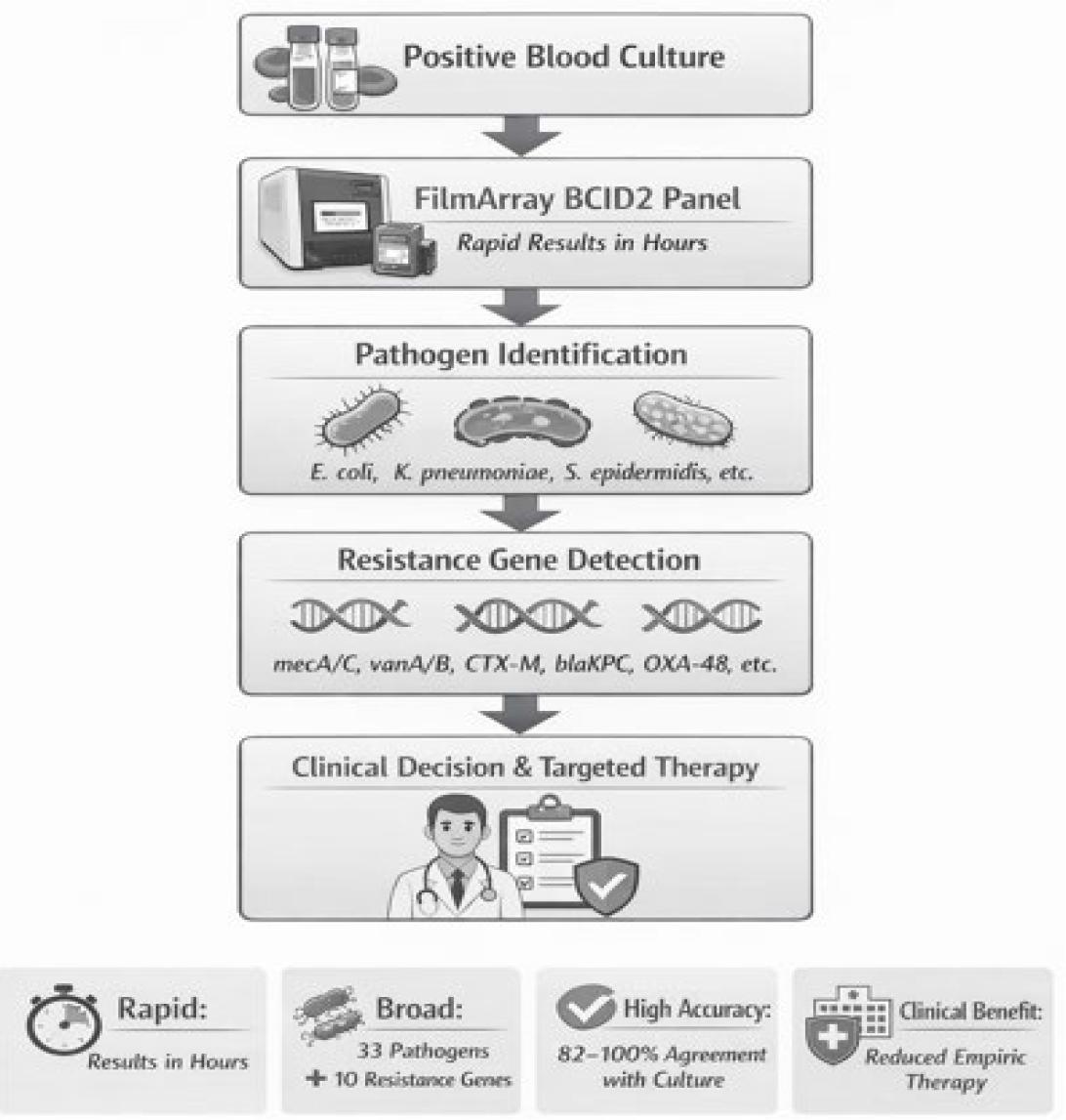
Bloodstream infections (BSIs) are systemic inflammatory responses triggered by the presence of microorganisms in the bloodstream (Viscoli 2016). BSIs are linked with high morbidity and mortality, particularly in intensive care unit (ICU) settings (Ferrer et al. 2014). Bacterial and fungal agents may cause BSIs, with commonly implicated pathogens including Fscherichia coli, Staphylococcus aureus, Coagulase-negative staphylococci (CoNS), Klebsiella pneumoniae, and Candida albicans, though prevalence varies by patient demographics and region (Holmes et al. 2025). Early and appropriate antimicrobial therapy is essential for optimal outcomes (Daneman et al. 2025). Accurate identification of blood isolates at the species level and determination of infection sources are critical for effective management (Seifert 2009). Blood culture remains the gold standard for pathogen identification and antimicrobial susceptibility determination in suspected BSIs, but its turnaround time is lengthy. Conventional blood cultures typically require 12–72 hours to yield a final result, and sensitivity may be reduced by prior antibiotic exposure or fastidious organisms (Opota et al. 2015). Recent advancements, such as matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) and nucleic acid-based methods, have significantly reduced the time to result. Molecular diagnostics can identify pathogens and resistance determinants within hours, allowing for more rapid targeted therapy and reduced empirical antibiotic usage (Trevino et al. 2017). Multiplex PCR panels such as BioFire® BCID2 have been evaluated in several studies and shown to achieve overall concordance rates of 82–97% with conventional culture, with particularly high performance for Gram-negative bacteremia (Kim et al. 2024; Kitagawa et al. 2025). The BioFire® BCID2 panel (bioMérieux, France) detects 33 pathogens and 10 resistance genes (Peri et al. 2021). This study aims to evaluate the clinical utility of BCID2 by comparing its diagnostic performance with conventional culture-based methods in positive blood culture samples.
This study was conducted using 50 blood culture samples obtained from the Ondokuz Mayıs University Faculty of Medicine Hospital between January 2023 and September 2025. Ethical approval for the study was obtained in 2025 with decision number 545. All 50 samples were derived exclusively from peripheral venous blood cultures. Catheter-tip cultures and catheter-drawn blood cultures were not included in the study. Furthermore, only the first blood culture set per patient was analyzed; repeat or follow-up blood culture sets from the same patient were excluded. This study design, therefore, does not allow assessment of contamination probability based on multiple concurrent culture sets, which is a recognized limitation for interpreting CoNS results. Blood culture samples accepted by the laboratory were loaded into the BD BACTEC™ blood culture system (Becton Dickinson, USA). Following a positive signal, the samples were subcultured onto BD Columbia Agar with 5% sheep blood and BD MacConkey Agar (MAC) (Becton Dickinson, USA). The inoculated plates were incubated at 36°C for 24 hours. Identification of the isolated microorganisms was performed using the VITEK® MS system (bioMérieux, France), and antimicrobial susceptibility testing was performed using the VITEK® 2 Compact automated system (bioMérieux, France). Simultaneously with subculturing after a positive signal was obtained in the blood culture system, the BCID2 test was performed during working hours, and the results were compared with culture results. The BCID2 panel test is a multiplex polymerase chain reaction (PCR)-based assay capable of detecting 33 pathogens and 10 antimicrobial resistance genes. The panel includes 15 Gram-negative bacteria (Acinetobacter calcoaceticus/baumannii complex, Bacteroides fragilis, Enterobacterales, Enterobacter cloacae complex, Escherichia coli, Klebsiella aerogenes, Klebsiella oxytoca, Klebsiella pneumoniae group, Proteus spp., Salmonella spp., Serratia marcescens, Haemophilus influenzae, Neisseria meningitidis, Pseudomonas aeruginosa, Stenotrophomonas maltophilia); 11 Gram-positive bacteria (Enterococcus faecalis, Enterococcus faecium, Listeria monocytogenes, Staphylococcus spp., Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus lugdunensis, Strepococcus spp., Streptococcus agalactiae, Streptococcus pneumoniae, Streptococcus pyogenes; seven yeast species (Candida albicans, Candida auris, Candida glabrata, Candida krusei, Candida parapsilosis, Candida tropicalis, Cryptococcus neoformans/gattii); and 10 antimicrobial resistance genes (mecA/C and MREJ for methicillin-resistant Staphylococcus aureus (MRSA), vanA/B for vancomycin resistance, CTX-M for extended-spectrum ß-lactamase (ESBL), blaKPC for Klebsiella pneumoniae carbapenemase (KPC), blaIMP for imipenemase (IMP), blaOXA-48 for oxacillinase-48 (OXA-48), blaNDM for New Delhi metallo-ß-lactamase (NDM), blaVIM for Verona integron-encoded metallo-ß-lactamase (VIM), and mcr-1 for mobile colistin resistance (mcr-1)). Resistance genes were reported only when the corresponding potential causative microorganism was also detected in the sample. In addition, conventional PCR was performed for microorganisms grown in culture to confirm the presence of resistance genes detected by the BCID2 panel using appropriate primer sequences (Poirel et al. 2011). Primer sequences used for conventional PCR validation of the BCID2 panel are presented in Table I.
Primer sequences used in this study.
| GenE | Primer | Sequence (5’→3’) | Expected amplicon size (bp) |
|---|---|---|---|
| VIM | VIM-F | GATGGTGTTTGGTCGCATA | 390 |
| VIM-R | CGAATGCGCAGCACCAG | ||
| NDM | NDM-F | GCA GCT TGT CGG CCA TGC GGG C | 782 |
| NDM-R | GGT CGC GAA GCT GAG CAC CGC | ||
| KPC | KPC-F | TGT CAC TGT ATC GCC GTC | 900 |
| KPC-R | CTC AGT GCT CTA CAG AAA ACC | ||
| IMP | IMP-F | GGAATAGAGTGCTTAAYTCC | 232 |
| IMP-R | GGTTTAAYAACAAACACACC | ||
| OXA-48 | OXA-48-F | GCGTGGTTAAGGATGAACAC | 438 |
| OXA-48-R | CATCAAGTTCAACCCAACCG | ||
| mecC | mecC-F | GAAAAAAAGGCTTAGAACGCCTC | 138 |
| mecC-R | GAAGATCTTTTCCGTTTTCAGC | ||
| mecA | mecA-F | GTAGAAATGACTGAACGTCCGATAA | 310 |
| mecA-R | CCA ATT CCA CAT TGT TTC GGT CTA A |
This table lists the PCR primer sequences used to detect pathogens and resistance genes in positive blood cultures, along with the expected amplicon sizes (bp) for each primer pair. Primers are shown in the 5’→3’ direction. The table summarizes the target resistance genes (VIM, NDM, KPC, IMP, OXA-48, mecA, mecC), their corresponding forward (F) and reverse (R) primers, and the expected DNA fragment sizes.
A total of 50 positive blood culture samples were analyzed using the BioFire® FilmArray BCID2 panel. At least one bacterial pathogen was detected in 47 of 50 samples (94%). The most frequently identified pathogens by the BCID2 panel were A. calcoaceticus/baumannii complex, K. pneumoniae, S. epidermidis, E. coli, and E. faecalis, respectively. While a single pathogen was detected in some samples, two or more microorganisms were identified concurrently in others. In this regard, BCID2 detected polymicrobial results in 20 cases (40%). Detailed microorganism combinations detected in polymicrobial samples and their corresponding blood culture results are presented in Table II.
Comparison of polymicrobial microorganisms detected by the BioFire® FilmArray BCID2 Panel and conventional blood culture results.
| Sample No. | BCID2 Results | Blood culture result | Clinical interpretation |
|---|---|---|---|
| 1, 2, 3, 14 | Staphylococcus epidermidis + Acinetobacter calcoaceticus/baumannii complex | Acinetobacter baumannii | Possible CoNS contamination |
| 4, 5 | Klebsiella pneumoniae group + Pseudomonas aeruginosa | Klebsiella pneumoniae or Pseudomonas aeruginosa | Predominant organism in culture |
| 6, 7, 10, 13, 15, 18 | Klebsiella pneumoniae group + Enterococcus faecalis + Staphylococcus spp. | Klebsiella pneumoniae | Possible polymicrobial BSI |
| 8, 12, 16 | Eschrichia coli + Klebsiella pneumoniae group + Enterococcus faecalis + Streptococcus spp. | No growth | Fastidious organisms / PCR sensitivity |
| 9 | Enterococcus faecalis + Proteus spp. | Enterococcus faecalis + Proteus mirabilis | Complete concordance |
| 11, 17 | Staphylococcus spp. + Pseudomonas aeruginosa | Pseudomonas aeruginosa | Possible CoNS contamination |
| 19 | Enterococcus faecalis + Staphylococcus spp. | Enterococcus faecalis | Predominant organism in culture |
| 20 | Eschrichia coli + Klebsiella pneumoniae group | Escherichia coli | Predominant organism in culture |
Overall, BCID2 detected a broader range of microorganisms than conventional culture in most polymicrobial samples, whereas culture frequently yielded only a single dominant organism or no growth. The comparison of microorganisms detected by the BCID2 panel with blood culture results, including diagnostic performance measures, is presented in Table 3.
Comparison of BCID2 and blood culture results with concordance and diagnostic performance measures.
| Microorganism | BCID2-positive samples (n) | Growth in blood culture (n) | Concordance rate (%) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|
| Acinetobacter calcoaceticus/baumannii complex | 14 | 9 | 64 | 100 | 87.8 | 64.3 | 100 |
| Klebsiella pneumoniae | 13 | 11 | 85 | 100 | 94.9 | 84.6 | 100 |
| Staphylococus epidermidis | 11 | 1 | 9 | 100 | 79.6 | 9.1 | 100 |
| Escherichia coli | 5 | 5 | 100 | 100 | 100 | 100 | 100 |
| Enterococcus faecalis | 5 | 1 | 20 | 100 | 91.8 | 20 | 100 |
| Pseudomonas aeruginosa | 4 | 4 | 100 | 100 | 100 | 100 | 100 |
Note: The concordance rate was calculated as follows: (BCID2-positive and culture-positive cases / total BCID2-positive cases) × 100. Diagnostic performance metrics, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), were determined using conventional blood culture as the reference standard. These results should be interpreted with caution, taking into account the inherent limitations of culture-based methods and the potential for clinical contamination.
Among the six organisms presented, E. coli and P. aeruginosa demonstrated 100% concordance between BCID2 and blood culture. K. pneumoniae showed an 85% concordance rate. In contrast, S. epidermidis and E. faecalis exhibited low concordance rates (9% and 20%, respectively), which likely reflect their propensity for skin contamination rather than true bloodstream infection. A strong correlation was observed between detected resistance genes and phenotypic susceptibility profiles. All K. pneumoniae isolates harboring carbapenemase genes (KPC, NDM, or OXA-48-like) were phenotypically resistant to carbapenems, whereas isolates without detected carbapenemase genes were susceptible (100%). The overall concordance rate between BCID2 and culture results was 82%.
Early and appropriate antimicrobial therapy is a decisive factor in the survival of patients with bloodstream infections (Briggs et al. 2021). Blood culture samples typically yield a positive signal within 12.8–17 hours (Pardo et al 2014). Although routine blood culture allows direct observation of pathogen growth, it is time-consuming due to the required incubation period of approximately 18–24 hours and subsequent sample processing steps. Furthermore, the clinical sensitivity is lower for certain fastidious pathogens that are difficult to grow in culture (Zhao et al. 2025). For these reasons, reporting of routine blood culture results often takes 48–72 hours (Serapide et al. 2025). In contrast, PCR-based methods enable pathogen identification within hours, allowing early initiation of targeted therapy and potentially shortening hospital length of stay, thus providing a significant time advantage (Fultariya et al. 2025). Several studies have also demonstrated that early detection of the causative agent significantly reduces treatment costs (Beekmann et al. 2003). This is consistent with published evaluations of multiplex PCR panels. Kim et al. (2024) reported a concordance rate of 96.8% across 155 positive blood cultures using a comparable multiplex PCR system, with particularly high sensitivity for Gram-negative organisms. Kitagawa et al. (2025) demonstrated that multiplex PCR testing led to earlier antibiotic de-escalation and reduced unnecessary broad-spectrum therapy. Serapide et al. (2025) similarly reported high sensitivity for BCID2 in detecting carbapenem-resistant organisms. The slightly lower concordance in our cohort may be partly attributable to the inclusion of CoNS as BCID2-positive results not confirmed by culture, as discussed below. A strong correlation was observed between the presence of antibiotic resistance genes and phenotypic susceptibility results. This finding is consistent with Kim et al. (2024), who reported a resistance gene concordance rate of 96.8%. The ability to detect CTX-M, OXA-48, NDM, KPC, VIM, IMP, vanA/B, and mecA/C genes enables the prediction of potential resistance profiles within one hour of a positive blood culture signal. For instance, all K. pneumoniae isolates harboring carbapenemase genes were phenotypically resistant to carbapenems, whereas isolates without detected carbapenemase genes were susceptible (100%). These results suggest that BCID2 can guide early and appropriate antimicrobial therapy, particularly for preventing unnecessary broad-spectrum antibiotic use in ICU patients (Elzi et al. 2012; Peri et al. 2021). CoNS, particularly S. epidermidis, pose significant challenges in clinical management, as they may be detected in blood cultures as both true pathogens and common contaminants (Vázquez et al. 2013; Banerjee et al. 2015). In our study, although culture positivity for S. epidermidis was low (9%), the high BCID2 detection rate (11 samples) suggests that most of these results likely represent contamination rather than true bacteremia. Importantly, all 50 samples in this study were obtained from a single peripheral blood culture set per patient; no repeat or paired blood culture sets were available, and no catheter-tip cultures were included. In clinical practice, the diagnosis of true CoNS bacteremia typically requires growth in at least two separate blood culture sets drawn from different sites (Elzi et al. 2012). The absence of this information in the present study means that BCID2-positive CoNS results cannot be reliably distinguished from contamination. Clinicians should therefore interpret BCID2 CoNS detections with considerable caution, particularly in the absence of clinical signs of infection. The high mecA/C gene detection rate (91%) in these samples may nonetheless provide useful antimicrobial stewardship information when the clinical context supports true infection. The detection of microorganisms such as E. coli, K. pneumoniae, A. baumannii, and Staphylococcus spp. by PCR in culture-negative samples may reflect higher analytical sensitivity of PCR compared to blood culture (Zheng et al. 2021) or, alternatively, the detection of non-viable organisms in patients who had received prior antibiotic therapy. Without clinical correlation data, these results cannot be definitively interpreted. This study has several important limitations that must be considered when interpreting its findings. First, the study was conducted at a single center with a limited sample size of 50 specimens, which substantially restricts the generalizability of the results. The findings should therefore be regarded as preliminary and hypothesis-generating rather than definitive. Second, all samples were obtained from a single peripheral venous blood culture set per patient. No repeat or paired blood culture sets were collected, and catheter-tip cultures or catheter-drawn samples were not included. This is a critical limitation for interpreting CoNS results, as standard clinical criteria for true CoNS bacteremia require growth in at least two separate culture sets. Without this information, differentiation between true bloodstream infection and contamination—particularly for S. epidermidis and E. faecalis—was not possible. Third, no clinical correlation data were available. Patient-level information, such as clinical signs of infection, inflammatory markers, underlying conditions, prior antibiotic use, and catheter status, was not accessible for this analysis. This absence of clinical data further limits the ability to classify BCID2-positive results as true infections or contaminants. Fourth, while diagnostic performance metrics are provided in Table III using culture as a reference, these values should be interpreted cautiously given the small sample size and the absence of a gold-standard clinical reference in cases of culture-negative PCR positivity. Future studies should include these metrics to allow meaningful comparison with published data. Fifth, the BCID2 panel is inherently limited to the 33 pathogens and 10 resistance genes it targets; organisms outside the panel cannot be detected. Finally, the direct impact of BCID2 on clinical outcomes, including mortality, hospital length of stay, and antimicrobial stewardship decisions, was not evaluated. Future multicenter, prospective studies with larger cohorts, paired blood culture sets, and access to detailed clinical data are needed to more rigorously define the role of BCID2 in routine clinical practice. In conclusion, the BCID2 panel demonstrated rapid and generally reliable detection of bloodstream pathogens and resistance genes, with particularly strong performance for key gram-negative organisms. However, given the small sample size, single-center design, and absence of clinical correlation and repeat blood culture data, conclusions must be drawn with caution. The notably low culture concordance for CoNS underscores the importance of integrating BCID2 results with clinical findings and standard microbiological methods. The panel may serve as a valuable complementary tool to conventional diagnostics, but should not replace them.