in the assessment of the significance of differences between mean ranges of motion to the right and left (cervical rotations and side bending). In order to compare mean values of cervical ranges of motion and suprasternale height between particular treatment stages and between both groups, the Mann-Whitney U test was applied.
Tables 1 and 2 present values of the ranges of motion of the cervical spine and suprasternale height during an initial measurement, on the 1st and 5th day of the therapy and 14 days after its completion.
Ranges of motion of the cervical spine and suprasternale height prior to the therapy, during the therapy (1st and 5th day) and 14 days after its completion in group 1 (individuals undergoing the therapy with myofascial techniques)
| Badany parametr/ | Moment wykonania pomiaru/ | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| przed terapią/ | 1 dnia po terapii/ | 5 dnia po terapii/ | 2 tyg. od zakończenia terapii/two weeks after the therapy completion | ||||||
| Śr.±SD/ | min-maks/ | Śr. ±SD/ | min-maks/ | Śr.±SD/ | min-maks/ | Śr. ±SD/ | min-maks/ | ||
| Odc. C/C-spine | zginanie/ | 1,9±0,96 | 0,5-3,5 | 2,1±0,96 | 1,0-4,5 | 1,9±0,92 | 1,0-4,0 | 2,0±0,97 | 0,8-4,0 |
| skłon P/ | 3,8±1,18 | 2,0-5,5 | 4,1±1,11 | 2,0-5,5 | 4,5±1,05* | 2,5-6,0 | 4,4±1,12 | 2,5-6,0 | |
| skłon L/ | 4,7±2,94 | 2,0-12,5 | 4,3±1,29 | 2,0-6,5 | 4,7±1,29 | 2,5-6,5 | 4,9±1,59 | 2,3-7,5 | |
| rotacja P/R rotation | 6,9±1,32 | 5,0-9,0 | 7,9±1,14* | 6,0-9,5 | 8,4±0,93* | 7,0-10,0 | 7,6±1,05 | 6,5-9,5 | |
| rotacja L/L rotation | 7,9±2,09 | 4,5-12,5 | 7,4±1,21 | 5,0-9,5 | 8,1±1,02 | 6,0-9,5 | 8,5±0,91 | 7,0-10,0 | |
| KLP/chest | wysokość supraster-nale/ suprasternale | 133,3± 6,83 | 124,5-145,0 | 133,9± 6,99 | 125,0-145,3 | 134,8± 6,89* | 124,2-146,6 | 134,6± 6,71* | 124,9-145,8 |
the range of motion differs significantly from the range achieved prior to the therapy (p<0.05)
The ranges of motion of the cervical spine in an initial measurement prior to the therapy did not vary significantly between the examined groups. No significant differences between the right and left side in rotational movements and in lateral flexions of the cervical spine were revealed in either of the groups. The suprasternale height in group 2 was significantly higher than in group 1 (p<0.05). (Table 1, Table 2).
An increase in the range of motion of the cervical flexion in group 1 after the 1st day of the therapy was insignificant at the level of 16%. However, after the 5th day of the therapy and 2 weeks after its completion, the range of motion did not differ from an initial measurement. In group 2, an increasing tendency was noted. After the first day of the therapy, the range of motion increased by 8%, after the 5th day it was 29% higher than the initial measurement, while 2 weeks after the therapy completion, an increase was at the level of 12%. However, the results achieved in this group were not significant, either (Table 3).
Ranges of motion of the cervical spine and suprasternale height prior to the therapy, during the therapy (1st and 5th day) and 14 days after its completion in group 2 (individuals undergoing the massage therapy)
| Badany parametr/ | Moment pomiaru/ | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| przed terapią/ | 1 dnia po terapii/ | 5 dnia po terapii/ | 2 tyg. od zakończenia terapii/two weeks after the therapy completion | ||||||
| Śr. ±SD/ | min-maks/ | Śr. ±SD/ | min-maks/ | Śr. ±SD/ | min-maks/ | Śr. ±SD/ | min-maks/ | ||
| Odc. C C-spine | Zginanie/ | 2,4±0,91 | 1,0-4,0 | 2,6±0,99 | 1,0-4,0 | 3,1±0,70 | 2,0-4,3 | 2,7±0,97 | 1,5-4,3 |
| skłon P/ | 3,8±0,97 | 3,0-6,0 | 4,0±1,91 | 2,5-9,0 | 4,2±1,39 | 2,5-6,2 | 4,5±1,50 | 2,5-7,5 | |
| skłon L/ | 4,3±2,31 | 1,0-8,0 | 4,2±2,16 | 1,5-9,0 | 4,4±1,92 | 1,0-8,5 | 4,3±1,47 | 2,0-7,0 | |
| rotacja P/R rotation | 7,3±1,27 | 6,0-9,0 | 6,6±1,56 | 4,5-9,3 | 8,6±1,12 | 7,0-11,0 | 8,7±0,85* | 7,5-10,0 | |
| rotacja L/L rotation | 7,2±2,13 | 2,5-10,5 | 7,2±1,58 | 4,5-9,0 | 8,1±1,12 | 6,0-10,0 | 8,2±1,31 | 6,5-10,0 | |
| KLP chest | wysokość supraster-nale/ | 140,9± 4,92 | 131,8-148,4 | 141,9± 4,96* | 132,7-148,7 | 142,4± 5,27* | 133,5-150,0 | 141,7± 4,47 | 132,6-147,1 |
the range of motion differs significantly from the range achieved prior to the therapy (p<0.05)
The range of motion of the right side bending increased in both groups. After the 1st day of the therapy, it increased insignificantly by 8% in group 1, while in group 2 it was higher by 5%. After the 5th day of the therapy, it increased significantly by 18% in group 1 (p<0.05), while in group 2 an increase was insignificant (by 10%). Two weeks after the therapy completion, the right side bending had an insignificantly bigger range of motion compared to the initial measurement in both groups (by 16% in group 1, by 18% in group 2) (Table 3). The range of motion of the left side bending decreased after the 1st day of the therapy in both groups, while in other measurements, it did not differ significantly from the initial examination (Table 3).
In group 1, the range of the right rotation after the first day of the therapy increased significantly by 15% (p<0.05). Then, after 5 days of the therapy an increase by 22% was also significant (p<0.05). However, 2 weeks after the therapy completion, it was insignificantly higher than the initial measurement (by 12%). In group 2, after the 1st day of the therapy, the range of motion increased insignificantly by 8%, while after the 5th day an insignificant increase by 18% was noted. A significant increase (by 19%) in the right rotation with regard to the initial measurement was observed 2 weeks after the therapy completion (p<0.05) (Table 3). As far as the left rotation is concerned, there were no significant changes in the range of motion compared to the initial measurement. In group 1, the results revealed considerable variability, i.e. after the 1st day of the therapy, an increase by 6% was noted, on the 5th day the results returned to the initial measurement values and 2 weeks after the therapy completion they increased by 8%. In turn, in group 2, the range of motion did not increase after the 1st day of the therapy. However, after the 5th day, it increased by 13%, while 2 weeks after the therapy completion it was higher by 14% compared to the initial measurement (Table 3).
Both myofascial techniques and massage led to an increase in suprasternale height during the therapy. After the 1st day of the therapy, compared to the initial measurement, an increase by 0.5% was noted in group 1, while in group 2 it was at a significant level, i.e. 0.7% (p<0.05). After the 5th day of the therapy, a significant increase (by 1%) in the examined parameter was observed in both groups (p<0.05). However, the effect achieved with the use of myofascial techniques after 2 weeks was maintained at a significant level (by 1%) (p<0.05), while suprasternale height in the group in which massage was applied did not differ significantly from the initial measurement (Table 3).
Increases in the range of motion of the cervical spine and in suprasternale height after the 1st day of the therapy (Δ1), after the 5th day of the therapy (Δ2) and 2 weeks after the therapy completion (Δ3)
| Przyrost zakresu ruchu/Increase in the range of motion | Grupa I/Group 1 | Grupa II/Group II |
|---|---|---|
| Zgięcie/Flexion | ||
| Δ1 [cm] | 0,3 | 0,2 |
| Δ2 [cm] | 0 | 0,7 |
| Δ3 [cm] | 1,0 | 0,3 |
| Skłon boczny w prawo/Right side bending | ||
| Δ1 [cm] | 0,3 | 0,2 |
| Δ2 [cm] | 0,7* | 0,4 |
| Δ3 [cm] | 0,6 | 0,7 |
| Skłon boczny w lewo/Left side bending | ||
| Δ1 [cm] | -0,3 | -0,1 |
| Δ2 [cm] | 0 | 0,1 |
| Δ3 [cm] | 0,2 | 0 |
| Rotacja w prawo/Right rotation | ||
| Δ1 [cm] | 1,0* | -0,6 |
| Δ2 [cm] | 1,5* | 1,3 |
| Δ3 [cm] | 0,8 | 1,4* |
| Rotacja w lew/Left rotation | ||
| Δ1 [cm] | 0,5 | 0 |
| Δ2 [cm] | 0,2 | 0,9 |
| Δ3 [cm] | 0,6 | 1,0 |
| Wysokość suprasternale/Suprasternale height | ||
| Δ1 [cm] | 0,6 | 1,0* |
| Δ2 [cm] | 1,5* | 1,5* |
| Δ3 [cm] | 1,3* | 0,8 |
the difference between the range of motion measured before the therapy and the range of motion at a particular moment of the therapy is statistically significant (p<0.05)
Upper crossed syndrome is a pathology characterised by significant body posture deviations from the commonly accepted norms [1,7]. Thus, its treatment should be based on the guidelines of postural education. The research described in this work refers directly to an improvement in the first phase of the motor control, i.e. the recovery of the mobility of the upper segment of the spine and shoulder girdle. Changes in the cervical spine mobility were observed, i.e. in the area which was directly affected by the postural changes in the upper crossed syndrome. In the available literature, there is no information regarding an influence of myofascial techniques or massage on the correction of upper crossed syndrome. Moore described a case study in which neck pain of a patient with upper crossed syndrome disappeared within a few weeks. However, a variety of the applied techniques such as chiropractice, cryotherapy, myofascial release or exercises, makes it impossible to assess the effectiveness of particular types of therapeutic procedures [14].
Assessing the effects of therapeutic techniques on an improvement in motor functions of a patient has posed a challenge for numerous researchers for many years. Efficient measurement methods which have a status of a “golden standard” in diagnosis are still being sought. Diagnosis with the use of X-ray imaging is perceived as such a standard in examining mobility; however, due to risks connected with exposure to radiation, other solutions are looked for [15].
Szubzda et al. assessed the influence of the therapeutic massage on an improvement in mobility and a decrease in spinal pain. The research group included 25 individuals (13 with cervical discopathy, 12 with lumbar discopathy). A linear measurement of spinal mobility (bend, extension, lateral flexion, rotation) was applied as a research tool. Also, the modified Melzack’s Pain Questionnaire was used. The mobility measurements were performed on the first day of the therapy and after 10 therapeutic sessions. On the basis of the obtained results, it was concluded that the applied therapy significantly increased ranges of motion of the spine, decreased pain and changed its character [16].
Topolska et al. assessed the effectiveness of the therapeutic massage in patients with cervical pain caused by degenerative changes or discopathy. The research group included 60 participants. Thirty individuals underwent physiotherapy and kinesiotherapy, while the other group of the participants additionally underwent a massage of the cervical spine. In the research, Saunders digital inclinometer was applied. Also, Neck Disability Index and VAS were used. After the therapy completion, a decrease in pain and an improvement in capabilities and functions were noted in both groups. Taking into account these results, it was concluded that massage results in the reduction of pain and the improvement in the quality of life of patients with cervical spine pain. An increase in the range of motion of bend and lateral flexions in the cervical spine was noted in individuals who additionally underwent massage [17].
The results obtained in this work confirm the effectiveness of both myofascial techniques and massage in increasing the ranges of motion in the cervical spine. The range of the right rotation after the 1st day of the therapy in group 1 increased significantly by approximately 14% (p<0.05), while after 5 days of the therapy it increased by 22% (p<0.05) compared to the values measured before the therapy. Moreover, it must be highlighted that 2 weeks after the therapy completion, a range of motion of the cervical spine was still higher than the range of motion measured before the therapy (in group 2 it was slightly bigger than in group 1). It may result from the effects of soft tissue manual work on muscle physiology, e.g. in the area of improving blood supply and regeneration processes [18]. The application of the measuring tape for the measurement of cervical spine mobility is a common procedure in therapy centres. However, it requires caution and precision from the therapist as the risk of measurement errors is relatively high.
Maksymowych et al. suggested measuring the range of the spine rotation with a measuring tape. The distance between suprasternal notch and the tragus of the ear was measured, which, according to the authors, considerably reduces the effects of the spinal flexion during the measurement. The authors also indicated the advantage of this method of measuring cervical rotation over the goniometer-based approach [19].
Youdas compared three methods of measuring the range of motion in the cervical spine, i.e. visual estimation, the use of a universal goniometer and the application of a cervical range of motion instrument (CROM). It turned out that only the range measured with CROM instrument had intraclass correlation coefficient greater than 80%, which was found to be a good result [20].
In 2010, Williams et al. conducted a systematic analysis of the available literature in which numerous methods for measuring the cervical range of motion were reviewed. It was concluded that CROM device was the best instrument for measuring the cervical range of motion both in terms of reliability and validity of the measurements as well as functionality. The application of this device is also well documented in the literature [14]. In light of these conclusions, it seems that in future studies on the methods of measuring the cervical range of motion, CROM device should be applied. It may be really useful when it comes to verifying the hypothesis on the effects of myofascial techniques on the improvement of the cervical range of motion.
Bordoni and Zanier presented a detailed system of connections of the diaphragm with the nervous, cardiovascular and lymphatic systems via the fascial system. They pointed to a significant role of the diaphragm not only while breathing but also in maintaining an optimal body posture. If muscle glide against their fascia is disturbed, there occur changes in the abdominal cavity pressure which is created by the contractions of abdominal muscles, pelvic floor muscles and diaphragm muscles. The authors concluded that it may indirectly lead to pathologies in the functions of this area [21].
The results of the research indicated that making the area located under the costal arches and anterior chest wall more elastic improves chest mobility in the longitudinal dimension both by the application of massage (by 1% after the 5th day of the therapy) and myofascial techniques (by 1% after the 5th day of the therapy). This may indirectly prove the “opening” of the diaphragm and anterior chest wall. Therefore, it seems justified to work on this area while correcting upper crossed syndrome with the expiratory chest position [3]. The obtained results point to the effectiveness of the forms of therapy applied in this work, which is proved by an improvement in suprasternale height and the retention of the effects 2 weeks after the therapy completion.
Due to a small size of the research group as well as measurement methods applied in the study, the results should be treated as a preliminary report, while the conclusions should be perceived as a starting point for perfecting functional diagnosis methods regarding upper spinal segments and the shoulder girdle. The results obtained in this study need to be verified on a larger group of participants referred to a control group. Due to the fact that both methods produced similar effects, we believe that it is worth considering the combined application of selected elements of both therapies so that they complement each other, e.g. the application of massage in order to improve blood supply before the myofascial techniques.
Both myofascial techniques and massage increase the mobility of the cervical spine in individuals with upper crossed syndrome.
Myofascial techniques and massage techniques significantly improve chest mobility in the longitudinal dimension at a similar level.