The genus Pseudomonas, part of the Pseudomonadaceae family, includes several species, such as Pseudomonas aeruginosa, Pseudomonas putida, Pseudomonas luteola, and Pseudomonas fluorescens. These Gram-negative, motile, and aerobic rods are known for their rapid growth and adaptability across various environments. Pseudomonas species are ubiquitous, thriving in natural settings like soil and water, as well as in clinical and artificial environments such as catheters and contact lenses (Jurado-Martín et al. 2021).
Among these, P. aeruginosa is particularly notorious for its extensive virulence arsenal and its role in hospital-acquired infections, especially in immunocompromised individuals. This bacterium can colonize various hospital surfaces and equipment, making its distribution patterns crucial for effective infection control measures. For instance, water outlets in UK hospitals were identified as likely sources of P. aeruginosa, highlighting the need to control these sources to prevent transmission (Halstead et al. 2021).
P. aeruginosa significantly impacts mortality rates in healthcare settings, particularly among burn victims, cystic fibrosis (CF) patients, and individuals with weakened immune systems. It is a notable nosocomial pathogen, with a high incidence of ventilator-associated and hospital-acquired pneumonia reported in China (Ding et al. 2016). The pathogenic capacity of P. aeruginosa to cause both acute and chronic infections is further complicated by its intrinsic and acquired resistance mechanisms to antibiotics, making eradicating infections particularly challenging (Pang et al. 2019).
The emergence of multidrug-resistant (MDR) strains of P. aeruginosa, exacerbated by the widespread use of broad-spectrum antibiotics, presents significant challenges to healthcare systems worldwide. This issue is underscored by the increasing prevalence of MDR P. aeruginosa in hospital infections, highlighting the significant global challenge posed by antimicrobial resistance (Lila et al. 2017; Mekonnen et al. 2021). The bacterium’s ability to form biofilms and resist multiple antibiotic classes further complicates treatment efforts (Ciofu and Tolker-Nielsen 2019).
P. aeruginosa harbors various resistance genes, such as blaCTX-M, blaSHV, qnrB, and blaACC-1, which enhance its defense against multiple antibiotics and complicate clinical management. These genes underscore the bacterium’s adaptability and need for innovative antibiotic development and resistance management strategies (Bonomo 2017).
In Iraq, P. aeruginosa poses a significant threat in clinical settings. Studies have reported a high prevalence of MDR and extensively drug-resistant (XDR) P. aeruginosa in hospitals, highlighting its extensive presence and resistance patterns. Clinical and environmental samples have revealed significant contamination in various hospital areas and a notable prevalence among healthcare workers’ hands and patients’ specimens (Alkhulaifi and Mohammed 2023; Mohammed Said et al. 2023). The escalating issue of antimicrobial resistance in Kurdistan further underscores the critical challenge posed by P. aeruginosa in the region (Qurbani et al. 2024).
Given the significant threat posed by P. aeruginosa in hospital settings, especially in regions with healthcare challenges, comprehensive studies on its prevalence, distribution, and antibiotic resistance profiles are urgently needed. This study aims to investigate these aspects in hospitals in Sulaymaniyah City, Iraq. By utilizing bacteriological, biochemical, and molecular methods, including PCR targeting of 16S rDNA sequences, we aim to characterize P. aeruginosa isolates from various hospital surfaces. Furthermore, this research seeks to identify antibiotic resistance genes, thereby enhancing our understanding of P. aeruginosa epidemiology in this region and potentially revolutionizing the development of effective infection control measures.
A comprehensive survey assessed bacterial contamination levels across various locations within seven hospitals in Sulaymaniyah City. A total of 300 samples were meticulously collected from diverse surfaces, including mops, sinks, medical waste, medical equipment, beds, desks, and floors. The hospitals included in the study were Emergency, Paediatric, Maternity, Teaching, Shahid Hemn, Hiwa, and Shar. Swab samples were collected under aseptic conditions using sterile cotton swabs (HEM Ltd., Russia) moistened with sterile saline solution (PiONEER Co. for Pharmaceutical Industries, Iraq). Each surface area was swabbed thoroughly to ensure uniform sampling (DES 2018). The swabs were immediately transferred to sterile containers and transported to the laboratory for further processing.
Upon receipt in the laboratory, swabs were streaked onto Cetrimide Agar medium (HiMedia Laboratories, LLC., India) and incubated at 37°C for 24–48 hours in an incubator (Memmert GmbH + Co.KG, Germany), as Cetrimide Agar is specific for the primary isolation of Pseudomonas species. Isolates showing growth on Cetrimide Agar were subjected to oxidase and catalase tests for preliminary identification. Oxidase Test Strips (Bioanalyse, Türkiye) and 3% hydrogen peroxide solution (HiMedia Laboratories, LLC., India) were used for these tests, respectively.
Final confirmation of Pseudomonas spp. was conducted through PCR amplification of 16S rRNA using specific primers (Sinaclon Co., Iran) for Pseudomonas species and P. aeruginosa. Briefly, bacterial DNA was extracted using the boiling method, as described by Dashti et al. (2009). Bacterial cells were suspended in 100 μl of sterile distilled water and boiled at 99°C for 10 seconds. The lysate was then centrifuged using a microcentrifuge (Biofuge, Germany), and the supernatant containing DNA was collected. PCR assays targeting 16S rDNA of Pseudomonas species and P. aeruginosa were performed using primers described by Mohammed et al. (2015). For Pseudomonas species identification, primers Pseudo S2-F (5’-GACGGGTGAGTAATGC-CTA-3’) and Pseudo S2-R (5’-CACTGGTGTTCCTTC-CTATA-3’) were used, amplifying a 670 bp fragment. For P. aeruginosa-specific identification, primers Pseud PA-SS-F (5’-GGGGGATCTTCGGACCTCA-3’) and Pseud PA-SS-R (5’-TCCTTAGAGTGCCCCACCCG-3’) were used, amplifying a 956 bp fragment.
Antimicrobial susceptibility testing was performed using the Kirby-Bauer disk diffusion method on Mueller-Hinton agar plates (HiMedia Laboratories, LLC., India). Five antibiotics, including streptomycin (10 μg), tobramycin (10 μg), moxifloxacin (5 μg), levofloxacin (5 μg), and norfloxacin (10 μg) (all from Bioanalyse, Türkiye), were selected based on guidelines outlined by the Clinical Laboratory Standards Institute (CLSI 2023). Zones of inhibition were measured and interpreted according to CLSI criteria to determine antibiotic susceptibility profiles.
PCR assays targeting antibiotic resistance genes (blaCXT-M, blaSHV, blaACC-1, and qnrB) were conducted using primers described by El-Doloy et al. (2006) and Ahmed et al. (2007).
PCR amplification was conducted in a 20 μl reaction mixture using an Applied Biosystems thermocycler (SBSbio, China). The reaction mixture consisted of 10 μl of 2 × premix Red Taq polymerase (iNtRON Biotechnology, Inc., Republic of Korea), 2 μl of bacterial DNA template, 1 μl of nuclease-free water (iNtRON Biotechnology, Inc., Republic of Korea), and 2 μl of specific primers targeting the desired gene regions as shown in Table I.
Distribution of resistance genes Pseudomonas aeruginosa.
| Gene | Target | Amplicon size | Primer Sequences (5’ to 3’) | Prevalence |
|---|---|---|---|---|
| blaCXT-M | Beta lactamase resistance gene (CTX-M) | 550 bp | F: CGCTTTGCGATGTGCAG | 10/26 (38.4%) |
| blaSHV | Beta lactamase resistance gene (SHV) | 800 bp | F: TTATCTCCCTGTTAGCCACC | 3/26 (11.5%) |
| blaACC-1 | Bet lactamase resistance gene (ACC-1) | 873 bp | F: CACCGAAGCCGTTAGTTGAT | 3/26 (11.5%) |
| qnrB | Quinolone resistance gene | 469 bp | F:GATCGTGAAAGCCAGAAAGG R: ACGATGCCTGGTAGTTGTCC | 3/26 (11.5%) |
The PCR amplification protocol commenced with an initial denaturation step at 95°C for 5 minutes, followed by 35 cycles of denaturation at 95°C for 30 seconds, annealing at 55°C for 30 seconds, and extension at 72°C for 30 seconds. A final extension step was performed at 72°C for 7 minutes to ensure complete amplification.
Subsequently, 10 μl of the PCR products were loaded onto a 1% agarose gel (iNtRON Biotechnology, Inc., Republic of Korea) and subjected to electrophoresis using a DNA gel electrophoresis system (Biotec-Fischer, Germany) at 100 volts for 30 minutes. Following electrophoresis, the gel was visualized under ultraviolet (UV) light using an Accuris™ UV Transilluminators (Accuris Instruments, USA) to observe the DNA bands. Gel images were then captured using a SmartDoc™ gel imaging system (Accuris Instruments, USA) for further analysis and documentation.
The characterization of Pseudomonas colonies on selective medium and biochemical testing indicate their characteristic green or blue-green coloration on Cetrimide Agar. Moreover, Pseudomonas species test positive for both oxidase and catalase, indicating the presence of cytochrome c oxidase and catalase enzymes, respectively, aiding in their identification.
The final confirmation of identification by specific genus amplification recorded that 66 isolates were confirmed as Pseudomonas, with only 26 isolates confirmed as P. aeruginosa. Fig. 1 illustrates the PCR amplification of the 16S rRNA gene, with a specific band size of 670 bp indicative of Pseudomonas species, and the specific amplification of the P. aeruginosa isolates, yielding a band size of 956 bp. The amplified products were visualized on a 1% DNA agarose gel alongside a 1.2 Kb DNA ladder for size comparison.
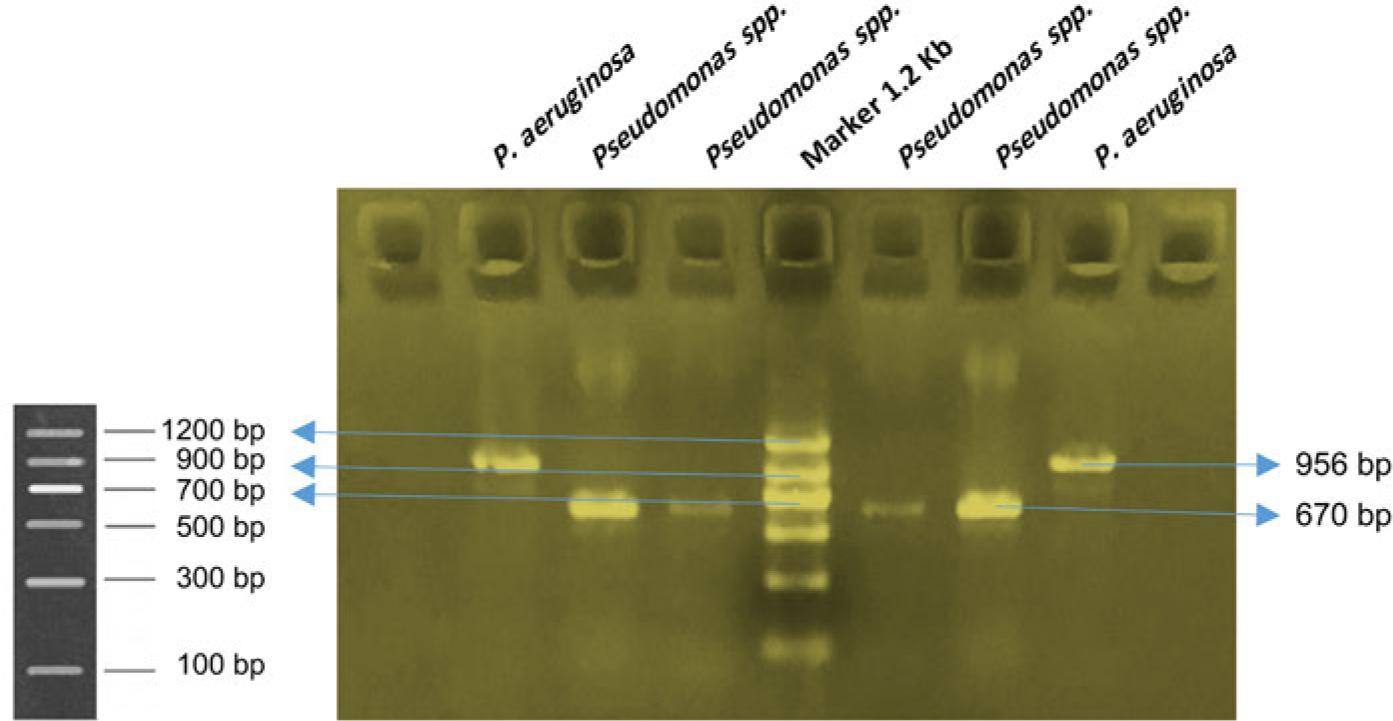
PCR confirmation of Pseudomonas species.
The 16S rRNA gene amplification product of 670 bp specific for Pseudomonas species and a 956 bp product for P. aeruginosa were run on 1% DNA agarose gel using 1.2 kbp DNA ladder.
Antibiotic susceptibility testing was performed to evaluate the resistance patterns of P. aeruginosa isolates to various antibiotics. The test revealed the resistance rates of P. aeruginosa to different antibiotics among the 26 samples analyzed. The resistance percentages were as follows: streptomycin (23.33%), tobramycin (13.63%), moxifloxacin (22.72%), levofloxacin (21.21%), and norfloxacin (22.72%), as shown in Fig. 2.
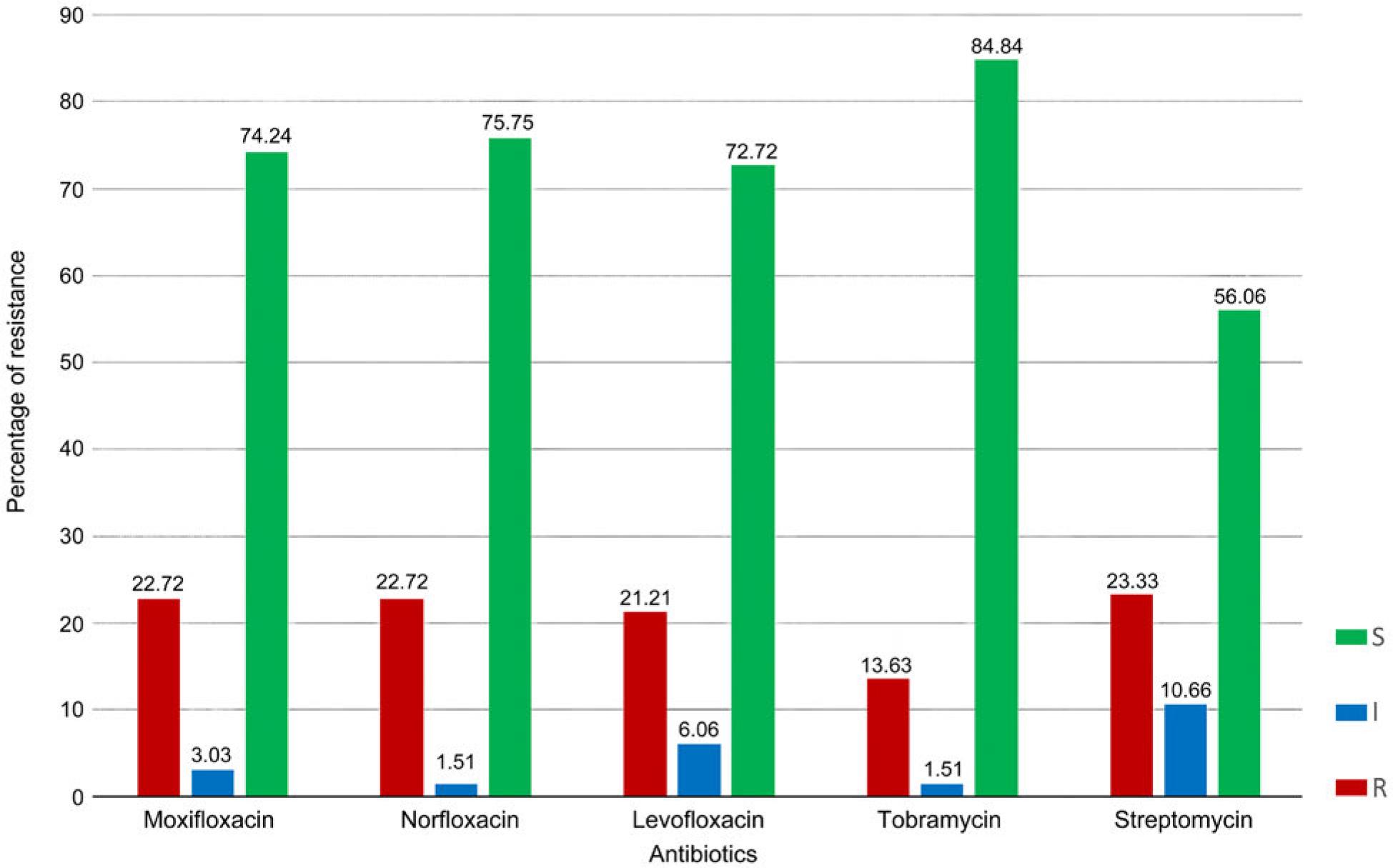
The rate of antibiotic resistance in 26 Pseudomonas aeruginosa isolates.
Of the 300 samples collected from various surfaces in seven hospitals, 66 were contaminated with Pseudomonas species, representing a contamination rate of 22%. Among these positive samples, only five hospitals with 26 were identified as P. aeruginosa, accounting for 39.39% of the Pseudomonas positive cases as shown in Table SI.
The examination of P. aeruginosa isolates in five hospitals revealed different levels of contamination, with Shar Hospital having the highest number of isolates (15) and Emergency Hospital having the lowest (1). Shar Hospital showed extensive contamination on various surfaces including mop, sink, floor, bed, and medical waste surfaces. Pediatric Hospital followed with six isolates found mainly on beds, bench, floor, mop and sink surfaces. Shahid Hemn and Hiwa hospitals each had two isolates, predominantly on mop and floor surfaces, as shown in Fig. 3.
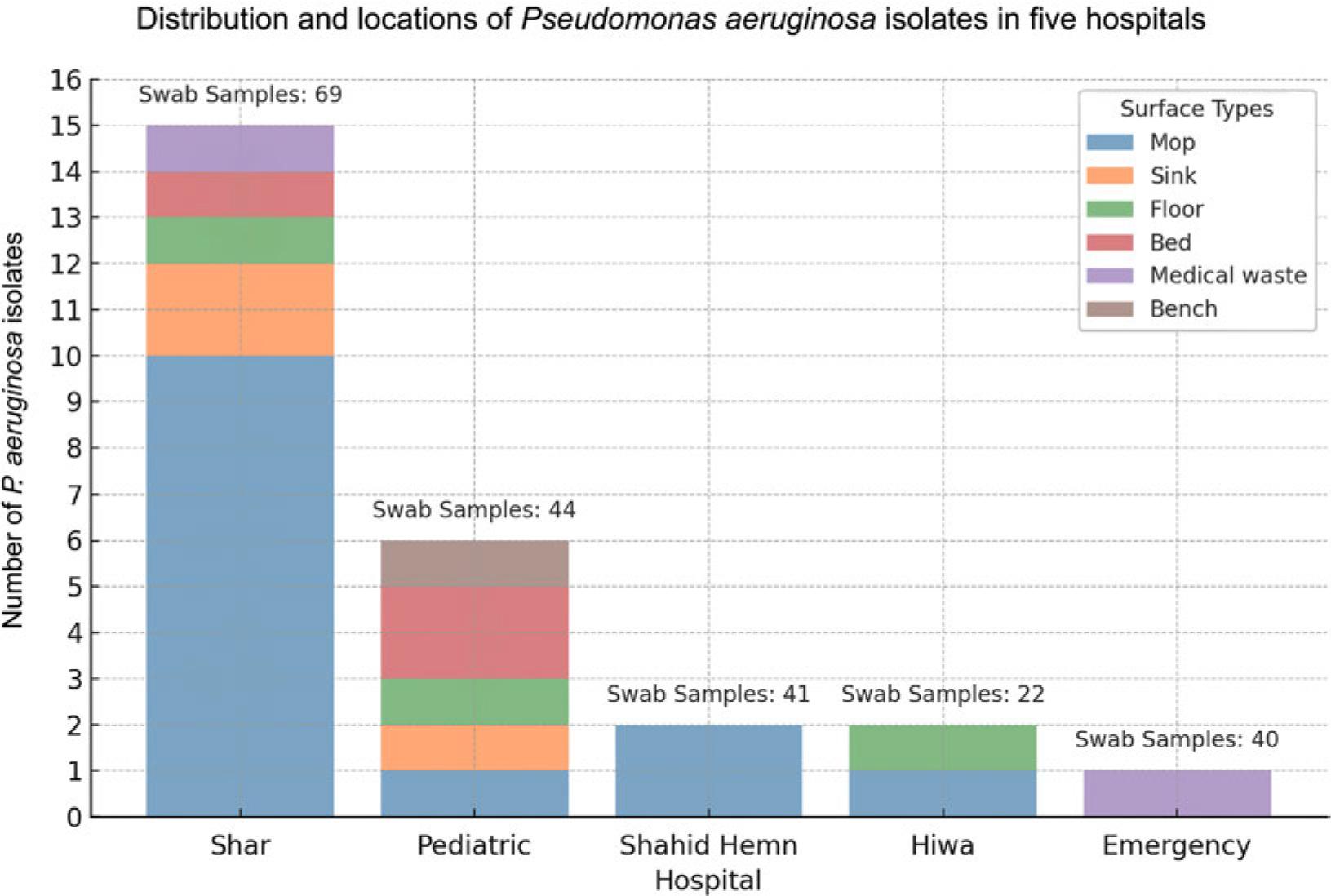
The distribution of Pseudomonas aeruginosa isolates across surface types in five hospitals. Colors denote different surfaces sampled, with total swab counts displayed above each bar.
Among the 26 P. aeruginosa isolates analyzed, several antibiotic resistance genes were detected. The distribution of these genes is summarized in Table I. Notably, the blaCTX-M gene was the most common, found in 10 isolates (38.4%). In addition, the blaSHV, blaACC-1, and qnrB genes were each detected in three isolates (11.5% each). These results highlight the diversity of antibiotic resistance mechanisms present in the isolated P. aeruginosa strains.
Our comprehensive investigation into the presence and antibiotic resistance patterns of Pseudomonas spp., particularly P. aeruginosa, in hospital settings in the city of Sulaymaniyah highlights the complex challenge of managing infections caused by this formidable pathogen. Using selective media, biochemical assays, and molecular techniques, we’ve aligned our methodology with established frameworks to identify and characterize these bacterial isolates, reinforcing the need for precise diagnostic strategies in the clinical management of infections. The discernible pigmentation and enzymatic activity of P. aeruginosa on Cetrimide Agar, as noted by Fujitani et al. (2011), along with our PCR verification of the 16S rRNA gene, reflects the critical role of comprehensive diagnostics, as highlighted by Deschaght et al. (2011), in the identification of this opportunistic bacterium. Our results reveal a significant pattern of resistance across a spectrum of antibiotics, describing a worrisome trend in P. aeruginosa’s ability to evolve multidrug resistance mechanisms. This scenario, as highlighted by Qurbani et al. (2024), exacerbates existing healthcare challenges within Kurdistan, Iraq, and underscores a broader global health crisis of antimicrobial resistance. Rampant environmental contamination, facilitated by indiscriminate antibiotic use and inadequate infection control measures, underscores the need for improved cleaning protocols and robust antimicrobial stewardship.
The emergence of multidrug-resistant P. aeruginosa strains underscores a critical therapeutic challenge, requiring targeted treatment strategies and careful antibiotic stewardship to avoid resistance escalation (Nolan and Behrends 2021; Sun et al. 2011). Our data confirm the need for nuanced therapeutic interventions, especially for CF patients besieged by MDR P. aeruginosa, echoing the sentiments of Stefani et al. (2017) regarding the central role of antibiotic susceptibility testing in therapeutic decision-making. Ibrahim et al. (2020) Giovagnorio et al. (2023) and further elaborate on the complexity of treating P. aeruginosa infections and the importance of novel antibiotics and combination therapies in combating these resistant strains. Our study not only confirms these concerns, but also provides a detailed resistance profile that underscores the urgency of innovative treatment methods to counteract the adaptive resistance mechanisms of P. aeruginosa.
The adaptive capacity of P. aeruginosa is further exemplified by its ability to form biofilms, which contribute significantly to its persistence in hospital environments and to antimicrobial resistance. P. aeruginosa biofilms pose a formidable challenge in clinical settings, serving as reservoirs for chronic infections and facilitating horizontal transfer of resistance genes (Sharma et al. 2019). This highlights the need for therapeutic strategies that not only target planktonic cells, but also address the biofilm growth mode.
Our investigation delineates a contamination rate of 22% for P. aeruginosa across various hospital surfaces, accentuating the persistent risk of hospital-acquired infections (HAIs) and the pivotal role of environmental reservoirs in facilitating the spread of this pathogen. The role of environmental reservoirs in disseminating P. aeruginosa is a critical concern in preventing HAIs. Beyond its clinical impact, P. aeruginosa extends its dominion into environmental microbiology. As a ubiquitous environmental bacterium, it traverses various ecological niches with remarkable adaptability, aided by a genome characterized by plasticity and high nutritional versatility (Grosso-Becerra et al. 2014). This connection reinforces the need for stringent environmental hygiene protocols in healthcare settings to minimize the incidence of HAIs (Panagea et al. 2005).
The linkage between environmental contamination and potential patient-to-patient transmission routes, highlighted by outbreaks traced back to contaminated surface cleaning equipment (Engelhart et al. 2002), necessitates comprehensive infection control protocols to mitigate HAIs effectively. Recent studies by Kotay et al. (2017) have demonstrated the potential for pathogens to disperse from sink traps to patients, emphasizing the importance of addressing often-overlooked environmental reservoirs in infection control strategies. This underscores the need for a holistic approach to hospital hygiene encompassing both direct patient care practices and environmental management.
This study’s identification of varied contamination levels across hospitals pinpoints the necessity for tailored cleaning protocols that address high-risk areas and high-touch surfaces to curtail the spread of P. aeruginosa. The role of environmental cleaning in infection control, as discussed by Dancer (2010; 2011; 2014) and the implications of contaminated surfaces on patient infections underline the significance of enhanced cleaning practices alongside hand hygiene to mitigate infection risks. In light of these findings, innovative decontamination methods, such as ultraviolet devices and hydrogen peroxide systems, as reviewed by Weber et al. (2016), may offer promising solutions for terminal room decontamination and warrant further investigation in our hospital settings.
Moreover, the detection of antibiotic resistance genes, including blaCTX-M, blaSHV, qnrB, and blaACC-1, in our P. aeruginosa isolates illuminates the sophisticated resistance arsenal of this pathogen. The widespread presence of the blaCTX-M gene, indicative of extended-spectrum β-lactamase (ESBL) production, presents considerable obstacles in selecting effective therapies, reinforcing the global concern over ESBL-producing strains and the paramount need for novel therapeutic avenues to address these challenges. Partridge et al. (2018) have extensively documented the role of mobile genetic elements in disseminating antimicrobial resistance genes, highlighting the potential for rapid spread of resistance within bacterial populations. This genetic mobility underscores the need for surveillance programs that monitor phenotypic resistance and the genetic determinants of resistance.
This study highlights the significant prevalence and distribution of P. aeruginosa on hospital surfaces in Sulaymaniyah city, emphasizing the pathogen’s role as a critical agent of hospital-acquired infections. With a contamination rate of 22% across various hospital environments and a notable presence of antibiotic resistance, our findings shed light on the urgent need for enhanced infection control measures and the development of new antimicrobial strategies. The detection of antibiotic resistance genes, including blaCTX-M, underscores the challenge posed by extended-spectrum β-lactamase-producing strains, further complicating the fight against these infections. Our study advocates for rigorous environmental hygiene practices, targeted antimicrobial stewardship, and innovative diagnostic and therapeutic approaches to curtail the spread of multidrug-resistant P. aeruginosa.