
hs-TnT levels of patients hospitalized for heart failure differ between men and women.
hs-TnT ≥15.83 pg/mL for women and hs-TnT ≥19.02 pg/mL for men were independently associated with all-cause long-term mortality prediction.
These sex-specific cut-off values of hs-TnT improved all-cause long-term mortality prediction.
Sex-based disparities in patients with heart failure (HF) span from the etiology to the clinical and biological characteristics and reflect on the intensity and efficacy of the therapeutical management as well [1].
Although current guidelines from professional societies [2][3] acknowledge these differences, they still lack concrete, practical gender-tailored recommendations. It is well-established that women are more likely to develop heart failure with preserved ejection fraction (HFpEF), commonly associated with hypertension, obesity, and diabetes, whereas men typically present with heart failure with reduced ejection fraction (HFrEF), predominantly caused by coronary artery disease [4][5]. Despite these known differences, the underlying biological mechanisms responsible for the distinct HF subtypes in men and women remain poorly understood. Research has demonstrated that women with HF, particularly HFpEF, generally exhibit better survival compared to men; however, this advantage diminishes significantly with diabetes, a condition posing a higher relative HF risk in women compared to men [6]. The underrepresentation of women in clinical trials and the absence of gender-specific treatment guidelines further highlight our incomplete understanding of how biological differences between sexes contribute to these observed outcomes [7].
Despite progress in identifying sex-specific risk factors for heart failure, such as pregnancy-related conditions [8], significant knowledge gaps remain. Although women are at an increased risk for developing HFpEF, limited research exists on hormonal influences, particularly the roles of estrogen and menopause, contributing to this disparity [9]. Addressing these gaps through focused studies is necessary to develop tailored strategies for prevention and treatment in women.
Biomarkers like NT-proBNP and high-sensitivity cardiac troponin (hs-Tn) are essential tools for diagnosing and managing heart failure, yet sex differences in their baseline levels and prognostic value have been scarcely characterized [10]. NT-proBNP is widely recognized as a reliable biomarker for HF diagnosis and prognosis, predicting outcomes such as hospitalization and mortality, particularly in patients with HFrEF [11]. Women generally exhibit higher NT-proBNP concentrations than men, even in healthy populations [12][13]. Regardless, NT-proBNP consistently predicts adverse outcomes across both sexes, suggesting its broad prognostic value, though adjustments for sex-specific thresholds may be warranted [11]. Similarly, hs-Tn levels are often elevated in heart failure, even in the absence of acute myocardial infarction, and persistent elevation indicates worse prognosis, including increased mortality and hospitalization rates [14]. In the general population, hs-Tn levels tend to be higher in men compared to women [15][16]. Guidelines now recommend sex-specific reference thresholds for hs-Tn to avoid myocardial infarction misdiagnosis, particularly in women [17].
Data regarding the distinct prognostic value of hs-Tn across sexes in heart failure remain conflicting: some studies report comparable predictive values for both genders [18], while others indicate stronger associations in men [19].
Therefore, we aimed to characterize sex-related differences in admission high-sensitivity troponin T (hs-TnT) and to evaluate their association with long-term all-cause mortality in patients hospitalized for heart failure.
We conducted a retrospective observational cohort study derived from the Hematological Indices in Heart Failure (HI-HF) database, a single-center registry including consecutive adults hospitalized for heart failure (HF) in the Cardiology Department of Colentina University Hospital (Bucharest, Romania) between January 2011 and December 2014. The parent cohort design, eligibility framework, and index hospitalization data capture have been previously reported [14][20].
The present analysis represents a prespecified biomarker-focused sub-study evaluating sex-related differences in high-sensitivity troponin T (hs-TnT) and its association with long-term prognosis in HF.
The study protocol was approved by the Hospital’s Ethical Committee on October 10th, 2018. All participants provided informed consent for the use of their clinical data for research purposes. All procedures complied with the Declaration of Helsinki.
From the HI-HF registry [20], we assembled a cohort of patients (Figure 1) with non-missing survival time and vital status, complete electronic medical records, admission hs-TnT and NT-proBNP, and a comprehensive transthoracic echocardiographic examination performed during the index hospitalization.
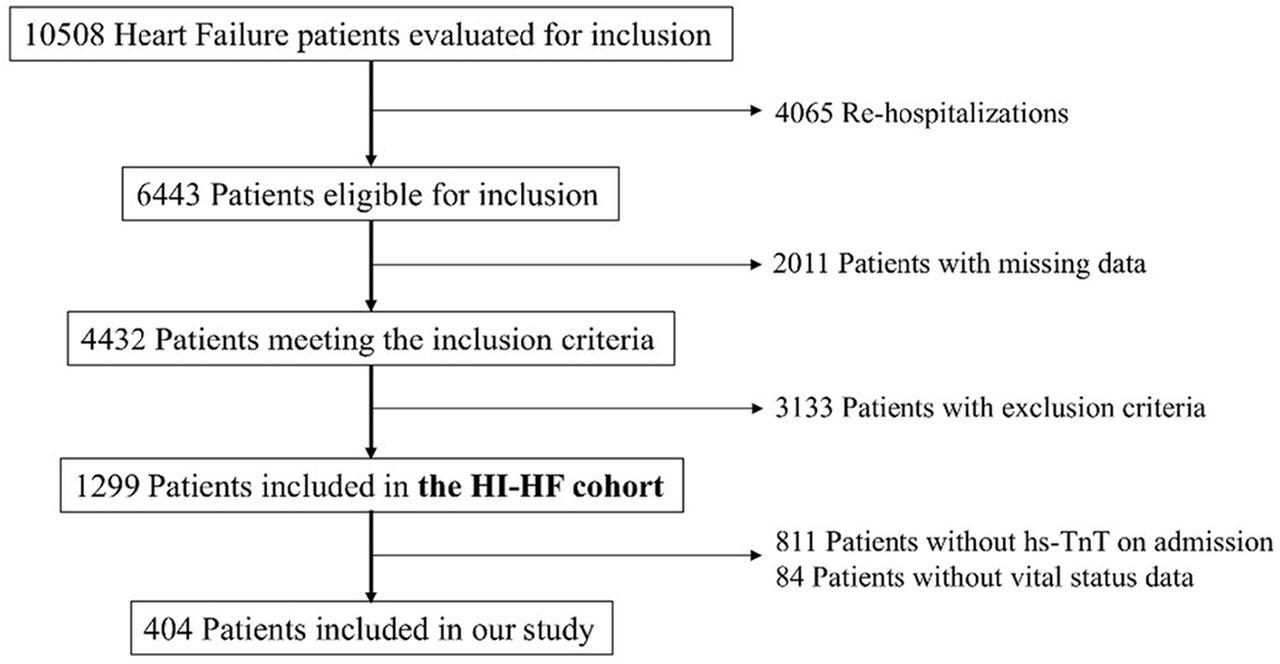
PRISMA consort flow diagram of the study.
Consistent with the parent cohort design, we applied prespecified exclusion criteria to reduce confounding from conditions expected to influence biomarker concentrations or prognosis independent of HF, including acute coronary syndromes, acute pulmonary embolism, active infection/inflammatory systemic disease, autoimmune disease, active malignancy or recent oncological treatment, and moderate-to-severe anemia.
Only the index hospitalization for each patient was considered, consistent with the registry’s approach of excluding readmissions during the enrollment interval.
HF diagnosis followed contemporaneous guideline-based clinical criteria used in the HI-HF registry, such as compatible signs or symptoms, elevated natriuretic peptides, and additional structural or functional criteria when ejection fraction was preserved.
Atrial fibrillation (AF) was defined based on documented atrial fibrillation/flutter. AF diagnosis included paroxysmal, persistent and permanent AF, as well as valvular and non-valvular AF.
Renal function was summarized by estimated glomerular filtration rate (eGFR) computed using the CKD-EPI equation.
Prolonged hospitalization was defined as >7 days.
Demographics, cardiovascular history, comorbidities, and index presentation features were extracted from electronic health records.
Transthoracic echocardiography was performed during the index hospitalization as part of routine clinical evaluation. Left ventricular ejection fraction (LVEF) was analyzed primarily as a continuous variable.
NT-proBNP was measured using Roche Diagnostics Elecsys® proBNP II immunoassay. Troponin T was measured using the Roche Diagnostics Elecsys® Troponin T STAT electrochemiluminescence immunoassay. Troponin concentrations are reported as pg/mL (numerically equivalent to ng/L). Two hs-TnT operational definitions were evaluated: conventional dichotomization (hs-TnT ≥14 pg/mL) and sex-specific classification. Sex-specific hs-TnT cut-offs were derived using receiver operating characteristic (ROC) analysis for long-term all-cause mortality, selecting the threshold maximizing the Youden index (hereafter referred to as sex-specific hs-TnT cut-offs).
The primary endpoint was long-term all-cause mortality. Vital status was established via the Romanian Public Healthcare Insurance System database, queried in August 2024. Follow-up time was calculated from the index hospitalization date to death. Patients who were still alive at the time of database query were treated as censored at their last recorded follow-up date.
Time-to-event was analyzed in years. For prespecified landmark analyses, follow-up was partitioned into an early window (≤1 year) and a late window (>1 year).
Potential selection bias was minimized by using a consecutive hospital-based registry and prespecified eligibility criteria consistent with the parent HI-HF cohort. Information bias was limited by extracting baseline clinical and comorbidity data from electronic health records and by using standardized laboratory assays and in-hospital echocardiography. Confounding was addressed through prespecified multivariable models incorporating key markers of heart failure severity and renal function, and by formal testing of sex × troponin interactions. To account for non-proportional hazards, time-dependent covariates and a prespecified 1-year landmark approach were applied. Residual confounding cannot be excluded given the observational design.
Data processing was performed using IBM SPSS Statistics version 20 (IBM Corp. in Armonk, NY) and MedCalc version 23.5.2. A p value <0.05 was considered statistically significant.
Continuous variables were summarized as mean±standard deviation (SD) if normally distributed, otherwise as median and interquartile range (IQR). Categorical variables were reported as absolute numbers and percentages (n, %). Group comparisons used χ2 or Fisher’s exact test (categorical) and Mann-Whitney U test (continuous, non-Gaussian).
Sex-specific cut-off values for hs-TnT were determined from the ROC analysis using Youden index associated criterion for the optimal sensitivity (Se) and specificity (Sp) association.
Unadjusted survival was described by Kaplan-Meier curves and compared using the log-rank test. Associations between hs-TnT cut-offs and mortality were quantified using Cox proportional hazards models, reporting hazard ratios (HRs) with 95% confidence intervals (CIs).
Multivariable Cox models were prespecified to adjust for clinically relevant confounders and HF severity markers: age, sex, LVEF, eGFR, NT-proBNP, atrial fibrillation, NYHA class, hypertension, and obesity. Troponin was then introduced as the exposure of interest in adjusted models (sex-specific hs-TnT cut-offs). NT-proBNP was log-transformed (ln(NT-proBNP)).
Effect modification by sex was evaluated using multiplicative interaction terms (sex×traditional hs-TnT; sex× sex-specific hs-TnT cut-offs) in fully adjusted models. Sex-stratified effects were interpreted from the combined coefficients. Forward, backward and stepwise methodology was used to ensure optimal selection of the independent associations.
The proportional hazards assumption for troponin definitions was assessed using extended Cox models with time-dependent covariates constructed as biomarker×ln(time); to avoid ln(0), time was offset by a small constant prior to transformation. Given evidence of time-varying effects, we performed a prespecified 1-year landmark (piecewise) Cox analysis, estimating early (≤1 year) and late (>1 year) associations.
The study is reported in accordance with the STROBE statement (see Supplementary table 1).
Generative AI tools were used solely for language support (translation and occasional paraphrasing) to improve clarity, grammar, and scientific style. These tools were not used for study conception, design, data extraction, statistical analyses, results generation, interpretation, or formulation of conclusions. All scientific content was produced, verified, and approved by the authors, who assume full responsibility for the accuracy and integrity of the work.
The study included 404 patients, 54.7% women. Median follow-up time from index hospitalization to death or censoring was 5.72 [3.38–6.87] years. During follow-up, 149 deaths (36.9%) occurred, with no difference in all-cause mortality by sex.
Baseline characteristics are summarized in Table 1. Women were older than men (74.24±8.93 vs 69.00±10.61 years; p<0.001) and had higher LVEF (44.59±11.54 vs 39.12±12.91%; p<0.001). Median hs-TnT was lower in women than in men (14.18 [9.21–25.25] vs 22.44 [12.77–33.53] pg/mL, p<0.001). Heart failure phenotype differed by sex, with HFrEF being more frequent in men and HFpEF more frequent in women (p<0.001). Men had higher prevalences of COPD, ischemic heart disease, and prior myocardial infarction, whereas thyroid dysfunction was more frequent in women (Table 1).
General characteristics for male and female patients
| Demographics and risk factors | Entire group (n=404) | Female (n=221) | Male (n=183) | p value* |
|---|---|---|---|---|
| General characteristics | ||||
| Age (years) | 71.87 (±10.06) | 74.24 (±8.93) | 69.00 (±10.61) | <0.001 |
| Systolic BP (mmHg) | 144.77 (±29.14) | 147.29 (±30.53) | 141.80 (±27.21) | 0.077 |
| Diastolic BP (mmHg) | 81.39 (±13.62) | 82.44 (±13.59) | 80.15 (±13.60) | 0.115 |
| Heart rate (bpm) | 85.01 (±25.63) | 85.60 (±26.32) | 84.28 (±24.79) | 0.624 |
| Heart failure characteristics | ||||
| HFrEF | 129 (31.9%) | 50 (22.6%) | 79 (43.2%) | <0.001 |
| HFmrEF | 121 (30.0%) | 69 (31.2%) | 52 (28.4%) | |
| HFpEF | 152 (37.6%) | 102 (46.2%) | 50 (27.3%) | |
| NYHA class III | 243 (60.1%) | 134 (60.6%) | 109 (59.6%) | 0.827 |
| NYHA class IV | 58 (14.5%) | 32 (14.5%) | 26 (14.5%) | 0.995 |
| Hospitalization outcome | ||||
| Length of stay (days) | 6.00 [5.00–8.00] | 6.00 [4.00–8.00] | 6.00 [5.00–9.75] | 0.498 |
| Extended stay | 97 (24.1%) | 45 (20.5%) | 52 (28.4%) | 0.066 |
| All causes mortality | 149 (36.9%) | 78 (35.3%) | 71 (38.8%) | 0.467 |
| Comorbidities and risk factors | ||||
| Arterial Hypertension | 325 (80.4%) | 184 (83.3%) | 141 (77.0%) | 0.117 |
| COPD | 19 (4.7%) | 3 (1.4%) | 16 (8.7%) | <0.001 |
| History of stroke | 49 (12.1%) | 29 (13.1%) | 20 (10.9%) | 0.501 |
| Atrial fibrillation | 191 (47.3%) | 104 (47.1%) | 87 (47.5%) | 0.923 |
| Ischemic heart disease | 176 (43.6%) | 85 (38.5%) | 91 (49.7%) | 0.023 |
| Prior myocardial infarction | 106 (26.2%) | 38 (17.2%) | 68 (37.2%) | <0.001 |
| Chronic kidney disease | 229 (56.7%) | 130 (58.8%) | 99 (54.1%) | 0.340 |
| Type 2 Diabetes Mellitus | 131(32.4%) | 71 (32.1%) | 60 (32.8%) | 0.888 |
| Obesity | 177 (43.8%) | 103 (46.6%) | 74 (40.4%) | 0.213 |
| Thyroid dysfunction | 36 (8.9%) | 30 (13.6%) | 6 (3.3%) | 0.003 |
| Echocardiographic characteristics | ||||
| LVEF (%) | 42.06 (±12.48) | 44.59 (±11.54) | 39.12 (±12.91) | <0.001 |
| Severe aortic stenosis | 6 (1.5%) | 4 (1.8%) | 2 (1.1%) | 0.553 |
| Severe aortic regurgitation | 5 (1.2%) | 3 (1.4%) | 2 (1.1%) | 0.811 |
| Severe mitral regurgitation | 57 (14.1%) | 32 (14.5%) | 25 (13.7%) | 0.814 |
| Pulmonary hypertension | 195 (48.3%) | 110 (49.8%) | 85 (46.4%) | 0.505 |
| Pericardial effusion | 27 (6.7%) | 18 (8.1%) | 9 (4.9%) | 0.196 |
| Aortic atheromatosis | 151 (37.4%) | 95 (43.0%) | 56 (30.6%) | 0.036 |
| Biological characteristics | ||||
| Hemoglobin (g/dL) | 13.13 (±1.91) | 12.61 (±1.70) | 13.77 (±1.98) | <0.001 |
| ESR (mm/h) | 19.00 [8.75–34.00] | 20.50 [10.00–33.25] | 17.50 [7.00–34.00] | 0.020 |
| Serum Na (mmol/L) | 139.65 (±7.94) | 140.05 (±4.56) | 139.15 (±10.75) | 0.262 |
| Serum K (mmol/L) | 4.36 (±0.50) | 4.34 (±0.55) | 4.38 (±0.43) | 0.469 |
| eGFR (ml/min/1.73m2) | 71.92 [55.06–88.75] | 66.16 [49.09–84.39] | 78.29 [57.35–89.37] | 0.026 |
| Glycemia (mg/dL) | 107.50 [94.00–134.50] | 111.50 [98.00–139.25] | 105.00 [88.75–126.75] | 0.401 |
| Total cholesterol (mg/dL) | 163.80 [137.00–207.25] | 172.75 [140.75–223.15] | 155.00 [127.35–190.75] | 0.010 |
| AST (UI/L) | 21.50 [17.47–28.57] | 21.00 [17.07–28.22] | 21.60 [17.62–28.72] | 0.264 |
| ALT (UI/L) | 18.10 [14.00–26.15] | 17.50 [13.45–24.85] | 19.90 [14.12–31.55] | 0.030 |
| NT-proBNP (ng/L) | 1687.50 [622.20–4319.75] | 1607.50 [504.62–3860.75] | 1777.50 [766.77–4859.00] | 0.595 |
| hs-TnT (pg/mL) | 17.06 [10.43–29.42] | 14.18 [9.21–25.25] | 22.44 [12.77–33.53] | <0.001 |
Note: *for comparison of female with male patients
Abbreviations: BP – blood pressure; HFrEF – heart failure with reduced ejection fraction; HFmrEF – heart failure with mid-range ejection fraction; HFpEF – heart failure with preserved ejection fraction; COPD – Chronic obstructive pulmonary disease; LVEF – left ventricular ejection fraction; ESR – erythrocyte sedimentation rate; eGFR – estimated glomerular filtration rate; AST – aspartate aminotransferase; ALT – alanine aminotransferase; hsTnT – high-sensitivity troponin T.
Men had higher median hs-TnT levels compared to women (17.96 [10.46–30.07] pg/mL versus 13.08 [8.74 – 21.32] pg/mL, p<0.001; Figure 2).
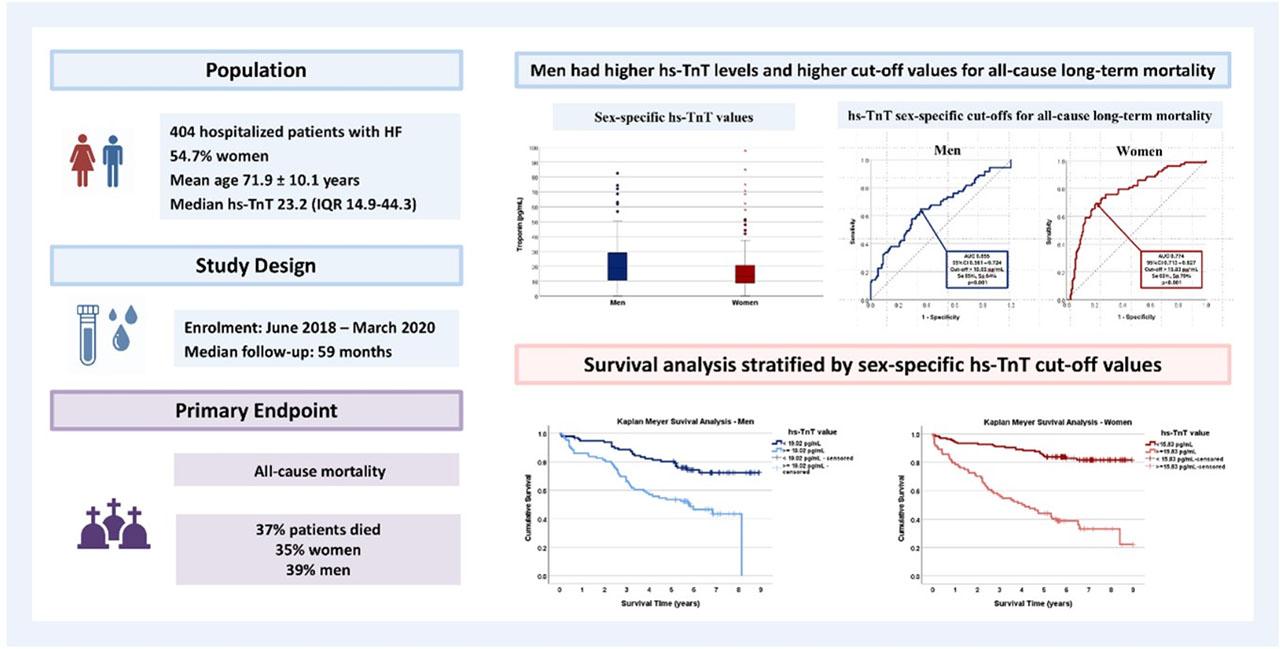
Central illustration. Derivation of sex-specific hs-TnT cut-off values and their implementation in survival analysis.
hs-TnT was associated with all-cause mortality for both genders, with a stronger correlation for women than men (AUC 0.774, 95%CI 0.713–0.827, p<0.001 versus AUC 0.655, 95%CI 0.581–0.724, p < 0.001). In ROC analysis for the association with the survival outcome, the hs-TnT cut-off for men was higher than for women (Figure 2), both cut-offs surpassing the conventional upper limit of normal of 14 pg/mL. We further defined increased hs-TnT levels for each gender using these cut-offs, respectively hs-TnT >19.02 pg/mL for men and hs-TnT > 15.83 pg/mL for women. 46.99% men had hs-TnT>19.02 pg/mL and 38.01% women had hs-TnT > 15.83 pg/mL.
When analyzing subgroups of LVEF, the cut-off for hs-TnT correlated with all-cause mortality were similar for women with LVEF < 50% and those with LVEF ≥ 50% (Supplementary Table 2). For men, however, the cut-off associated with the outcome was significantly higher for those with LVEF < 50% compared to those with LVEF ≥ 50% (Supplementary Table 2).
In univariable analysis, most predictors of elevated hs-TnT levels were mutual for men and women: age, NYHA class, clinical congestion, LVEF, estimated pulmonary artery systolic pressure (PASP), severe mitral regurgitation, NT-proBNP, hemoglobin levels, kidney function estimated by the glomerular filtration rate (eGFR) (Table 2). Severe tricuspid regurgitation, serum sodium levels and glycemia were correlated with increased hs-TnT only for women (Table 2).
Baseline characteristics for outcome sex-specific hs-TnT cut-off groups in men and women
| A. Categorical variables | ||||||||
|---|---|---|---|---|---|---|---|---|
| Men | Women | |||||||
| Variable | hs-TnT <19.02 pg/mL n (%) | hs-TnT ≥19.02 pg/mL n (%) | OR (95% CI) | p | hs-TnT <15.83 pg/mL n (%) | hs-TnT ≥15.83 pg/mL n (%) | OR (95% CI) | p |
| Heart failure characteristics | ||||||||
| NYHA III and IV | 38 (39.20%) | 55 (64.00%) | 2.75 (1.51–5.03) | 0.001 | 66 (48.18%) | 60 (71.43%) | 2.69 (1.51–4.80) | 0.001 |
| Clinical congestion | 25 (25.80%) | 48 (55.80%) | 3.64 (1.95–6.78) | <0.0 01 | 39 (28.47%) | 45 (53.57%) | 2.90 (1.64–5.11) | <0.0 01 |
| Hospitalization outcome | ||||||||
| Extended stay (>7 days) | 16 (16.50%) | 36 (41.90%) | 3.65 (1.84–7.24) | <0.0 01 | 12 (8.76%) | 33 (40.24%) | 7.02 (3.35–14.68) | <0.0 01 |
| Comorbidities and risk factors | ||||||||
| Hypertension | 76 (78.40%) | 65 (75.60%) | 0.86 (0.43–1.70) | 0.657 | 117 (85.40%) | 67 (79.76%) | 0.67 (0.33–1.37) | 0.276 |
| COPD | 9 (9.30%) | 7 (8.10%) | 0.87 (0.31–2.44) | 0.785 | 0 (0.00%) | 3 (3.57%) | Not estimable | 0.054* |
| Prior stroke | 7 (7.20%) | 13 (15.10%) | 2.29 (0.87–6.04) | 0.087 | 15 (10.95%) | 14 (16.67%) | 1.63 (0.74–3.57) | 0.222 |
| Atrial fibrillation | 45 (46.40%) | 42 (48.80%) | 1.10 (0.62–1.97) | 0.741 | 59 (43.07%) | 45 (53.57%) | 1.53 (0.88–2.63) | 0.129 |
| Ischemic heart disease | 51 (52.60%) | 40 (46.50%) | 0.78 (0.44–1.40) | 0.413 | 53 (38.69%) | 32 (38.10%) | 0.98 (0.56–1.71) | 0.930 |
| Prior myocardial infarction | 36 (37.10%) | 32 (37.20%) | 1.00 (0.55–1.83) | 0.989 | 22 (16.06%) | 16 (19.05%) | 1.23 (0.60–2.50) | 0.568 |
| Type 2 diabetes | 30 (30.90%) | 30 (34.90%) | 1.20 (0.65–2.22) | 0.569 | 39 (28.47%) | 32 (38.10%) | 1.55 (0.87–2.75) | 0.137 |
| Obesity | 42 (43.30%) | 32 (37.20%) | 0.78 (0.43–1.40) | 0.402 | 69 (50.36%) | 34 (40.48%) | 0.67 (0.39–1.16) | 0.15 3 |
| Peripheral artery disease | 11 (11.30%) | 10 (11.60%) | 1.03 (0.41–2.56) | 0.951 | 7 (5.11%) | 5 (5.95%) | 1.18 (0.36–3.83) | 0.769* |
| Chronic kidney disease | 41 (42.30%) | 58 (67.40%) | 2.83 (1.55–5.18) | 0.001 | 64 (46.72%) | 66 (78.57%) | 4.18 (2.25–7.77) | <0.0 01 |
| Echocardiographic characteristics | ||||||||
| Severe aortic stenosis | 1 (1.00%) | 1 (1.20%) | 1.13 (0.07–18.34) | 1.000* | 0 (0.00%) | 4 (4.76%) | Not estimable | 0.020* |
| Severe aortic regurgitation | 0 (0.00%) | 2 (2.30%) | Not estimable | 0.219* | 0 (0.00%) | 3 (3.57%) | Not estimable | 0.054* |
| Severe mitral regurgitation (grade 3–4) | 8 (8.20%) | 17 (19.80%) | 2.74 (1.12–6.72) | 0.024 | 10 (7.30%) | 22 (26.19%) | 4.51 (2.01–10.10) | <0.001 |
| Severe tricuspid regurgitation | 9 (9.30%) | 13 (15.10%) | 1.74 (0.70–4.30) | 0.226 | 13 (9.49%) | 22 (26.19%) | 3.38 (1.60–7.17) | 0.001 |
| Pulmonary hypertension | 36 (37.10%) | 49 (57.00%) | 2.24 (1.24–4.06) | 0.007 | 58 (42.34%) | 52 (61.90%) | 2.21 (1.27–3.86) | 0.005 |
| Pericardial effusion | 5 (5.20%) | 4 (4.70%) | 0.90 (0.23–3.46) | 1.000* | 8 (5.84%) | 10 (11.90%) | 2.18 (0.82–5.76) | 0.110 |
| Biological characteristics | ||||||||
| eGFR <60 mL/min/1.73 m2 | 15 (15.50%) | 37 (43.00%) | 4.13 (2.06–8.28) | <0.001 | 34 (24.82%) | 47 (55.95%) | 3.85 (2.16–6.87) | <0.001 |
| B. Continuous variables | ||||||
|---|---|---|---|---|---|---|
| Men | Women | |||||
| Variable | hs-TnT <19.02 pg/mL | hs-TnT ≥19.02 pg/mL | p | hs-TnT <15.83 pg/mL median [Q1–Q3] | hs-TnT ≥15.83 pg/mL median [Q1–Q3] | p |
| General characteristics | ||||||
| Age (years) | 66.00 [60.00–74.50] | 73.00 [62.00–79.00] | 0.006 | 73.00 [65.00–78.00] | 79.00 [74.25–83.00] | <0.001 |
| Hospitalization outcome | ||||||
| Length of stay (days) | 5.00 [4.00–7.00] | 7.00 [4.75–10.00] | <0.001 | 5.00 [4.00–6.00] | 7.00 [5.00–10.00] | <0.001 |
| Echocardiographic characteristics | ||||||
| LVEF / EF (%) | 46.00 [36.00–52.00] | 35.00 [25.00–45.00] | <0.001 | 50.00 [43.50–54.00] | 43.50 [33.75–50.00] | <0.001 |
| PAPS (mmHg) | 35.00 [28.00–43.00] | 42.00 [34.00–57.25] | 0.003 | 35.00 [27.00–40.00] | 45.00 [32.50–55.00] | <0.001 |
| Biological characteristics | ||||||
| Hemoglobin (g/dL) | 14.30 [13.08–15.12] | 13.60 [11.98–14.90] | 0.025 | 13.00 [12.10–13.90] | 11.92 [10.82–13.40] | <0.001 |
| ESR (mm/h) | 16.00 [6.00–27.00] | 18.00 [6.00–35.00] | 0.435 | 19.00 [10.00–30.50] | 23.00 [12.50–48.00] | 0.061 |
| Sodium (mmol/L) | 141.00 [138.00–142.00] | 140.00 [137.00–142.00] | 0.527 | 141.00 [139.00–143.00] | 140.00 [137.00–143.00] | 0.017 |
| Potassium (mmol/L) | 4.39 [4.05–4.74] | 4.32 [4.05–4.60] | 0.444 | 4.39 [3.98–4.66] | 4.36 [3.93–4.74] | 0.990 |
| Creatinine (mg/dL) | 0.94 [0.85–1.10] | 1.10 [0.90–1.43] | <0.001 | 0.80 [0.70–0.93] | 0.97 [0.80–1.27] | <0.001 |
| eGFR (ml/min/1.73m2) | 83.19 [66.95–92.72] | 64.86 [47.74–84.76] | <0.001 | 74.86 [59.86–92.14] | 55.83 [40.20–73.13] | <0.001 |
| Glycemia (mg/dL) | 104.00 [91.00–119.50] | 106.50 [94.00–126.75] | 0.496 | 101.00 [90.00–124.50] | 117.00 [101.50–150.50] | 0.001 |
| logBNP | 2.89 [2.54–3.13] | 3.40 [2.97–3.79] | <0.001 | 2.89 [2.56–3.26] | 3.46 [3.01–3.83] | <0.001 |
Abbreviation: hs-TnT – high-sensitivity troponin T; OR – odds ratio; CI – confidence interval; Q1–Q3 – interquartile range; COPD – chronic obstructive pulmonary disease; eGFR – estimated glomerular filtration rate; LVEF – left ventricular ejection fraction; PAPS – pulmonary artery systolic pressure; ESR – erythrocyte sedimentation rate.
In multivariable analysis, the independent predictors of elevated hs-TnT in men were the signs of clinical congestion, NT-proBNP levels, LVEF and eGFR (Table 3). The independent predictors of elevated hs-TnT in women were age, NT-proBNP levels and eGFR (Table 3).
Independent parameters associated with increased hs-TnT – Multivariable analysis
| Men hs-TnT ≥ 19.02 pg/mL | Women hs-TnT ≥ 15.83 pg/mL | ||||
|---|---|---|---|---|---|
| HR* (95%CI) | p value | HR** (95%CI) | p value | ||
| Clinical congestion | 2.24 (1.16–5.07) | 0.019 | Age | 1.08 (1.02–1.14) | 0.005 |
| LnNT-proBNP | 3.30 (1.42–7.67) | 0.005 | LnNT-proBNP | 4.22 (2.02–8.81) | < 0.001 |
| eGFR | 0.97 (0.95–0.99) | 0.001 | eGFR | 0.98 (0.96–0.99) | 0.016 |
| LVEF | 0.96 (0.93–0.99) | 0.027 | |||
Note: *Adjusted for age, NYHA class, chronic obstructive pulmonary disease, chronic kidney disease, severe mitral regurgitation, estimated pulmonary artery systolic pressure, hemoglobin – variables without independent correlation with increased hs-TnT
Note: **Adjusted for NYHA class, clinical congestion, chronic obstructive pulmonary disease, chronic kidney disease, LVEF, severe aortic stenosis, severe mitral regurgitation, severe tricuspid regurgitation, estimated pulmonary artery systolic pressure, hemoglobin, serum sodium, glycemia – variables without independent correlation with increased hs-TnT
Men and women had similar survival (log-rank χ2=0.515, p=0.473).
Using the conventional hs-TnT upper limit of normal, men with hs-TnT > 14 pg/mL had a risk ratio of all-cause long-term mortality of 1.37 (95%CI 1.10–1.72, p = 0.01) compared to those with hs-TnT < 14 pg/mL. Using the cut-off of hs-TnT ≥ 19.02 pg/mL the risk stratification was improved to 1.60 (95%CI 1.24–2.06, p< 0.001). Women with hs-TnT > 14 pg/mL had a risk ratio of all-cause long-term mortality of 2.09 (95%CI 1.63–2.69, p < 0.001) compared to those with hs-TnT < 14 pg/mL. Using the cut-off of hs-TnT ≥ 15.83 pg/mL the risk stratification was improved to 2.31 (95%CI 1.72–3.11, p< 0.001).
For both sexes, troponin levels were correlated with survival. The Kaplan-Meyer analysis using the sex-specific hs-TnT cut-offs showed significantly better survival in men with hs-TnT < 19.02 pg/mL compared to those with hs-TnT ≥ 19.02 pg/mL (7.36, 95%CI 6.82–7.91 years versus 5.14, 95%CI 4.48–5.79 years, log-rank χ2=16.406, p<0.001), as well as in women with hs-TnT < 15.83 pg/mL compared to those with hs-TnT ≥ 15.83 pg/mL (7.85, 95%CI 7.43–8.26 years versus 4.62, 95%CI 3.87–5.35 years, log-rank χ2=59.174, p<0.001) (Figure 2).
We further divided each gender-based group into three subgroups using the hs-TnT sex-specific and out-come specific cut-offs as well as the conventional cut-off of 14 pg/mL. Women with hs-TnT < 14 pg/mL had the best outcome, and those with hs-TnT has the worst outcome. Women with hs-TnT between 14–15.83 pg/mL had similar all-cause mortality as those with hsTnT ≥ 15.83 pg/mL only during the first year of follow-up, after which the three survival curves were significantly separated (Figure 3). Men with hs-TnT between 14–19.02 pg/mL had similar prognosis as those with hs-TnT < 14 pg/mL, significantly better than those with hs-TnT > 19.02 pg/mL (Figure 3).
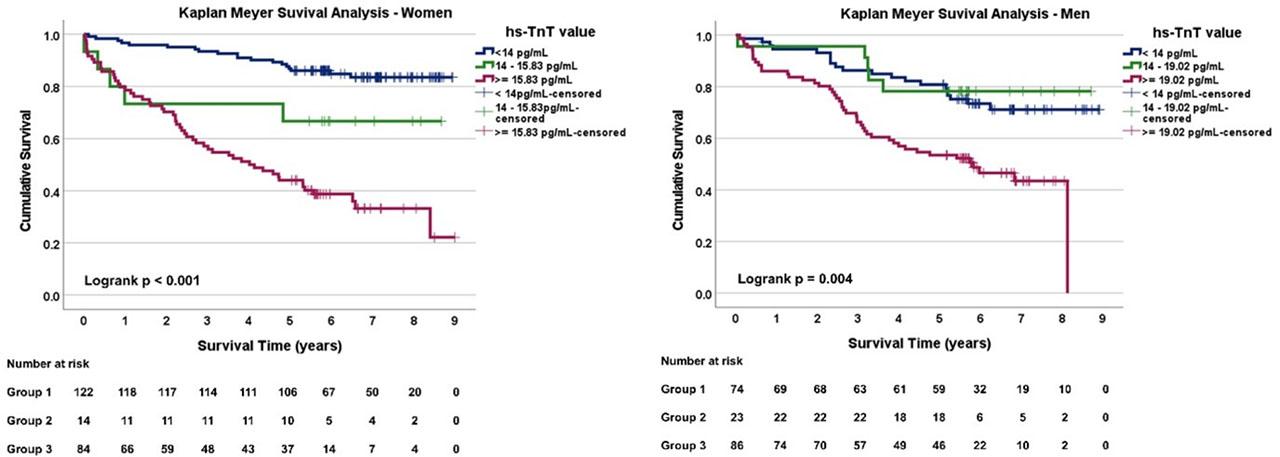
Survival analysis stratified by hs-TnT values for A – Women, and B – Men.
Univariable Cox analysis identified the clinical, laboratory and echocardiographic parameters associated with mortality for each sex-based group (Table 4). These parameters were then included in the multivariable Cox analysis to determine the independent predictors of all-cause mortality.
Univariate Cox regression for all-cause mortality – comparison across groups
| Predictor | Men | Women | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| General characteristics | ||||||
| Age (per 1 year) | 1.03 | 1.01–1.05 | 0.013 | 1.08 | 1.05–1.11 | <0.001 |
| Heart failure characteristics | ||||||
| NYHA III and IV | 1.82 | 1.13–2.94 | 0.014 | 2.14 | 1.32–3.49 | 0.002 |
| Clinical congestion | 1.74 | 1.09–2.77 | 0.020 | 1.87 | 1.20–2.92 | 0.006 |
| Cardiovascular risk factors and comorbidities | ||||||
| HTN | 0.76 | 0.45–1.28 | 0.298 | 0.63 | 0.37–1.09 | 0.097 |
| Atrial fibrillation | 1.32 | 0.83–2.11 | 0.240 | 1.96 | 1.24–3.08 | 0.004 |
| Prior stroke | 1.47 | 0.75–2.88 | 0.258 | 1.09 | 0.58–2.06 | 0.797 |
| IHD | 1.14 | 0.72–1.82 | 0.580 | 0.77 | 0.48–1.23 | 0.270 |
| Prior MI | 1.36 | 0.85–2.18 | 0.203 | 0.91 | 0.50–1.65 | 0.759 |
| Type 2 diabetes | 0.82 | 0.49–1.37 | 0.444 | 1.24 | 0.78–1.97 | 0.358 |
| CKD | 1.78 | 1.09–2.89 | 0.021 | 2.31 | 1.40–3.81 | 0.001 |
| Obesity | 0.46 | 0.27–0.77 | 0.003 | 0.54 | 0.34–0.86 | 0.009 |
| Echocardiographic characteristics | ||||||
| LVEF (per 1%) | 0.97 | 0.95–0.99 | <0.001 | 0.96 | 0.95–0.98 | <0.001 |
| ePASP (per 1mmHg) | 1.03 | 1.01–1.05 | 0.002 | 1.03 | 1.01–1.05 | 0.004 |
| Severe MR | 2.08 | 1.16–3.73 | 0.015 | 2.34 | 1.39–3.93 | 0.001 |
| Severe TR | 1.71 | 0.89–3.26 | 0.10 | 2.61 | 1.58–4.32 | <0.001 |
| Severe AS | 1.59 | 0.22–11.47 | 0.65 | 2.21 | 0.69–7.02 | 0.18 |
| Biological characteristics | ||||||
| hs-TnT sex-specific cut-off | 2.66 | 1.62–4.34 | <0.001 | 5.50 | 3.38–8.94 | <0.001 |
| hs-TnT ≥14 pg/mL | 2.11 | 1.26–3.56 | 0.005 | 5.66 | 3.36–9.53 | <0.001 |
| lnNTproBNP (per 1 unit) | 1.57 | 1.31–1.88 | <0.001 | 1.58 | 1.34–1.87 | <0.001 |
| eGFR (per 1 mL/min/1.73m2) | 0.99 | 0.98–1.00 | 0.033 | 0.98 | 0.97–0.99 | 0.001 |
| Hemoglobin (per 1 g/dL) | 0.80 | 0.72–0.89 | <0.001 | 0.89 | 0.78–1.00 | 0.056 |
| Serum Na (per 1mmol/L) | 0.99 | 0.98–1.02 | 0.91 | 0.96 | 0.91–1.00 | 0.053 |
| Serum K (per 1 mmol/mL) | 0.89 | 0.51–1.55 | 0.67 | 1.42 | 0.94–2.14 | 0.092 |
Abbreviations: AS – aortic stenosis; CKD – chronic kidney disease; ePASP – estimated pulmonary artery systolic pressure; HTN – arterial hypertension; IHD – ischemic heart disease; LVEF – left ventricular ejection fraction; MI – myocardial infarction; MR – mitral regurgitation; TR – tricuspid regurgitation.
Hemoglobin and NT-proBNP levels were independently correlated with the outcome in men. Adding hs-TnT ≥ 19.02 pg/mL increased the predictive performance of the model (Figure 4) and proved its independent predictive value (Table 5). Age and NT-proBNP levels were independently correlated with the outcome in women. Adding hs-TnT ≥ 15.83 pg/mL increased the predictive performance of the model (Figure 4) and proved its independent predictive value (Table 5).
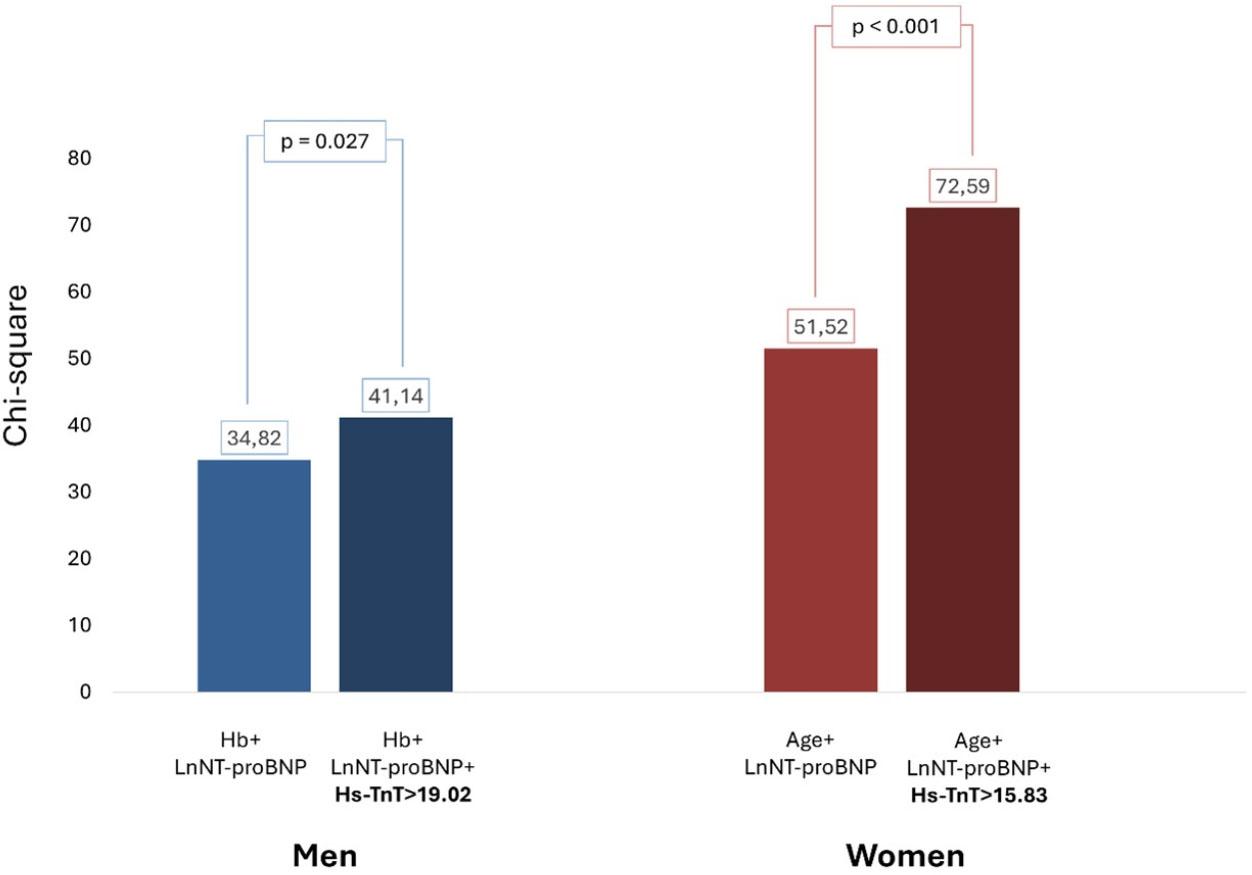
Hierarchical Cox Regression Analysis showing the incremental clinical value of sex-specific increased hs-TnT.
Stepwise multivariable Cox analysis for all-cause long-term mortality
| Independent predictors for all-cause long-term mortality | |||||
|---|---|---|---|---|---|
| Men | Women | ||||
| HR* (95%CI) | p value | HR** (95%CI) | p value | ||
| Hemoglobin (per 1g/dL) | 0.88 (0.78–0.98) | 0.021 | Age (per 1 year) | 1.05 (1.02–1.09) | 0.003 |
| LnNT-proBNP (per 1 unit) | 1.28 (1.03–1.59) | 0.025 | LnNT-proBNP (per 1 unit) | 1.22 (1.01–1.47) | 0.035 |
| hs-TnT ≥ 19.02 pg/mL | 1.91 (1.07–3.41) | 0.029 | hs-TnT ≥ 15.83 pg/mL | 3.54 (2.07–6.07) | < 0.001 |
Note: *Adjusted for NYHA class, clinical congestion, atrial fibrillation, chronic kidney disease, obesity, age, LVEF, estimated pulmonary artery systolic pressure, severe mitral regurgitation, severe tricuspid regurgitation – variables without independent prognostic value in the final steps of the regression
Note: **Adjusted for NYHA class, clinical congestion, atrial fibrillation, chronic kidney disease, obesity, LVEF, estimated pulmonary artery systolic pressure, severe mitral regurgitation, severe tricuspid regurgitation, severe aortic stenosis, serum sodium, hemoglobin – variables without independent prognostic value in the final steps of the regression
Time-dependent Cox analyses showed that the prognostic effect of hs-TnT was not constant over follow-up (p<0.001 for time interaction for both the conventional threshold and the sex-specific cut-off). A prespecified 1-year landmark analysis was therefore performed. Within the first year, neither hs-TnT category nor its interaction with sex was significant. Beyond 1 year (among 1-year survivors; n=341, 101 deaths), sex modified the troponin-mortality association for both approaches (sex×hs-TnT: HR 3.05, 95% CI 1.25-7.43; p=0.014; sex×sex-specific cut-off: HR 2.89, 95% CI 1.22–6.82; p=0.016).
In this cohort of patients discharged alive after heart failure hospitalization that were followed-up for a median duration of 5.72 years for all-cause mortality, we found that: i) hs-TnT levels on admission were higher in men compared to women; ii) hs-TnT was correlated with all-cause long-term in both men and women; iii) sex-specific and outcome-specific cut-off values for hs-TnT improved mortality risk stratification, respectively hs-TnT ≥ 19.02 pg/mL for men and hs-TnT ≥ 15.83 pg/mL for women.
Low-grade high sensitivity troponin release is common in HF, and its prognostic use expands well beyond acute coronary syndromes [18][21][22]. It is a marker of myocardial injury and implicitly of worse outcomes in this setting, and its predictive role is supported by current HF management guidelines [2][3]. While our study concurs with this well-known data, it further highlights the utmost importance of using differentiated cut-offs of the hs-TnT for men and women.
Women have lower circulating cardiac troponin concentrations than men, even in the absence of comorbidities, and reference limits are influenced by the type of assay used as well as the populations’ baseline characteristics [23]. In this context, in the general population, a similar absolute hs-TnT value may plausibly reflect a different prognosis in women than in men, influenced by gender-specific traits such as myocardial mass or hormonal background, or subclinical cardiovascular disease [24][25]. Large population analyses suggest that, while biomarker-HF associations are broadly similar between sexes, subtle differences in predictive contribution can exist, including for troponin levels [26].
The sex-related biomarker variations found in our cohort are compatible with known differences in HF phenotypes and substrate. HFpEF and the hypertensive-metabolic HF pathways are more prevalent in women, where microvascular dysfunction, endothelial inflammation, concentric remodeling, and myocardial fibrosis are frequently involved pathophysiologically [27][28][29]. These processes therefore contribute to the prognostic value of hs-TnT levels, as it reflects diffuse microvascular dysfunction and fibrotic remodeling [30]. Renal dysfunction is another key modifier of circulating troponin and HF risk interpretation, not only by reduced renal clearance but also by its association with a higher burden of cardiac abnormalities such as the increased left ventricular pressures due to higher LV mass and more advanced diastolic dysfunction [31][32]. This is clinically relevant since cardiorenal interactions might differ by sex across HF phenotypes and comorbidity patterns [26][33]. Men with HFpEF have higher prevalence of both ischemic coronary disease and chronic kidney disease with worse cardiac and renal function compared to women, both independent predictors of increased troponin levels [32][34].
In our cohort, NT-proBNP and eGFR were independent predictors of elevated hs-TnT in both men and women, highlighting the strong correlation of myocardial injury to HF severity, as well as the bidirectional cardiorenal dependency. Clinical congestion and LVEF were independently correlated to increased hs-TnT in men, concordant with previous data linking the triad of systolic dysfunction, secondary myocardial injury and subsequent clinical congestion [35]. Age was an independent determinant of higher hs-TnT in women, coinciding with prior observations documented in the general population by de Bakker et al. They found consistently increasing hs-TnI levels with aging in women, with higher titers linked to worse outcomes in both women and men [36].
Research focusing on sex and HF biomarkers emphasized the importance of adapting and personalizing the cut-offs, keeping the prognostic sex-specificity as an open question requiring targeted validation [33]. Outcome-specific cut-off values for troponin were investigated in both acute and chronic heart failure patients and different limits were proposed for different settings [37]. Sex-specific values were studied predominantly in chronic heart failure, where the proposed cut-offs for all-cause long-term mortality span from 16 to 18 ng/L in women, and from 23 to 33 ng/L in men [10][37].
Given the data underlining the sex-related differences of troponin values as well as the unique drivers of increased biomarker levels in men and women in acute heart failure, adjusted limits for prognostic evaluation is needed in this setting. Our study is among the few to investigate the role of sex-specific cut-offs for hs-TnT as a predictor of all-cause long-term mortality of patients admitted for decompensated heart failure. Similar to the chronic setting, we proved that different reference values are useful for optimizing the long-term prognostic assessment of patients hospitalized for HF. Increased levels of high sensitivity cardiac troponins were associated with poor outcomes in stable heart failure regardless of the assay used or type of measured biomarker, however there is data suggesting that hs-TnT might have a better predictive value compared to hs-TnI in heart failure patients [19]. In our cohort, hs-TnT levels with sex-specific cut-offs improved the risk stratification for all-cause mortality by 23% in men and 22% in women, underlining the importance of using adjusted values when evaluating prognosis.
Moreover, the cut-offs derived from our analysis, respectively hs-TnT ≥ 19.02 pg/mL for men and hs-TnT ≥ 15.83 pg/mL for women were independent predictors of all-cause long-term mortality after adjustment for all other clinical, biological and echocardiographic parameters linked to the outcome. The risk of death associated with these cut-offs was higher for women than men, in concordance with previous data showing that even if troponin levels are lower in women, for the same values, the prognosis is worse for them compared to men, across different settings [37].
We also observed time-dependence of the hs-TnT and all-cause mortality association, suggesting that a single admission value may capture both acute hemodynamic stress and an underlying trajectory of chronic injury. This interpretation is consistent with evidence that serial troponin measurements and longitudinal changes add prognostic information in chronic HF and acute HF settings [38][39][40][41]. Recurrent low-level troponin elevation patterns across HF hospitalizations have also been linked to worse outcomes than intermittent patterns, supporting the concept of persistent injury phenotypes [42].
From a clinical perspective, our findings support sex-aware interpretation of hs-TnT for long-term risk profiling in hospitalized HF patients, and strengthen the need for sex-specific validated cut-offs to be used routinely in clinical practice, in addition to the natriuretic peptides, as we have proved their independent and incremental prognostic value in this setting.
We acknowledge several limitations to our study. This was a retrospective single-center study, with possible residual confounding despite prespecified adjustment. hs-TnT was measured at admission only. Serial post-discharge trajectories were not available.
The sex-specific prognostic cut-offs were internally derived and require external validation. Time-dependent and landmark approaches improve interpretability under non-proportional hazards but can reduce precision in early windows.
The primary endpoint of our study was all-cause mortality; therefore, another limitation is the lack of data on cardiovascular mortality. However, all-cause mortality is a robust endpoint frequently used in prognostic studies in heart failure, especially when the follow-up period is prolonged, like in our case.
Our cohort was hospitalized between 2011 and 2014. While this timeframe includes the restraint of former therapeutic possibilities lacking the impact of the current pillars of optimal medical therapy, it offered the possibility to extend the follow-up duration to a maximum of 9 years, which we consider a strength of our study.
Future work should externally validate sex-specific prognostic hs-TnT thresholds in contemporary multicenter HF cohorts and should quantify the incremental value beyond natriuretic peptides using discrimination and calibration metrics. Prospective studies should incorporate serial hs-TnT measurements to clarify whether sex differences reflect trajectories rather than baseline values.
Sex-specific hs-TnT analysis improved long-term all-cause mortality risk stratification in hospitalized heart failure patients. hs-TnT was higher in men with HF compared to women with the optimal cut-offs correlated with long-term all-cause mortality being hs-TnT ≥ 19.02 pg/mL for men and hs-TnT ≥ 15.83 pg/mL for women. These values had independent prognostic value in the risk stratification models for both sexes and significantly improved the predicted probability assessment.