
Cone-beam Computed Tomography (CBCT) is an increasingly used imaging modality. It has a conical X-ray beam and a flat-panel detector. In a single gantry rotation, CBCT acquires an entire volumetric data set, which can be displayed as an isotropic cross-sectional imaging study using specialized 3D image reconstruction algorithms [1].
There are multiple advantages in comparison with multidetector CT (MDCT). It exposes the patient to a lower radiation dose (especially of importance in the pediatric population), while a high-spatial resolution and high-quality images of bony architecture can be achieved with greater detail than MDCT [12345]. It is suitable for postoperative follow-up in patients with metallic implants with use of metal artifact algorithms [36].
In addition, there is a relative low cost of equipment in comparison with MDCT [3].
Some disadvantages exist as well. CBCT is prone to motion artifacts, due to the long scanning time. Also, any motion affects the entire CBCT data set since it uses a volumetric acquisition, whereas on MDCT it may only affect a small portion of the scan [13].
Most currently used CBCT have a limited field of view (FOV), one of the many factors responsible for the low-dose exposure, but a limitation to the use of CBCT when a large bone or joint needs to be examined pre- or postoperatively.
The lower tube voltage and small gantry size compared with MDCT are other important reasons why larger joints (shoulder, hip) and body areas such as the lumbar spine cannot be imaged adequately.
The current new generation of CBCT aims at optimizing the benefits while limiting the traditional disadvantages of CBCT with a larger gantry, higher tube voltage and a moveable table.
In our department, we currently use a CBCT with a gantry of 77 cm patient aperture, a tube voltage of 70–120 kV (selectable in 10 kV steps), and a movable table (NewTom 7G, QR systems, Verona, Italy).
With this larger gantry and higher tube voltage (120 kV), large joints and body parts can be examined. The high-spatial resolution of bony architecture leads to a very good evaluation of fusion material in cervical and lumbar spine (Figure 1). High-spatial resolution images of cartilage surface after intra-articular contrast injection, already shown very useful in other joints such as the wrist [78], can now be obtained in the shoulder joint (Figure 2). The availability of fluoroscopy makes it possible to perform the contrast injection while the patient is installed for the scan, keeping the time between injection and scan to a minimum.
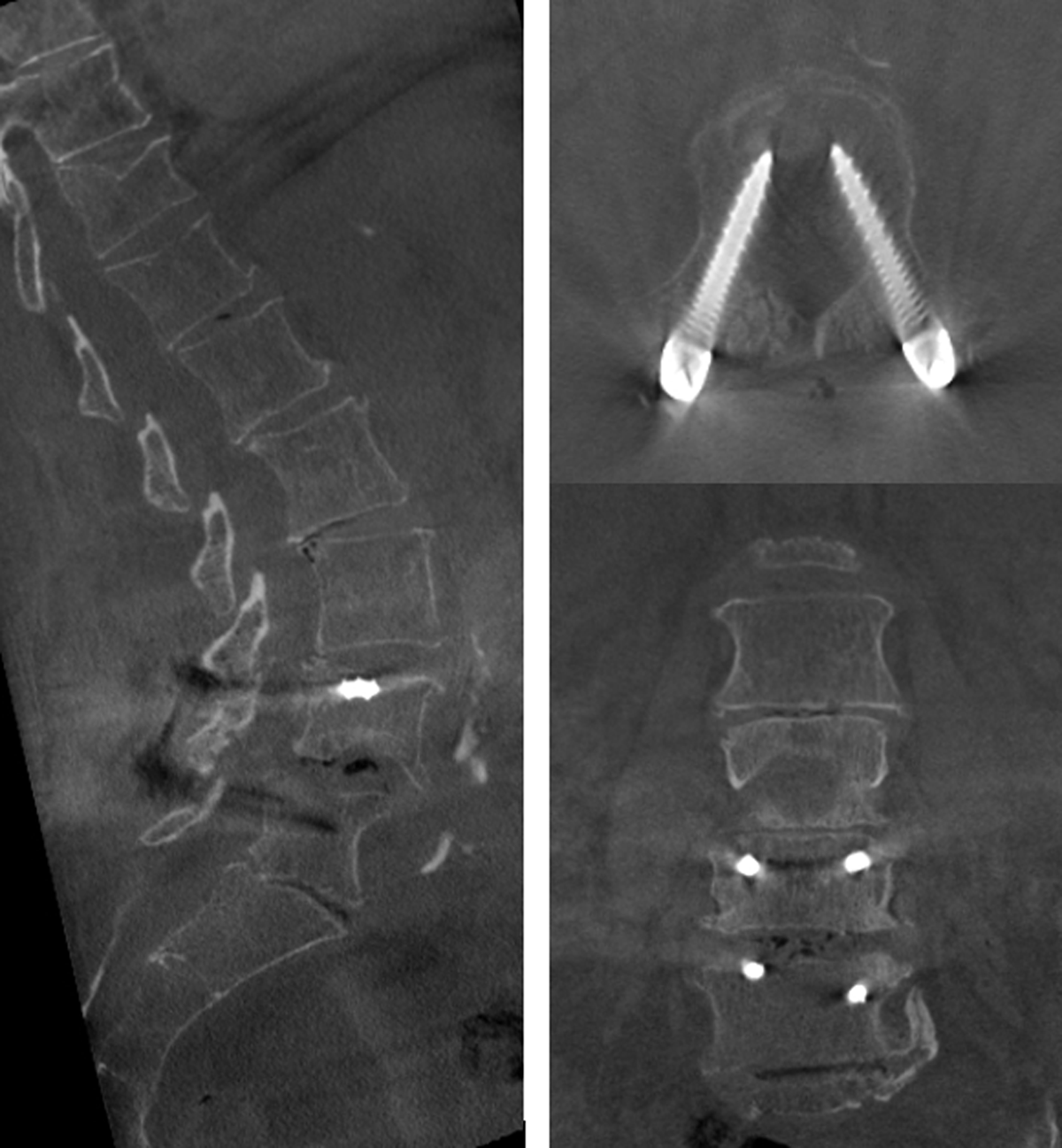
Figure 1
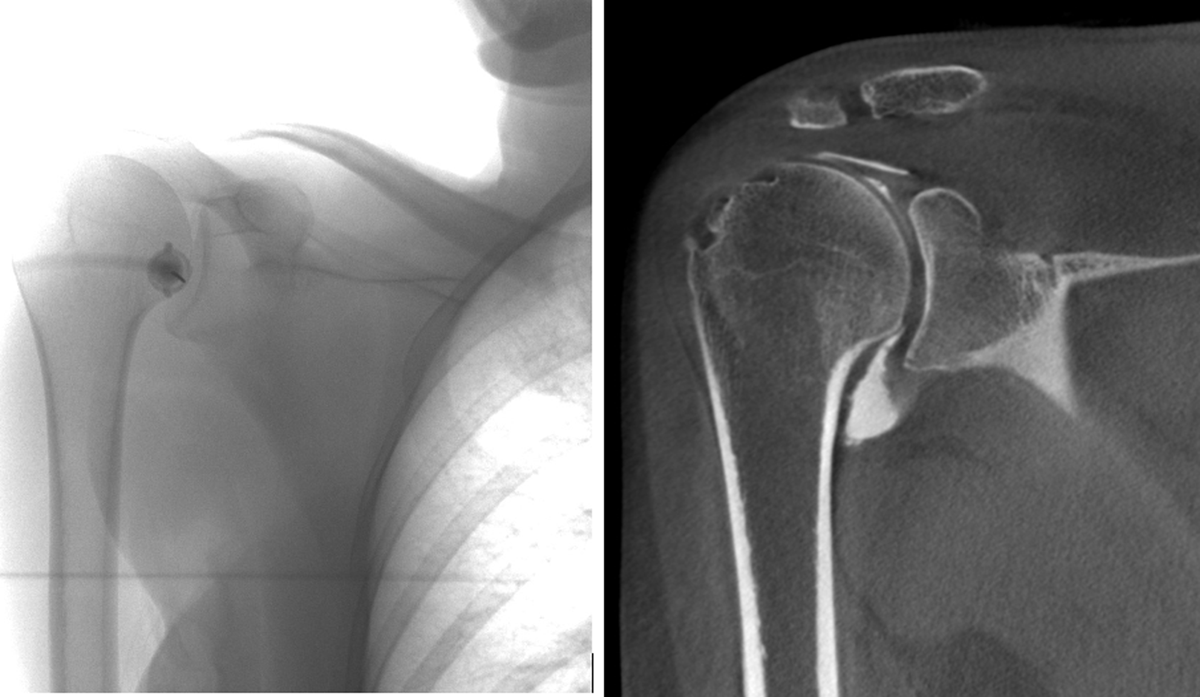
Figure 2
New techniques with image stitching make it now possible to scan a large FOV, up to 29 (x-y axis) × 56 cm (z-axis) and 17 × 62 cm. For example, the whole lumbar spine or a fracture of a large bone can be fully visualized, with a superior bone detail as compared to MDCT (Figure 3). Different combinations of small FOV and different dose settings make help minimizing dose exposure whilst imaging smaller bones and children.
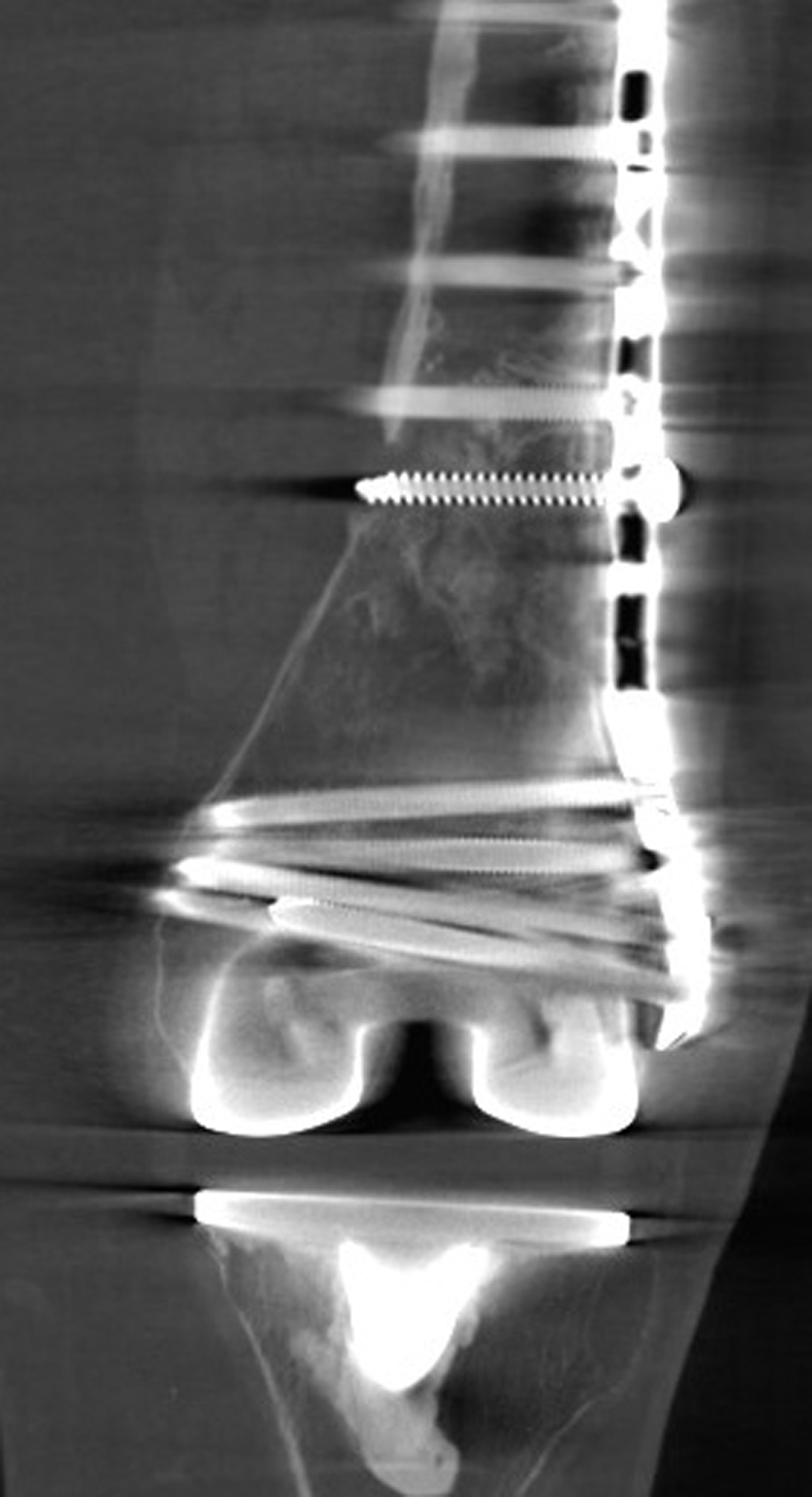
Figure 3
Very promising is the current development of dual energy CBCT for the detection of bone marrow edema. Prior studies showed Magnetic Resonance Imaging (MRI) to be the gold standard in detecting (radiographically occult) scaphoid fractures [9], with CBCT serving as an alternative in case of limited availability of MRI. With the addition of dual energy, CBCT will likely become a more accurate tool to detect these fractures, challenging MRI. Other important benefits of dual energy are better soft tissue visualization (when using low-voltage in the range of 20–40 kV), and reduction of beam hardening artifacts.
CBCT can also help predict the risk of vertebral fractures in osteoporosis. Trabecular bone structure is an important factor in bone strength, together with mineral content (assessed with dual energy X-ray absorptiometry, DEXA). Studies have shown CBCT to have a high correlation with micro-CT (the current gold standard) in quantifying the bone structure, with the limitation that these studies were performed on the radius [1011]. It is possible that new generation CBCT will further improve the accuracy of these measurements, especially when the lumbar spine or femur will be used as focus.
New data shows that the implementation of iterative reconstructions and artificial intelligence in high-end CBCT is a potential tool towards a further substantial dose reduction.
Competing Interests
The authors have no competing interests to declare.