
Cystic fibrosis (CF) is a genetic disorder caused by pathogenic variants in the CF transmembrane conductance regulator (CFTR) gene, which encodes a chloride channel involved in epithelial ion transport. This leads to the production of abnormally thick, sticky mucus that impairs respiratory and digestive function (Care for people with cystic fibrosis 2019). In the lungs, excess mucus forms plaques and plugs that create sites for chronic airway infections, leading to recurrent pulmonary exacerbations (PEx) and impaired air flow (Worlitzsch et al. 2002; Kesimer et al. 2017). These infections trigger an excessive and ineffective inflammatory response, resulting in bronchiectasis (Chalmers et al. 2017). In Poland, the incidence of CF is approximately 1 in 5,000 births, with 70–80 new cases each year (Sands et al. 2021).
Patients with CF are highly susceptible to respiratory infections due to the accumulation of thick, sticky mucus in the lungs. This mucus provides an ideal environment for bacterial growth, making it difficult for the body to clear infections. Chronic bacterial infections, along with recurrent PEx, inevitably lead to progressive lung damage. In patients with CF, life expectancy and quality of life are primarily determined by the degree of respiratory function. Respiratory disease remains the leading cause of death, with nearly 95% of CF-related mortality attributed to respiratory failure due to progressive lung damage induced by chronic infections (Lyczak et al. 2002).
The treatment of chronic bronchopulmonary disease in patients with CF includes daily physiotherapy, medications to improve mucociliary clearance, and antibiotics (systemic during PEx and nebulized for eradication or chronic treatment) to slow disease progression and prolong life expectancy. Preventing infections is critical, especially those caused by bacteria resistant to commonly used antibiotics (Smyth et al. 2014). The presence of drug-resistant bacteria complicates treatment and requires higher antibiotic doses due to increased drug clearance and poor bronchial penetration. Despite eradication efforts, chronic infections with Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus (MRSA) frequently develop, often necessitating intravenous antibiotic therapy for approximately 14 days, or longer in severe cases. The treatment of PEx aims to improve clinical symptoms, normalize inflammatory markers, and restore spirometry parameters to baseline levels (Smyth et al. 2014).
The increasing multidrug resistance (MDR) among bacteria reduces the effectiveness of routinely used antibiotics, worsening the prognosis of CF patients. Currently, there are no epidemiological data on infections in Polish patients with CF, including information on drug susceptibility to new antibiotics. Understanding bacterial susceptibility and resistance mechanisms is crucial for selecting effective treatment and optimizing antibiotic therapy. Since routine susceptibility testing does not include newer antibiotics, these agents are rarely added to hospital formularies and are not widely used. On the other hand, data on microbial susceptibility can quickly become outdated and should be regularly updated. Such information is essential for guiding appropriate antimicrobial therapy, revising hospital formularies or regional guidelines, and identifying new, more effective treatment options for CF patients to improve their quality of life.
This study aimed to investigate the current etiology and epidemiology of bacterial infections in Polish patients with CF. Specifically, it sought to determine the in vitro antimicrobial susceptibility of strains isolated from the respiratory tract to commonly used antibacterial drugs to identify key needs in CF antibiotic therapy.
The study was conducted at three sites providing routine care for patients with CF in Poland, including two adult centers and one pediatric center. Data were collected from August 1, 2022 (first patient visit) to July 20, 2023 (last patient visit). The study population included both children and adults with CF, with no prior assumptions as to the size of each group.
The inclusion criteria comprised male and female patients, both children and adults, with a confirmed diagnosis of CF based on sweat chloride test (≥60 mmol/l) and/or genetic testing. Eligible patients were those who routinely provided respiratory specimens (i.e. induced or spontaneous sputum or bronchoalveolar lavage [BAL]) collected for microbiological testing during medical visits. Additionally, each participant, or their legally authorized representative, parent(s), or legal guardian, was required to provide a personally signed and dated informed consent form or assent, indicating that they had been informed of all relevant aspects of the study. Patients who did not provide signed informed consent or assent were excluded from participation.
Written informed consent was obtained from each subject before enrollment and before the initiation of any study procedures. The study design, objectives, and duration were explained, and participants were informed of their right to withdraw from the study at any time and for any reason.
The final protocol, any amendments, and informed consent documents were reviewed and approved by the Institutional Review Board and/or the Independent Ethics Committee of each participating site (Resolution 72/2021 of the Bioethics Committee at the Institute of Tuberculosis and Lung Diseases in Warsaw, 13.01.2022). The study was conducted in accordance with legal and regulatory requirements, and its scientific purpose, value, and rigor were consistent with generally accepted research practices.
The primary objective of this noninterventional, prospective observational trial was to identify bacterial strains isolated from the respiratory tracts of patients with CF and to determine their in vitro antimicrobial susceptibility to 17 antibacterial drugs. Secondary objectives were as follows: 1) to investigate the current etiology and epidemiology of bacterial infections through microbiological analysis of samples collected from CF patients in Poland; 2) to identify and compare microbiological data collected during PEx visits and routine or control visits; and 3) to analyze the resistance patterns of pathogens responsible for infections in this patient population.
The study protocol and collected data are presented in Figure 1. During the first visit, patients could undergo additional examinations at the discretion of the investigator; however, these procedures were not mandatory for study participation. For subsequent visits by the same patient, the presence of a clinical indication for sample collection was the sole criterion for continued participation.
Study protocol.
BAL = bronchoalveolar lavage, MIC = minimum inhibitory concentration
Visit two, and any additional follow-up visits for the same patient could occur within 12 months of the study duration as outpatient or hospital visits, and could be scheduled for the management of PEx or as control visits following antibiotic therapy. The diagnosis of PEx was based on the Fuchs criteria (Naseem et al. 2024).
Demographic data were summarized for the whole population. Additionally, the following clinical characteristics were collected: forced expiratory volume in 1 second (FEV1) as a numerical variable (% predicted value), time since CF diagnosis (in years), and frequency of PEx.
The primary endpoint was the minimum inhibitory concentration (MIC) and also MIC90 of tested antibiotics. Secondary endpoints included: 1) identification of bacterial species isolated from the respiratory tract of CF patients; 2) percentage of strains susceptible or resistant to the tested antibiotics; 3) comparison of microbiological and demographic results collected during PEx visits and during planned/control visits; and 4) resistance pattern of the isolated strains.
Microbiological material obtained from CF patients was used to identify bacterial strains and assess antibiotic susceptibility. Samples were routinely collected during medical visits, including those for PEx management or control visits following antibiotic therapy. Multiple samples from the same patient were allowed during the study period. Sputum samples (induced or spontaneous) or BAL samples were collected for local diagnostic and treatment purposes, with isolated bacteria subsequently sent to the central laboratory for further analysis. If more than one strain of a given species was cultured from a sample, all strains identified as pathogenic were included in the analysis.
Bacterial strains were identified using routine methods applied in local laboratories. Samples were cultured on general and selective media. Identification of the grown isolates was performed using the VITEK 2 ID automated system (bioMérieux, France). The general requirement was that all microbiological analyses were carried out in accordance with European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. MIC measurement and susceptibility tests were performed using standardized methods in the local or central microbiology laboratory. MIC interpretation followed the EUCAST breakpoints version 12.0. Susceptibility testing included amikacin, cefepime, ceftaroline, ceftazidime, ceftazidime/avibactam, ciprofloxacin, clindamycin, colistin, co-trimoxazole, imipenem, levofloxacin, linezolid, meropenem, piperacillin/tazobactam, tigecycline, tobramycin, and vancomycin.
Resistance mechanisms such as MRSA, extended-spectrum beta-lactamase (ESBL), carbapenemases (class A: Klebsiella pneumoniae carbapenemase, New Delhi metallo-β-lactamase, class D: OXA-48), and Haemophilus influenzae types in pediatric patients were assessed using routine methods by the local microbiology laboratory. All isolates were categorized as MDR, extensively drug-resistant (XDR), or pandrug-resistant (PDR), where MDR refers to resistance to at least one agent in three or more antimicrobial categories, XDR indicates resistance to at least one agent in all but two or fewer categories (i.e., susceptible to only one or two), and PDR denotes non-susceptibility to all agents in all antimicrobial categories (Magiorakos et al. 2011).
The physiological upper respiratory tract is defined as a community of microorganisms naturally inhabiting this anatomical niche, playing a protective role by preventing colonization by pathogenic species (Davis 1996).
Since no formal hypothesis was tested in the study and all analyses were descriptive, the sample size was not estimated. Data were analyzed using standard descriptive statistics, including the number of samples or patients, mean, standard deviation, upper and lower quartiles, minimum, median, and maximum. Frequency tables were used for categorical variables, and the number of cases with missing data was reported when relevant. The level of statistical significance was set at 0.05. 95% confidence intervals for proportions were calculated using the Wilson method with Yates continuity correction (when applicable) as implemented in the prop.test function of the R statistical software.
During the study, 179 patients were screened, with no cases of screening failure, failure to meet the inclusion criteria, or refusal to sign an informed consent form. Participants included 62 children and 117 adults. All patients completed the study.
The mean age of the total population was 22.8 years (median, 22.0; range, 4.0–62.0). In adult patients, the mean age was 28.8 years (median, 27.0; range, 18.0–62.0). In pediatric patients, the mean age was 11.6 years (median, 12.5; range, 4.0–17.0). Women comprised 64.8% of the total population, with 62.9% in children and 65.8% in adults. The mean body mass index (BMI) was 18.1 kg/m2 (range, 13.2-26.9) in children and 21.5 kg/m2 (range, 15.2–37.9) in adults, with similar medians (17.7 kg/m2 and 21.0 kg/m2, respectively). Among adults, 66.7% had a normal weight, 19.8% were underweight, 9.9% were overweight, and 3.6% were obese.
Participants attended a total of 282 visits: 121 visits by children and 161 visits by adults. Of all visits, 213 (75.5%) were planned, with 91 (75.2%) in the pediatric group and 122 (75.8%) in the adult group. PEx visits accounted for 69 visits (24.5%), with 30 visits (24.8%) in the pediatric group and 39 visits (24.2%) in the adult group. No control visits after antibiotic therapy were reported. The detailed characteristics of visits are presented in Table I.
Characteristics of visits.
| Overall, n = 179 | Children, n = 62 | Adult, n = 117 | |
|---|---|---|---|
| Total number of patients | 179 | 62 | 117 |
| Total number of visits | 282 | 121 | 161 |
| Visit type | |||
| Planned | 213 (75.5%) | 91 (75.2%) | 122 (75.8%) |
| PEx | 69 (24.5%) | 30 (24.8%) | 39 (24.2%) |
| Control visit after antibiotic therapy | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Collected samples | n = 282 | n = 121 | n = 161 |
| Not analyzed | 11 (3.9%) | 3 (2.5%) | 8 (5.0%) |
| Microbiologically analyzed | 271 (96.1%) | 118 (97.5%) | 153 (95.0%) |
| Sample type | |||
| Spontaneous sputum | 237 (87.5%) | 116 (98.3%) | 121 (79.1%) |
| Induced sputum | 9 (3.3%) | 0 (0.0%) | 9 (5.9%) |
| BAL | 25 (9.2%) | 2 (1.7%) | 23 (15.0%) |
BAL – bronchoalveolar lavage, PEx – pulmonary exacerbations
The median time since CF diagnosis in the overall population was 16.9 years (range, 6 months – 51.9 years). For children, it was 11.8 years (range, 1.3–17.7 years), while for adults, it was 22.3 years (range, 6 months – 51.9 years).
FEV1 measurements were obtained for 115 individuals, including 59 children and 56 adults. The median predicted FEV1% was 91.0% in pediatric patients (range, 43.0–126.0) and 66.0% in adults (range, 23.0–120.0).
The median frequency of PEx was 4 (range, 0–8) in children and 2 (range, 0–14) in adults. The incidence of PEx in children was 3-fold higher than in adults (33.9/100 patient-years vs. 11.1/100 patient-years, respectively).
Antibiotic therapy within 12 months prior to the first visit was used in 144 subjects, including 62 children and 82 adults. The mean duration of antibiotic therapy was 80.5 days (median, 39.0 days; range, 0.0–365.0 days). The mean duration of antibiotic therapy was 147.8 days (median, 70.0 days; range, 0.0–365.0 days) in children and 29.6 days (median, 24.0 days; range, 0.0-126.0 days) in adults.
A total of 81 patients received CFTR modulators during the follow-up, including 30 children and 51 adults. These patients attended 119 visits in total, and PEx were reported in 21 individuals during these visits.
Although all patients were eligible with at least one visit, only those with ≥2 visits (n=60) could be included in the analysis of antibiotic therapy during study participation, PEx, and comparisons between PEx and planned or control visits. Among patients who attended at least two visits, 42 (75%) experienced a mean of 1.4 exacerbations (median, 1.0; range, 0.0–6.0). Of these patients, 21 (35%) had one exacerbation, and 21 (35%) had more than 1. In 18 patients (30%, n = 18), no exacerbations were reported. The overall incidence of exacerbations was 340.9 per 100 person-years. It was higher in the group aged <18 years (416.7 per 100 person-years) and lower in the group aged ≥18 years (276.9). There was a trend for a decreasing incidence of exacerbations with increasing BMI. In underweight patients (n = 26), the incidence was 453.4 per 100 person-years, compared with 278.0 in normal-weight patients (n = 26) and 221.4 in overweight patients (n = 6).
A total of 282 microbiological samples were collected (121 from children and 161 from adults). The detailed analysis included only samples with cultured strains, totaling 271 (96.1%), of which 118 (97.5%) were from children and 153 (95.0%) from adults. The remaining 11 samples did not yield any cultured strains and were therefore excluded from further analysis. These samples were collected from 178 patients: 61 children and 117 adults. Most samples were spontaneous sputum (237; 87.5% of the overall), including 116 (98.3%) from children and 121 (79.1%) from adults. BAL samples accounted for 15% of adult samples (n = 23) and only 1.7% of pediatric samples (n = 2). Induced sputum samples were collected only from adults (9 samples, 5.9%).
Detailed data on the frequency of bacterial strain isolation are presented in Table II. The most commonly isolated strain in the study population was S. aureus, found in 177 samples (65.3%) and identified in 129 patients (72.5%). In children, S. aureus was detected in 73 samples (61.9%), accounting for 75.4% of the pediatric population. In adults, it was found in 104 samples (68.0%), representing 70.9% of the adult population. MRSA was identified in 6.8% of S. aureus strains (12 samples overall) and was most common in samples from adults (11 cases, 7.2%).
Identification of bacteria strains isolated from the respiratory tract of patients with CF.
| Bacterial strain | Overall | Children | Adult |
|---|---|---|---|
| Samples | Samples | Samples | |
| Staphylococcus aureus (total) | 177 (65.3%) | 73 (61.9%) | 104 (68.0%) |
| Staphylococcus aureus (MRSA) | 12 (4.4%) | 1 (0.8%) | 11 (7.2%) |
| Pseudomonas aeruginosa | 107 (39.5%) | 28 (23.7%) | 79 (51.6%) |
| Physiological upper respiratory tract flora | 37 (13.7%) | 27 (22.9%) | 10 (6.5%) |
| Stenotrophomonas maltophilia | 15 (5.5%) | 8 (6.8%) | 7 (4.6%) |
| Achromobacter xylosoxidans | 13 (4.8%) | 1 (0.8%) | 12 (7.8%) |
| Haemophilus influenzae | 9 (3.3%) | 2 (1.7%) | 7 (4.6%) |
| Klebsiella spp. | 8 (3.0%) | 1 (0.8%) | 7 (4.6%) |
| Escherichia coli | 8 (3.0%) | 1 (0.8%) | 7 (4.6%) |
| Burkholderia spp. | 6 (2.2%) | - | 6 (3.9%) |
| Enterobacter cloacae | 6 (2.2%) | 2 (1.7%) | 4 (2.6%) |
| Pseudomonas spp. | 6 (2.2%) | 1 (0.8%) | 5 (3.3%) |
| Proteus mirabilis | 6 (2.2%) | - | 6 (3.9%) |
| Serratia spp. | 4 (1.5%) | - | 4 (2.6%) |
| Morganella morganii | 3 (1.1%) | - | 3 (2.0%) |
| Ochrobactrum anthropii | 2 (0.7%) | - | 2 (1.3%) |
| Sphingobacterium multivorum | 2 (0.7%) | - | 2 (1.3%) |
| Other* | 7 (2.6%) | 2 (1.7%) | 5 (3.3%) |
*The other group includes one strain of each species: Sphingomonas paucimobilis, Comamonas testosteroni, Citrobacter freundii, Chryseobacterium tructae, Acinetobacter lwoffii, Achromobacter mucicolens, and Mould fungi.
The second-most-isolated bacterial strain in the overall population was P. aeruginosa. It was detected in 107 samples (39.5%), representing 40.4% of the population (n = 72). Among children, it was present in 28 samples (23.7%), representing 23.0% of the pediatric population. In adults, it was found in 79 samples (51.6%), representing 49.6% of the adult population.
Coinfection with S. aureus and P. aeruginosa was identified in 50 patients (28.1%), including 39 adults (33.3%) and 11 children (18%).
Among the remaining bacterial strains, Stenotrophomonas maltophilia was identified in 7 children (11.5%) and 5 adults (4.3%), while Achromobacter xylosoxidans was identified in 11 adults (9.4%) and 1 child (1.6%). Haemophilus influenzae was identified in 2 children (3.3%) and 6 adults (5.1%). Klebsiella spp. And Escherichia coli in 7 adults (6.0%) and in 1 child (1.6%). Burkholderia spp. Was isolated in only 4 adults (3.4%).
Physiological upper respiratory tract flora was reported in 37 samples (13.7%) obtained from 20 patients (11.2%).
The primary objective of the study was to identify bacterial strains isolated from the respiratory tract of patients with CF and to determine their in vitro antimicrobial susceptibility to a panel of antibacterial agents.
Because more than one strain of a given species could be cultured from a single sample, a higher number of isolates from certain species or genera were subjected to microbiological analysis. For example, 163 isolates of P. aeruginosa were analyzed. The numbers of other isolates included in the microbiological analysis are provided in Supplementary Table I.
All isolated S. aureus strains showed 100% susceptibility to tigecycline, linezolid, and vancomycin (MIC90 mean values: 0.2, 1.5, and 1.5, respectively), with high susceptibility to co-trimoxazole and ceftaroline (99.4% each; MIC90: 0.094 and 0.8, respectively) and amikacin (98.3%; MIC90: 6.6). For ciprofloxacin and levofloxacin, S. aureus strains were susceptible in 77.8% (MIC: 4.0) and 87.3% (MIC90: 1.8), respectively, under increased exposure. The highest percentage of resistant strains was observed for clindamycin, ciprofloxacin, and tobramycin (23.1%, 19.4%, and 14.7% of resistant strains, respectively) (Fig. 2, Table SI). MRSA isolates were 100% susceptible to ceftaroline, co-trimoxazole, linezolid, and vancomycin. The highest resistance rates were observed for clindamycin (54.5%), ciprofloxacin (45.5%), levofloxacin (54.5%), and tobramycin (63.6%).
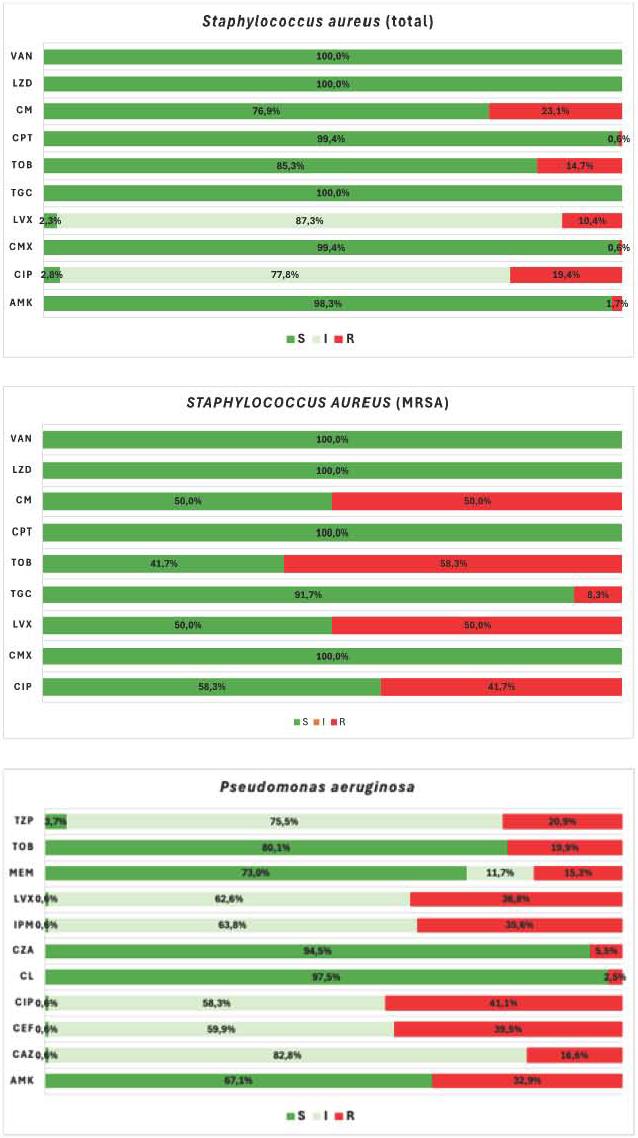
Susceptibility of Staphylococcus aureus (A – total, B – MRSA) and Pseudomonas aeruginosa (C) to the tested antibiotics (using EUCAST criteria).
AMK = Amikacin, CAZ = Ceftazidime, CEF = Cefepime, CZA = Ceftazidime/avibactam, CL = Colistin, CPT = Ceftaroline, CIP = Ciprofloxacin, CM = Clindamycin, CMX = Co-trimoxazole, IPM = Imipenem, MEM = Meropenem, LVX = Levofloxacin, LZD = Linezolid, TGC = Tigecycline, TOB = Tobramycin, TZP = Piperacillin/tazobactam, VAN = Vancomycin. EUCAST categorization: S = Susceptible, standard dosing regimen, I = Susceptible, increased exposure, R = Resistant
For P. aeruginosa, the highest susceptibility was noted for colistin (97.5% of susceptible strains; mean MIC90 value: 1.9) and ceftazidime/avibactam (94.5% of susceptible strains; mean MIC90: 4.0). For tobramycin, 80% susceptibility was observed. For meropenem, 73% susceptibility was observed, with 11.7% under increased exposure, and a mean MIC90 of 32. A significant number of the tested strains were resistant to ciprofloxacin, cefepime, levofloxacin, and imipenem (Fig. 2, Table SI).
A. xylosoxidans showed the highest susceptibility to colistin (85.7%), cotrimoxazole (81.8%), piperacillin/tazobactam (78.6%), imipenem (71.4%), and ceftazidime/avibactam (54.5%), with mean MIC90 values of 7.6, 4.5, 217.6, 32.0, and 256, respectively. However, all strains were resistant to amikacin, cefepime, ciprofloxacin, levofloxacin, tigecycline, and tobramycin (Fig. 3, Table SI). This means that most isolated A. xylosoxidans strains were MDR.

Susceptibility of Burkholderia sp. (A), Achromobacter xylosoxidans (B),% and Stenotrophomonas maltophila (C) to the tested antibiotics (using EUCAST criteria).
AMK = Amikacin, CEF = Cefepime, CAZ = Ceftazidime, CPT = Ceftaroline, CZA = Ceftazidime/avibactam, CIP = Ciprofloxacin, CMX = Co-trimoxazole, CL = Colistin, IPM = Imipenem, LVX = Levofloxacin, MEM = Meropenem, TZP = Piperacillin/tazobactam, TGC = Tigecycline, TOB = Tobramycin. EUCAST categorization: S = Susceptible, standard dosing regimen, I = Susceptible, increased exposure, R = Resistant
Stenotrophomonas maltophilia showed a susceptibility rate of 93.3% (MIC90: 0.8) to co-trimoxazole under increased exposure. The strains were highly resistant to ceftazidime (80%) and levofloxacin (60%) (Fig. 3, Table SI).
Haemophilus influenzae strains were 100% susceptible to ciprofloxacin, levofloxacin, meropenem, and piperacillin/tazobactam. Nearly 90% susceptibility was observed for co-trimoxazole, imipenem, and ceftaroline (88.9% each) (Table SI).
Burkholderia spp. showed no consistent pattern of susceptibility. The strains were most susceptible to meropenem, with 83.3% classified as susceptible and an additional 16.7% considered susceptible under increased exposure conditions (mean MIC90: 5.0). Susceptibility to ceftazidime was 50%, with an additional 16.7% considered susceptible under increased exposure conditions (MIC90: 20). For co-trimoxazole and ceftazidime/avibactam, susceptibility rates were 66.7% and 60%, respectively, with corresponding MIC90 values of 32.0 and 32.0. The highest resistance was observed with levofloxacin – 66.7% (Fig. 3, Table SI).
Details of the in vitro susceptibility analysis of bacterial strains isolated from the respiratory tract of CF patients to various antibacterial agents are presented in Table SI.
No meaningful differences were found in the microbiological flora isolated from samples collected during planned/control visits compared with those obtained during PEx visits. The most common strain was S. aureus, detected in 68.8% of samples from planned visits and 54.5% of samples from PEx visits. P. aeruginosa was isolated from 38.5% and 42.4% of samples, respectively. The occurrence of other strains was as follows: A. xylosoxidans – 2.9% and 10.6%; Burkholderia spp. – 2.4% and 1.5%; E. coli – 3.4% and 1.5%; H. influenzae – 3.4% and 3.0%; Klebsiella spp. – 3.4% and 3.0%; and Stenotrophomonas maltophlia – 4.9% and 7.6%, respectively.
The frequency of bacterial strains identified during the first visit was analyzed in relation to the frequency of PEx reported in the preceding 12 months. Strains more frequently detected in patients with a higher incidence of PEx included A. xylosoxidans, Klebsiella spp., and Pseudomonas spp. In particular, Pseudomonas spp. and A. xylosoxidans were observed at higher frequencies in patients who reported more than 3 exacerbations in the 12 months preceding visit 1.
Among the 233 isolates tested for resistance mechanisms, 73 demonstrated a resistance pattern, including 55 MDR, 11 PDR, and 7 XDR isolates.
The highest number of strains with resistance mechanisms occurred among Gram-negative bacilli. These included P. aeruginosa (35 out of 163 strains tested), S. maltophilia (8 out of 15), A. xylosoxidans (6 out of 14), Burkholderia spp. (2 out of 6), Proteus mirabilis (2 out of 6), and Enterobacter cloacae (2 out of 6). Detailed data on resistance patterns are provided in Table SII.
Among the 163 P. aeruginosa samples tested for resistance mechanisms, 27 exhibited an MDR pattern, accounting for 77.1% of all resistant P. aeruginosa strains. Additionally, 6 PDR strains and 2 XDR strains were identified.
Among children, 12 of 17 resistant isolates (70.6%) were classified as MDR. In adults, the MDR pattern was detected in 15 of 18 resistant isolates (83.3%). A higher prevalence of PDR was observed in children, with 5 of 17 isolates (29.4%) showing this pattern, compared with only 1 case (5.6%) in adults.
An additional analysis of antibiotic resistance patterns was performed to identify other resistance mechanisms in the collected strains. Two mechanisms were identified: MRSA in 12 cases of S. aureus and ESBL in 2 bacterial strains – E. cloacae and Klebsiella spp., with 2 cases each.
The initiation of antibiotic therapy or continuation of therapy initiated after visit 1 was reported in 32 subjects (53.3%), including 21 children (70%) and 11 adults (36.7%), considering only patients who attended at least 2 visits. Most patients (81.2%, n = 26) received 2 or more antibiotics, including 18 children (85.7%) and 8 adults (72.7%). The mean duration of the antibiotic treatment was 5.5 months (median, 2.5 months; range, 0.0–21.4 months), with 3.7 months (median, 3.1 months; range 0.0–14.7 months) in children and 8.8 months (median, 1.1 months; range, 0.0–21.4 months) in adults.
The most used antibiotic was oral azithromycin, predominantly used in CF due to its anti-inflammatory properties: it was used in 21 participants (65.6%) of the total group and in 18 children (85.7%). The second most used antibiotic in the whole group and in children was amikacin (43.8%, n = 14, and 52.4%, n = 11, respectively). The third most frequent antibiotic in the whole group and in children was colistin (21.9%, n = 7, and 28.6%, n = 6, respectively). In adults, several antibiotics, including amikacin, azithromycin, and clindamycin were used with the same frequency (27.3%, n = 3 each).
The aim of this noninterventional study was to investigate the current etiology and epidemiology of bacterial infections in Polish patients with CF. The study also evaluated the in vitro antimicrobial susceptibility of bacterial strains isolated from the respiratory tract to commonly used antibacterial drugs and analyzed resistance patterns of the identified pathogens.
CF is characterized by recurrent bacterial respiratory infections. With disease progression, many patients become infected with less common and more difficult-to-treat microorganisms, such as Burkholderia cepacia (Perikleous et al. 2023). With disease progression, many patients become infected with more uncommon and difficult-to-treat microorganisms, such as B. cepacia (Perikleous et al. 2023). Extensive antibiotic use and declining respiratory function eventually promote the emergence of opportunistic pathogens, such as Achromobacter spp. and S. maltophilia (Menetrey et al. 2020).
Data collected from CF patients in this study are consistent with the existing literature. In our study, S. aureus was the most common strain, detected in over 70% of patients, with a higher prevalence in pediatric patients (75.4%) compared with adults (70.9%). The literature shows that the prevalence of S. aureus exceeds 50% in infants and peaks at 80% in early adolescence (Sands et al. 2021). In the second and third decades of life, this strain becomes less frequent, accompanied by a steady increase in P. aeruginosa colonization rates (Valenza et al. 2008; Fisher et al. 2021). In this study, P. aeruginosa was the second most common pathogen, identified in 40.4% of patients, including nearly one-quarter of children and half of adults. Registry studies reported a prevalence of P. aeruginosa of 55% among adult patients with CF (Fisher et al. 2021; Turcios 2020). The prevalence of P. aeruginosa has decreased, especially among those under 18 years of age, from 47% in 1997 to 27.5% in 2017 (Blanchard and Waters 2019). Coinfection with S. aureus and P. aeruginosa was common, occurring in 28% of patients in the present study, consistent with previous reports reporting rates of 30.6% to 50.7% (Fisher et al. 2021).
S. aureus has a high ability to acquire resistance to antibiotics, partly due to its ability to form biofilm (Perikleous et al. 2023). The isolation of MRSA is an increasing concern, as it is associated with deterioration of lung function and impaired somatic development in children (Turcios 2020). Vancomycin and linezolid are first-line treatments for patients with CF and MRSA-related PEx (Perikleous et al. 2023). Ceftaroline seems to be a promising agent against MRSA, but experience with this drug in patients with CF is limited (Turcios 2020; Lo et al. 2022). In the present study, all S. aureus strains were susceptible to linezolid, vancomycin, and tigecycline, with high susceptibility to ceftaroline, co-trimoxazole, and amikacin. They were also susceptible to ciprofloxacin and levofloxacin at higher exposure levels. However, nearly a quarter of the strains were resistant to clindamycin, with moderate resistance to tobramycin and ciprofloxacin. A total of 12 MRSA isolates were identified in 8 patients.
Treatment of P. aeruginosa infections in CF patients is challenging due to the pathogen’s resistance to many antibiotics (Pang et al. 2019). MDR P. aeruginosa is a major concern, and the World Health Organization has identified carbapenem-resistant strains as a critical priority for the development of new antibiotics (Tacconelli et al. 2018; Perikleous et al. 2023). Ceftazidime/avibactam has shown significant (>70%) in vitro activity against resistant strains in adults with CF (Atkin et al. 2018). In this study, P. aeruginosa showed the highest susceptibility to colistin (97.5%), followed by ceftazidime/avibactam (94.5%) and tobramycin (80%). MDR P. aeruginosa strains were identified in most samples tested in this study (77.1%), more often in adults (83.3%) than in children (70.6%). According to the literature, more than 50% of individuals with CF aged 18 years or older in the United States are infected with P. aeruginosa, of whom approximately one-third are classified as MDR (Atkin et al. 2018). The diversity of antibiotic resistance mechanisms contributes to the development of MDR P. aeruginosa strains. As a result, conventional antibiotic therapies against P. aeruginosa infections have become increasingly ineffective (Pang et al. 2019; Perikleous et al. 2023). In our study, the high prevalence of the MDR pattern (77.1%) among resistant P. aeruginosa strains underscores the growing challenge of antimicrobial resistance. The identification of six PDR and two XDR strains further highlight the severity of the resistance problem. Interestingly, the pediatric population exhibited a higher proportion of PDR strains (29.4%) compared to adults (5.6%), suggesting a greater vulnerability in younger patients. Interestingly, the study also found a significant number of microbiological samples containing rarer bacterial species such as Stenotrophomonas spp., Burkholderia spp. Achromobacter spp., Comamonas testosteroni, Ochrobactrum anthropii, and Sphingomonas paucimobilis. Many of these isolates showed high levels of multidrug resistance, leaving limited treatment options available. Careful monitoring of the prevalence of such strains in CF patients is essential to prevent them from becoming an even more serious clinical challenge in this population.
The literature shows increasing rates of S. maltophilia infections in CF patients (Goss et al. 2004). The prevalence of Achromobacter infections has been reported to range from 3% to 30% (Blanchard et al. 2019). The epidemiology of B. cepacia complex infections in CF has been extensively studied due to the potential for transmission between patients. In 2017, 2.4% of individuals with CF in the CF Foundation Patient Registry Annual Report were culture positive for these strains (Blanchard et al. 2019). According to other sources, the prevalence of B. cepacia complex in patients with CF is estimated at 2% to 3%, with adults more frequently affected (Turcios 2020).
Antibiotics are the cornerstone of CF management, with patients often undergoing repeated courses of broad-spectrum antibiotics to improve quality of life and increase life expectancy. Early initiation of appropriate antibiotic therapy, based on in vitro susceptibility, is essential to treat bacterial infections and prevent serious complications (Perikleous et al. 2023).
The role of antimicrobial susceptibility results obtained in this study should be interpreted with caution. In vitro testing of CF pathogens does not always accurately reflect the complex milieu of the CF airway (Høiby et al. 2010; Nolan et al. 2021). Although in vitro susceptibility results may contribute to clinical decision-making, they do not always correlate with treatment outcomes; therefore, the clinical efficacy of antimicrobial agents cannot be determined solely based on these results (Atkin et al. 2018). Moreover, the observation that one strain appears more susceptible than another in vitro does not necessarily predict a successful clinical outcome.
The study also aimed to analyze microbiological results obtained during PEx and routine visits. No relevant differences in the frequency of isolated strains were observed. The diversity of bacterial strains was similar between adult and pediatric populations, as well as between patients with and without exacerbations. However, the low frequency of certain strains limits the strength of any conclusions. Nonetheless, this observation aligns with recent studies of inhaled antipseudomonal therapies (tobramycin and aztreonam), which demonstrated that sputum microbiota remains relatively stable during treatment in CF (Caverly and VanDevanter 2022).
Data collected on the disease course prior to enrollment showed that Pseudomonas spp. and A. xylosoxidans were more frequently isolated from patients who reported more than 3 exacerbations in the 12 months preceding enrollment. This finding supports the potential role of A. xylosoxidans in CF and is consistent with the results of a case-control retrospective study published in 2021. In that study, the annual rate of respiratory exacerbations increased in the year following A. xylosoxidans infection compared with the preceding year, along with a higher frequency of hospital admissions and oral antibiotic use (Marsac et al. 2021). However, due to the limited number of detections, the relative risk of exacerbation was calculated in the current study only in respect to the presence of S. aureus and P. aeruginosa.
A total of 81 patients received CFTR modulators during the follow-up. The use of these modulators improves clinical outcomes, including a reduction in PEx frequency, although their effects on respiratory bacterial flora remain under investigation. However, this issue was not the focus of the present study (Milczewska et al. 2024).
According to the demographic data, the mean age of study participants was nearly 23 years, considerably higher than the 2021 European Cystic Fibrosis Society Patient Registry (ECFSPR) reported mean age. In that report, the mean age of CF patients in Poland was 15.6 years, with 64.6% younger than 18 years and 35.4% older than 18 years (Zolin et al. 2023). In contrast, in the present study, 34.6% of participants were children and 65.4% were adults. This distribution may account for the higher mean age observed in the current study compared with the ECFSPR data.
The results of this study may have important implications for clinical practice in Poland. The consistently high susceptibility of S. aureus strains to linezolid, vancomycin, tigecycline, and ceftaroline, as well as the good in vitro activity of ceftazidime/avibactam and colistin against P. aeruginosa, suggest that these agents could be considered as key therapeutic options in the management of PEx in CF patients. Conversely, the high resistance rates to ciprofloxacin and cefepime highlight the need for cautious use of these drugs in empirical therapy. These findings may support updates of local antibiotic treatment guidelines for CF in Poland, particularly with respect to the role of newer beta-lactam/beta-lactamase inhibitor combinations and the limited usefulness of some older agents. Regular surveillance studies such as the present one are essential for informing evidence-based adjustments to treatment strategies and formularies, thereby improving the effectiveness of antibiotic therapy in the CF population.
This study has several limitations. First, as an observational study, the clinical characteristics of participants were similar to those typically seen in screening programs. The study population was limited to 3 centers and may not fully represent the broader CF population in Poland, as differences in patient age were observed compared with other data sources. Second, the small number of samples from strains other than the two most common strains limits conclusions on susceptibility and resistance, thereby constraining the ability to assess broader implications for antibiotic therapy in CF.
In conclusion, S. aureus was the most common strain detected in CF patients and showed high susceptibility to tigecycline, linezolid, vancomycin, co-trimoxazole, and ceftaroline. P. aeruginosa, the second most common strain, was susceptible to colistin, ceftazidime/avibactam, and tobramycin, with the highest resistance to ciprofloxacin and cefepime. Coinfection with S. aureus and P. aeruginosa was more common in adults.
Bacterial diversity was comparable between adults and children, although the low frequency of certain species limited the statistical analysis. Most samples were not evaluated for resistance patterns; however, P. aeruginosa strains were frequently classified as MDR. MRSA and ESBL-producing strains of E. cloacae and Klebsiella spp. were also identified.