

Figure 1
Axial T2-WI of the prostate in a 66-year-old man with PSA of 10 ng/ml. Far anteriorly and cranially on the left side in the transition zone of the prostate there is an ill-defined marked low-signal intensity area (white star) with irregular contour, suspicious for prostate cancer.
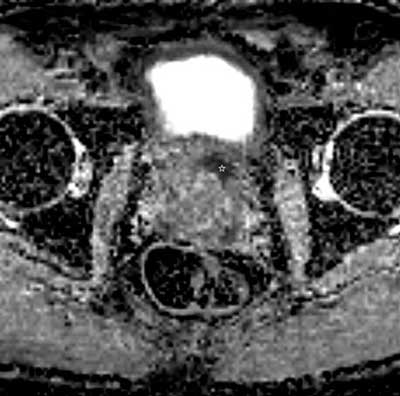
Figure 2
Axial ADC map of DWI in the same patient and at the same level as Figure 1. The lesion shows very low ADC value (white star) with corresponding very high signal intensity on the high-b-value images (not presented), which is suggestive of a high-grade prostate cancer. In the radiology report this lesion was scored PI-RADS 4, indicating that the likelihood of a clinically significant prostate cancer is high.
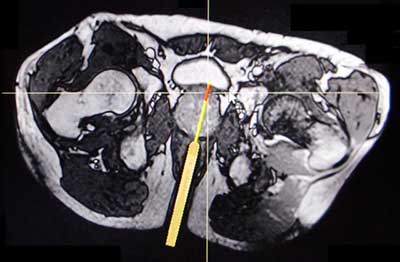
Figure 3
Axial T2-WI of in-bore MRI guided transrectal prostate biopsy in the same patient and at the same level as Figures 1 and 2. The patient initially underwent a systematic transrectal ultrasound guided prostate biopsy but the pathology result showed no malignancy. Because of the persistently rising PSA and the difficult location of the suspicious lesion, an in-bore MRI guided transrectal prostate biopsy was performed. The position of the transrectal needle guide (thick line) and the tru-cut biopsy needle (fine line) are demonstrated on the T2-WI and confirm that the suspicious lesion is sampled correctly. Two biopsy cores were taken, and the pathology result revealed Gleason 4 + 4 prostate cancer in both of them.