
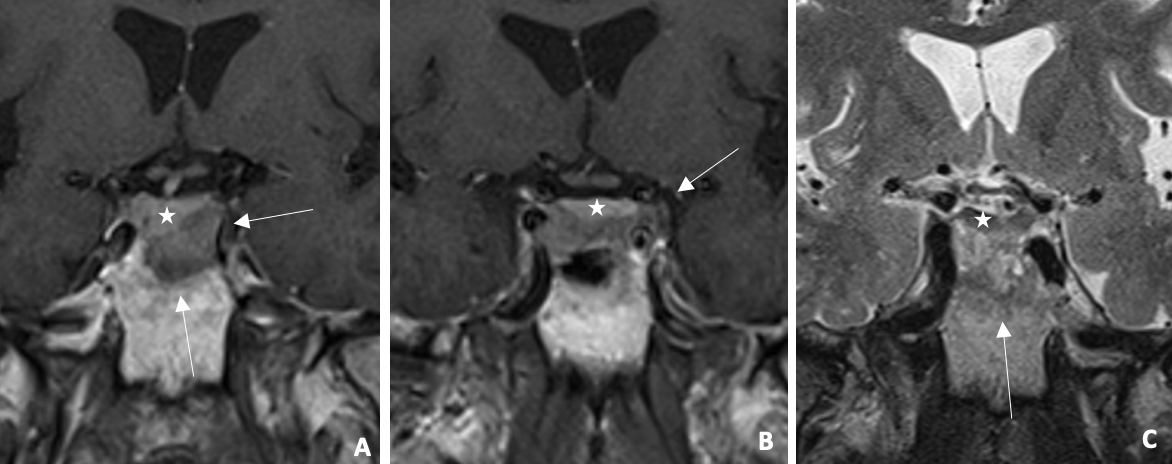
Figure 1
Infiltrative lesion (arrow) centered on the sellar region (A–B) Coronal post‑constrat T1WI: right deviation of pituitary stalk and pituitary gland (star). (C) Coronal T2WI: heterogeneous lesion , adjacent to hypointense pituitary gland. MRI shows infiltrative sellar lesion displacing pituitary stalk/gland.
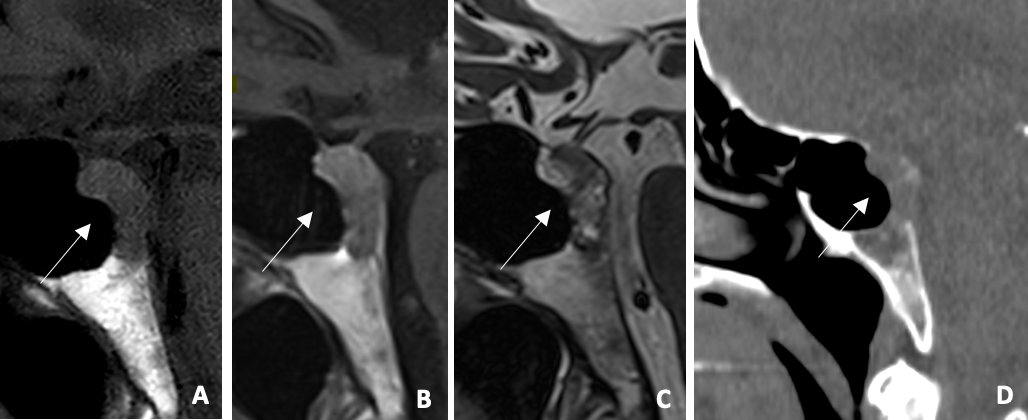
Figure 2
(A) Sagittal T1WI: hypointense expansive clival lesion (B) Sagittal post‑contrast T1WI: mild enhancement (C) Sagittal T2WI: heterogeneous lesion with hyperintense areas (D) Sagittal CT: Lytic clival lesion. Mildy enhancing clival lesion on MRI and lytic on CT.
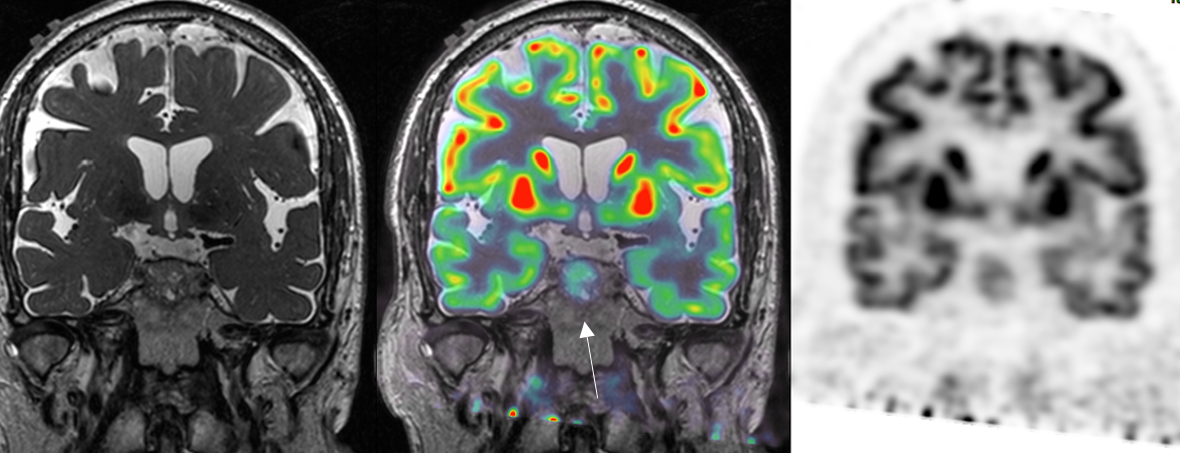
Figure 3
Coronal PET‑CT F18‑FDG with MRI coregistration: moderate uptake of infiltrative sellar lesion. Moderate FDG uptake of infiltrative sellar lesion.
Table 1
Imaging‑based differential diagnosis of most frequent clival lesions.
| PATHOLOGY | IMAGING FEATURES | LOCALIZATION |
|---|---|---|
| Chordoma | Hyperintense on T2WI with soap bubble appearance Thumb sign | Midline, spheno‑occipital synchondrosis |
| Chondrosarcoma | Ring or arc calcifications Hyperintense on T2WI, septa enhancement | Off‑midline, petro‑occipital synchondrosis |
| Plasmacytoma | Punched‑out lytic lesion Isointense on T1/T2WI Homogeneous enhancement | May cross synchondrosis |
| Metastasis | Variable signal, often multifocal | Anywhere |
| Giant Cell Tumor | Expansive well‑defined, cortical thinning | Sphenoïd > temporal > frontal |
| Nasopharyngeal Carcinoma | Erosive lesion, thickening of the posterior nasopharyngeal wall, affecting the adjacent soft tissues | Cavum involvement Cervical lymphadenopathy |