
Postpartum depression (PPD) is a significant mental health issue that affects a substantial number of new mothers globally. The prevalence of PPD varies widely, with estimates ranging from 10% to 70%, depending on socioeconomic factors, cultural contexts, and social support. In low- and middle-income countries, the prevalence can reach 19.2%, while it is around 12.9% in high-income countries. [1] This disparity highlights the influence of socio-environmental factors on PPD incidence. PPD negatively affects not only the mothers but also child development and family dynamics. Children of mothers with PPD are at risk for behavioural issues and cognitive delays. [2] Additionally, PPD may impair breastfeeding practices, leading to early cessation and negatively impacting infant health. [3,4] PPD's psychosocial consequences include maternal isolation, feelings of inadequacy, and the intensification of depressive symptoms. Social support plays a crucial role in reducing the incidence and severity of PPD. [5] Intervention strategies focused on counselling and social support programs have shown promise in mitigating PPD. [6] Furthermore, stressful life events and conditions such as preterm birth can increase PPD risk, with some studies indicating a prevalence of 70% among mothers of preterm infants. [7] PPD is often a dyadic phenomenon affecting both parents, and family-centred interventions are essential for addressing its broader impact. [8] Psychotherapy, including cognitive-behavioural therapy (CBT), and pharmacotherapy, such as SSRIs, have been found effective in treating PPD. [9] Increasing awareness and training healthcare providers to identify PPD can lead to improved outcomes. [10]
Depressive symptoms in postpartum women arise from a multifactorial aetiology involving hormonal, neurobiological, and psychosocial factors. The sharp decline in estrogen and progesterone following childbirth is associated with the onset of depressive symptoms in new mothers. [11] Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis and elevated cortisol levels have also been linked to stress and depressive symptoms in postpartum women. [12] Additionally, neuroactive steroids, such as allopregnanolone, and neuroinflammatory processes may disrupt neurotransmitter systems like serotonin and dopamine, contributing to mood disturbances. [13] Psychosocial stressors, such as life events or lack of social support, also increase vulnerability to PPD, underscoring the importance of a biopsychosocial model in understanding it. [14]
Inflammatory cytokines, such as IL-6, TNF-α, and CRP, play a key role in depressive symptoms by affecting neurotransmitter metabolism and neurogenesis. [15,16] Elevated pro-inflammatory cytokine levels have been observed in individuals with depression, which suggests a bidirectional relationship where inflammation contributes to depression, and depression, in turn, exacerbates inflammatory responses. [17,18] These cytokines may also reduce reward system responsiveness in the brain, leading to anhedonia, a core symptom of depression. [19,20] Anti-inflammatory treatments are being explored as adjunct therapies for depression, especially in individuals with elevated inflammation. [21,22]
Research has demonstrated a link between pro-inflammatory cytokines and PPD. Elevated levels of IL-6 and TNF-α during the postpartum period are correlated with increased depressive symptoms. [23,24] These cytokines may influence neurotransmitter regulation and neuroplasticity, leading to mood disturbances. Additionally, psychosocial stressors, such as physical trauma during childbirth, can trigger inflammatory responses, contributing to PPD. [25] Genetic factors may further modulate the inflammatory response, increasing the susceptibility to PPD. [25]
Despite increasing evidence linking inflammatory cytokines to PPD, the research presents several inconsistencies and gaps. Studies on the role of specific cytokines, such as IL-6 and TNF-α, show conflicting results, with some finding significant associations while others report no relationship. Furthermore, many studies lack large and diverse sample sizes, which limits the generalizability of their findings. Another challenge is the variation in cytokine measurement techniques and the timing of assessments across studies, making it difficult to draw definitive conclusions. Additionally, few studies consider the interplay between biological and psychosocial factors, such as stress and social support, that may influence both cytokine levels and depressive symptoms. This fragmented evidence underscores the need for a comprehensive synthesis of the available data to clarify the role of inflammatory cytokines in PPD and identify potential biomarkers for early detection and intervention.
The objective of this systematic review is to evaluate the relationship between inflammatory cytokines and depressive symptoms in postpartum women. By synthesising data from existing studies, this review aims to provide a clearer understanding of the role of cytokines in the pathophysiology of PPD. Specifically, this review aims to identify which cytokines, if any, are consistently associated with postpartum depressive symptoms and to highlight areas where further research is needed. This analysis will help inform future studies and potentially contribute to the development of targeted interventions for PPD.
This systematic review was conducted in accordance with the PRISMA 2020 guidelines. [26] A comprehensive literature search was performed in five electronic databases: PubMed, ScienceDirect, CINAHL, Web of Science, and Tripdatabase. The search included studies published in English up to September 2024. Keywords and medical subject headings (MeSH) related to “inflammatory cytokines”, “postpartum blues”, and “postpartum depressive symptoms” were used. The reference lists of included studies were also manually screened to identify additional relevant studies.
Studies were included if they examined the relationship between inflammatory cytokines and depressive symptoms in postpartum women. Eligible studies had to involve human participants, focus on postpartum women, and include assessments of both inflammatory cytokine levels and depressive symptoms. Exclusion criteria were non-English language articles, studies that did not measure both variables of interest, and studies involving non-postpartum populations.
Two reviewers independently extracted data, including study characteristics, participant demographics, types of cytokines measured, and assessments of depressive symptoms. Disagreements were resolved by discussion until a consensus was reached. The primary outcome was the association between cytokine levels and depressive symptoms.
The risk of bias in the included studies was evaluated using the Revised Risk of Bias Assessment Tool for Nonrandomized Studies of Interventions (RoBANS 2). [27] Domains assessed included comparability of target groups, selection, confounders, blinding of assessors, and outcome reporting.
The initial search identified a total of 1,308 articles across five electronic databases. After filtering based on original research article type, 42 articles were screened based on titles and abstracts. Of these, 13 articles were selected for full-text review. Following a full-text assessment, two studies were removed as duplicates, and one study was excluded because it lacked full-text access. [28] The nine (9) studies met the eligibility criteria and were included in this systematic review. The PRISMA flowchart illustrating this search process is shown in Figure 1.
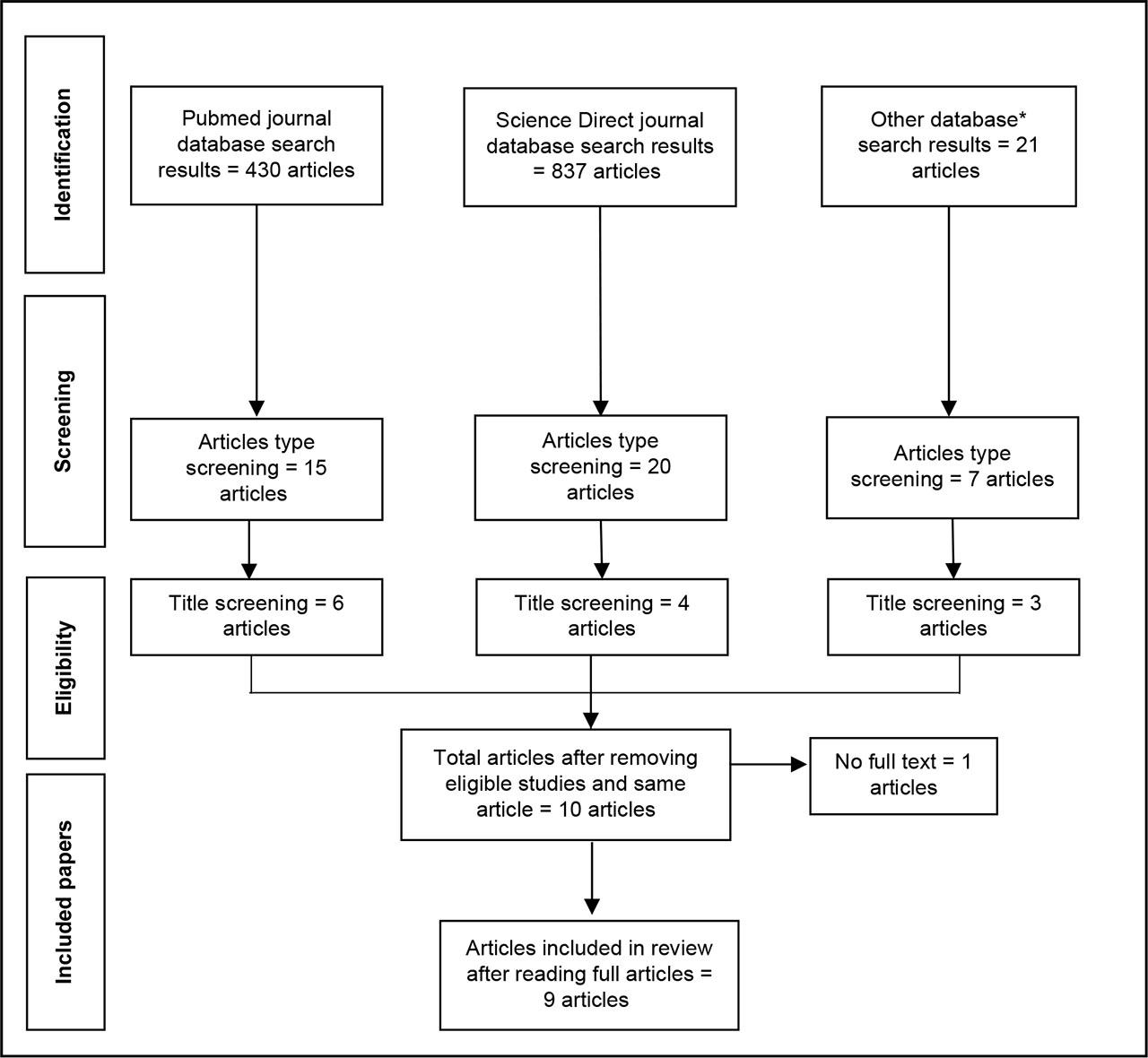
PRISMA flowchart.
The risk of bias assessment revealed variability in study quality. Using the Revised Risk of Bias Assessment Tool for Nonrandomized Studies of Interventions (RoBANS 2), three studies were classified as having a high risk of bias, primarily due to issues with selection bias and selective outcome reporting. Conversely, five studies were rated as having a low risk of bias, demonstrating robust methodologies and thorough reporting. Detailed risk of bias results are summarised in Table 1.
Risk of Bias Assessment using Revised Risk of Bias Assessment Tool for Nonrandomised Studies of Interventions (RoBANS 2).
| No. | Domain | Study Index Number | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
| 1. | Comparability of the target group | Low | High | Unclear | Unclear | Low | Low | Low | Low | Low |
| 2. | Target group selection | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| 3. | Confounders | Low | High | Low | Low | Low | Low | Unclear | Low | Low |
| 4. | Measurement of exposure | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| 5. | Blinding of assessors | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| 6. | Outcome assessment | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| 7. | Incomplete outcome data | Low | Low | Low | Low | Low | Low | Low | Unclear | Low |
| 8. | Selective outcome reporting | High | Low | High | High | Low | Low | Low | Low | Low |
| Overall results | Moderate | High | High | High | Low | Low | Low | Low | Low | |
The nine studies included a total of 888 postpartum women. Study designs varied, with seven cohort studies, one case-control study, and one cross-sectional study. The majority of studies (four) were conducted in the United States, while one study each came from Canada, Poland, Sweden, China, and Taiwan. The average age of participants ranged from 25 to 31 years. Depressive symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS) in five studies, the Centre for Epidemiologic Studies Depression Scale (CES-D) in two studies, and the Hamilton Depression Rating Scale (HDRS) in two studies.
Analysis of the data revealed that IL-1β was significantly elevated in postpartum women with depressive symptoms, supported by two studies, with one study having a low risk of bias and the other one having a high risk of bias. Inconsistent findings were observed for IL-6, with three studies supporting an association and three opposing it. IL-10 and TNF-α generally showed no significant association with depressive symptoms. Specifically, IL-10 had one supportive study and two opposing studies, whereas TNF-α was not significantly associated in any of the included studies. CRP levels showed no significant relationship with depressive symptoms, with one study supporting and three studies refuting the association. A summary of the included studies is presented in Table 2.
Summary of included studies.
| No. | Study details | Subject characteristics | Result |
|---|---|---|---|
| 1. |
|
| Levels of prenatal cytokines (IL-1, IL-5, IL-7, MPI-1α, GM-CSF, MCP, MIB) were not statistically different when participants were grouped as either low-high stress, yes-no fatigue, or yes-no depression. |
| 2. |
|
| Five cytokines were significantly elevated in women with postpartum depressive symptoms; TRANCE, HGF, IL-18, FGF-23, and CXCL1. |
| 3. |
|
| No significant relationships were found between inflammatory cytokines (hs-CRP, IFN-γ, TNF-α, IL-2, IL-6) and psychosocial measures. |
| 4. |
|
|
|
| 5. |
|
|
|
| 6. |
|
|
|
| 7. |
|
| The difference between IL-6 and IL-10 levels in women with and without depression was not statistically significant. |
| 8. |
|
| CRP levels were not significantly associated with HDRS score even after controlling for maternal BMI and total night sleep. |
| 9. |
|
| The serum levels of Hs-CRP and IL-6 after delivery in women with depression were significantly higher than in women without depression. |
CES-D: Center for Epidemiologic Study-Depression; CXCL1: C-X-C motif chemokine 1; EPDS: Edinburgh Postnatal Depression Scale; FGF-23: Fibroblast growth factor 23; HDRS: Hamilton Depression Rating Scale; HGF: Hepatocyte growth factor; IL: Interleukin; KYN: kynurenine; SERO: serotonin; TNF: Tumour Necrosis Factor; TRANCE: Tumor necrosis factor ligand superfamily member; TRY: Tryptophan; POMS: Profile of Mood States; PSS: Perceived Stress Scale.
This systematic review found an inconsistent relationship between inflammatory cytokines and depressive symptoms in postpartum women. IL-1β was significantly elevated in postpartum women with depressive symptoms in two studies, suggesting its potential as a biomarker for detecting depression in postpartum women. However, findings on IL-6 were mixed; three studies reported an association, while others did not. IL-10 and TNF-α generally showed no significant association with PPD. These results suggest that while IL-1β may be relevant, more research is required to clarify the roles of other cytokines.
The results align with previous research indicating the involvement of inflammatory cytokines in depressive disorders, but underscore the variability of findings. Similar to earlier studies, IL-1β emerged as a more consistent marker, while IL-6 demonstrated conflicting results [24 - Osborne et al., 2019; 31 - Cheng & Pickler, 2014]. These inconsistencies are likely due to differences in study designs, sample sizes, and cytokine measurement techniques. Prior research has also highlighted mixed results for IL-6, reflecting the need for standardised methodologies to assess its role in postpartum depression [23 - Dunn et al., 2015].
The potential link between cytokines and PPD may involve several biological pathways. Hormonal fluctuations after childbirth, particularly the sudden decline in estrogen and progesterone, can trigger immune responses and increase cytokine levels. [12,29] Elevated levels of IL-1β and IL-6 may interfere with the serotonin and dopamine neurotransmitter systems, leading to mood disturbances. [13,30] Additionally, dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis due to stress could enhance inflammation, exacerbating depressive symptoms. [14]
The included studies exhibited a range of strengths and weaknesses. A key strength was the use of validated depression scales like EPDS and CES-D, ensuring a reliable assessment of depressive symptoms. The potential for IL-1β to serve as a biomarker for postpartum depression could have significant clinical implications. If further validated, measuring IL-1β levels could help identify postpartum women at risk for developing depressive symptoms, facilitating early intervention. However, their clinical utility remains uncertain given the inconsistent findings on IL-6, IL-10, and TNF-α. Clinicians should continue to use comprehensive assessments of psychosocial factors, while cytokine measures could complement these in the future.
This review has several limitations. Many studies were limited by small sample sizes, which reduced the generalizability of their findings. The heterogeneity in cytokine measurement methods, as well as the timing of assessments, also contributed to inconsistent results. The risk of bias was moderate to high in some studies, further complicating the interpretation of the conclusions. Finally, the exclusion of non-English language studies may have omitted relevant research, reducing the scope of this review.
Future research should address the limitations identified in this review. Larger, more diverse sample sizes are necessary to improve the generalizability of findings. Additionally, studies should focus on longitudinal tracking of cytokine levels across the perinatal period to determine the timing of inflammatory responses in relation to depressive symptoms. Exploring the interaction between biological and psychosocial factors, such as stress, trauma, and social support, will provide a more comprehensive understanding of the appearance of depressive symptoms in postpartum women.
This systematic review highlights the potential role of IL-1β in postpartum depressive symptoms, while the evidence for IL-6, IL-10, and TNF-α remains inconclusive. Further high-quality studies are needed to clarify the relationship between inflammatory cytokines and postpartum depression and to explore their potential as biomarkers for clinical use.
IL-1β is significantly higher in postpartum women with depressive symptoms.
IL-2 and TNF-α are not significantly different between those groups.
The relationship between IL-6 levels and depressive symptoms in postpartum women is still inconsistent.
The relationship between IL-10 levels and depressive symptoms in postpartum women favours no significant association.
The relationship between CRP levels and depressive symptoms in postpartum women favours no significant association.