This review provides the most comprehensive synthesis to date of early surgical mortality in acute type A aortic dissection, based on contemporary data from 17 major national and multicentre registries. It highlights significant regional variation in outcomes, driven by differences in patient profiles, health system organization and registry methodology. The findings emphasize the need for standardized reporting and expanded data collection in underrepresented regions to support meaningful global comparisons and improve care.
Acute type A aortic dissection (ATAAD) represents one of the most catastrophic cardiovascular emergencies, characterized by abrupt onset, rapid clinical deterioration, and a persistently high risk of early mortality [1,2,3]. Despite considerable advances in diagnostic imaging, surgical techniques, and perioperative care, the management of ATAAD continues to pose substantial challenges [4,5]. The condition demands immediate recognition and emergent surgical intervention, as any delay is associated with a sharp increase in mortality [4].
Contemporary management strategies are largely informed by data derived from large-scale, multicentre registries and national databases, such as the International Registry of Acute Aortic Dissection (IRAD), the German Registry for Acute Aortic Dissection Type A (GERAADA) and the Nordic Consortium for Acute Type A Aortic Dissection (NORCAAD) [1,4,6,7,8,9].
Notably, recent data suggest a gradual decline in early postoperative mortality rates over the past two decades [6,10,11,12,13]. However, significant geographic and institutional heterogeneity persists, influenced by factors such as differences in healthcare infrastructure, surgical approach and preoperative risk profiles. Understanding these disparities is essential to contextualize outcomes and to guide improvements in care delivery and health policy.
This review synthesizes the most recent evidence from major multicentre and national registries, with a focus on contemporary in-hospital and early postoperative mortality trends in ATAAD. By consolidating these data, we aim to provide a nuanced and comprehensive overview of the current prognostic landscape of ATAAD across diverse healthcare systems.
Databases Searched: we conducted a targeted literature search using the following databases: PubMed, Google Scholar, and the Cochrane Library.
Search Strategy: the search was performed using a combination of MeSH terms and free-text keywords, including: “aorta,” “acute type A,” “aortic dissection,” “in-hospital mortality,” “early mortality,” and “early outcomes.” These terms were applied individually and in various combinations to ensure broad coverage. Additional relevant studies were identified through manual screening of reference lists from key articles.
The search was last updated in March 2025 and was limited to articles published in English within the past 10 years, to reflect contemporary management practices.
Inclusion and Exclusion Criteria: We included studies that:
Reported on acute type A aortic dissection (ATAAD)
Provided quantitative data on in-hospital, 30-day, operative or 48-hour mortality
Derived data from national or multicentre registries.
We excluded:
Case reports and single-centre studies
Studies published more than 10 years ago
Studies that presented combined analyses of type A and type B aortic dissection without providing separate outcome data for type A cases.
Single-centre studies were excluded because their findings may not be broadly applicable and are more likely to reflect local practices, institutional expertise, or patient selection, rather than national or regional trends.
Screening Process and Reviewers: Titles and abstracts were screened independently by two reviewers. Full-text articles of potentially relevant studies were assessed for eligibility based on the predefined criteria. A detailed flowchart outlining the study selection process is presented in Figure 1.
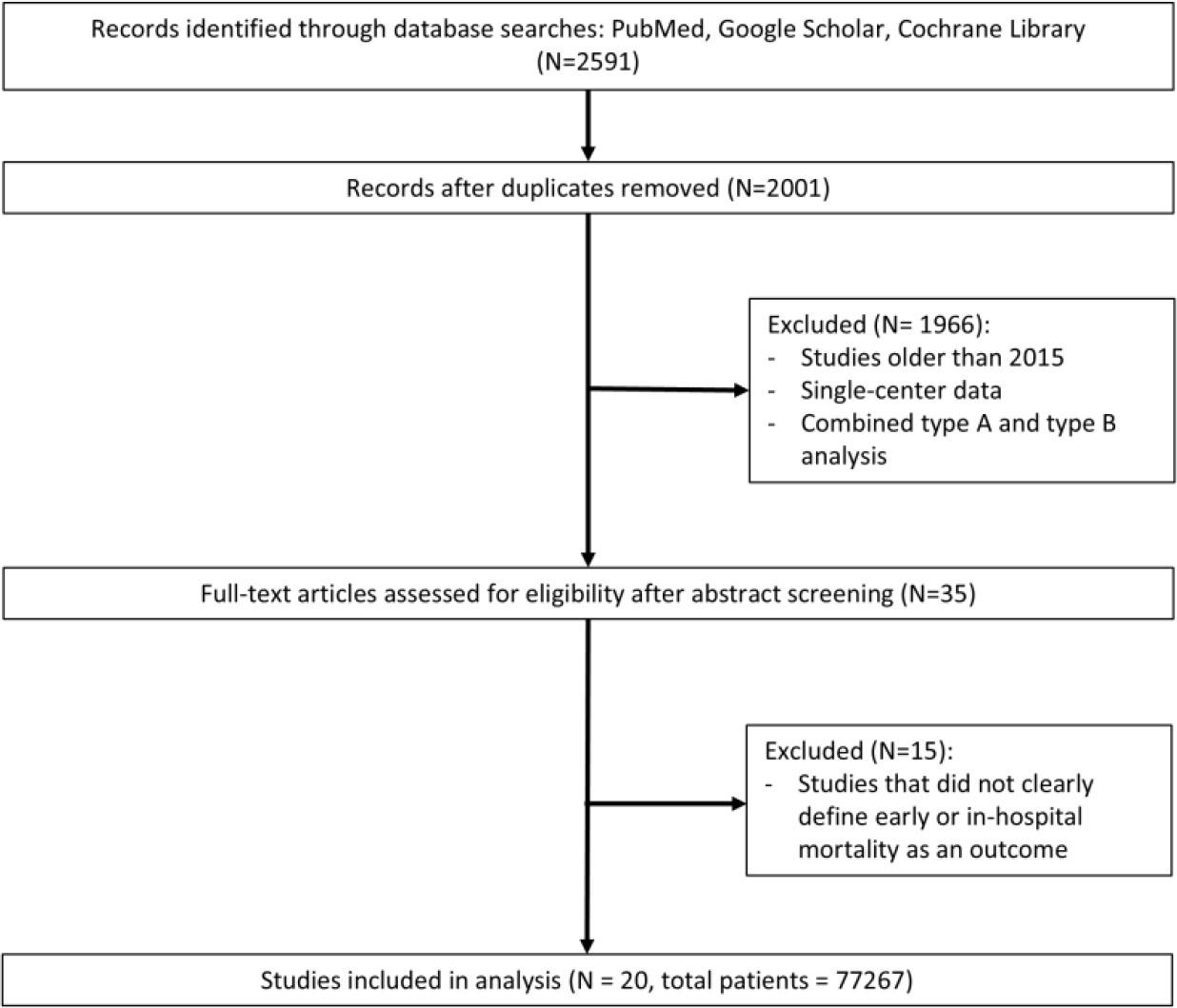
Flowchart of the Identification and Selection of Studies Reporting Mortality in Acute Type A Aortic Dissection.
Risk of Bias Assessment: Risk of bias across the included registries was assessed using a structured checklist adapted to observational and administrative datasets. The domains evaluated included: clarity of inclusion criteria, use of standardized outcome definitions, national or multicentre scope, consecutive case inclusion, completeness of data reporting and the likelihood of selection bias.
Registries based on administrative discharge data (such as the German DRG and NIS) were rated as having moderate risk of selection bias: while they capture a broad, near-complete national cohort, the reliance on ICD coding and absence of clinical validation may introduce misclassification and inconsistencies in case identification. A summary of the quality assessment is provided in Supplementary Table 1.
Meaningful cross-registry comparisons remain challenging due to differences in study design, data collection methods and outcome definitions (Table 1). Mortality outcomes and demographic profiles across the major ATAAD registries are summarized in Table 2, while the prevalence of preoperative risk factors is detailed in Table 3.
Methodological Characteristics of Contemporary ATAAD Registries
| Study | Region | Study Type | Data Source | Included |
|---|---|---|---|---|
| 14 countries | retrospective analysis of prospectively collected data | standardized case report forms (350 variables) | AAD – tertiary referral centres | |
| 8 european countries | retrospective analysis of prospectively collected data | standardized case report forms | Surgically treated ATAAD – referral centres | |
| Denmark, Finland, Iceland, Sweden | retrospective analysis of prospectively collected data | standardized case report forms (194 variables) | Surgically treated ATAAD – referral centres | |
| Austria, Switzerland, Germany | prospective | standardized case report forms (90 parameters) | Surgically treated ATAAD |
| Germany | retrospective | ICD-10 codes & other codes | Surgically treated AAD – nationwide coverage |
| Denmark | retrospective | ICD-10 codes & other codes (linked 4 different registries) | Acute Aortic Dissection – nationwide coverage | |
| Netherlands | retrospective analysis of prospectively collected data | standardized case report forms + mortality data via ICD-10 codes | Surgically treated AAD – nationwide coverage |
| Romania | retrospective analysis of prospectively collected data | standardized case report forms | ATAAD – referral centres |
| UK | retrospective analysis of prospectively collected data | standardized case report forms | Surgically treated ATAAD – referral centres |
| USA | retrospective | ICD-10 codes | Surgically treated ATAAD – nationwide coverage |
| USA | retrospective analysis of prospectively collected data | standardized case report forms (>260 variables) | Surgically treated ATAAD – nationwide coverage |
| Japan | retrospective analysis of prospectively collected data | standardized case report forms (255 variables) | Surgically treated AAD – nationwide coverage |
| Japan | retrospective | standardized case report forms (162 variables) | AAD – referral centres |
| Japan | retrospective | ICD-10 codes | AAD – nationwide coverage |
| China | retrospective analysis of prospectively collected data | standardized case report forms | Surgically treated ATAAD – referral centres |
| China | retrospective analysis of prospectively and retrospectively collected data | standardized case report forms | ATAAD and ATAIMH – referral centres |
| Australia and New Zealand | retrospective | standardized case report forms | Surgically treated ATAAD |
AAD – acute aortic dissection, ANZSCTS – Australian and New Zealand Society of Cardiac and Thoracic Surgeons, ATAAD – acute type A aortic dissection, ATAIMH – acute type A intramural hematoma, ERTAAD – European Registry of Type A Aortic Dissection, GERAADA – German Registry for Acute Aortic Dissection Type A, ICD-10 – International Classification of Diseases, 10th Revision, IRAD – International Registry of Acute Aortic Dissection, JROAD-DPC – Japanese Registry of All Cardiac and Vascular Diseases–Diagnostic Procedure Combination, JRAD – Japan Registry of Acute Aortic Dissection, NORCAAD – Nordic Consortium for Acute Type A Aortic Dissection, RENADA-RO – Romanian National Registry of Aortic Dissections, Sino-RAD – Chinese Registry of Aortic Dissection, STS – Society of Thoracic Surgeons
Mortality Outcomes and Demographic Profiles Across Major ATAAD Registries
| Study | N | Years | Age | Female Gender | Surgical Mortality | Medically Managed / Mortality |
|---|---|---|---|---|---|---|
| 5611 | 1996 – 2018 | 60.4± 14.1 | 32.9% | 48h 4.4% | 8.6 % / 23.7% |
| 2952 | 1996 – 2016 | in-hospital 25% → 18%* | 14% / 57% | ||
| 2477 | 2005 – 2021 | 63.5± 13.1 | 31% | in-hospital 18.2% | |
| 1159 | 2005 – 2014 | 61.5 ± 12.1 | 32.4% | in-hospital 16% | |
| 2137 | 2006 – 2010 | 60.5± 13.6 | 38.3% | 30-day 16.9% | |
| 14911 | 2006 – 2014 | 64 ± 9 | 35% | in-hospital 19.5% | |
| 1157 | 2006 – 2015 | 66 [57–74] | 35.4% | in-hospital 18% | 26% / 52% |
| 1620 | 1996 – 2016 | 63.5 ± 12.9 | 32.5% | 30-day 22% | |
| 1317 | 2018 – 2021 | 63.1 ± 11.8 | 41% | in-hospital 20.4% → 13.9% | |
| 30-day 17.2% | ||||||
| 501 | 2011 – 2022 | 60 ± 11 | 35% | in-hospital 29% | |
| 4203 | 2009 – 2018 | 64 [52–73] | 33.3% | in-hospital 17.8% | |
| 7805 | 2017 – 2018 | 60.0 ± 13.6 | 34% | in-hospital 15.3% | |
| 2982 | 2011 – 2012 | 59.7 ± 14.0 | 34.4% | operative 17.4% | |
| 11843 | 2008 – 2015 | 69 [60–77] | 51.8% | operative9.5% | |
| 30-day 7.6% | ||||||
| 1217 | 2011 – 2016 | 67.9 ± 13.1 | 52.1% | in-hospital 10.8% | 24.8% / 16.6% |
| 10131 | 2012 – 2015 | 69.8 ± 13.5 | 53.1% | in-hospital 11.8% | 33% / 49.7% |
| 1058 | 2018 – 2021 | 51.6 ± 11.7 | 23.8% | in-hospital 7.6% | |
| 1582 | 2012 – 2016 | 48.9 ± 11.1 | 21.7% | in-hospital 5.5% | 7.8% / not mentioned |
| 2604 | 2001 – 2021 | 65 [54–74] | 33% | 30-day 18% |
(1995–1999 → 2010–2013)
ATAAD – acute type A aortic dissection, ERTAAD – European Registry of Type A Aortic Dissection, GERAADA – German Registry for Acute Aortic Dissection Type A, IRAD – International Registry of Acute Aortic Dissection, JROAD-DPC – Japanese Registry of All Cardiac and Vascular Diseases–Diagnostic Procedure Combination, JRAD – Japan Registry of Acute Aortic Dissection, NORCAAD – Nordic Consortium for Acute Type A Aortic Dissection, RENADA-RO – Romanian National Registry of Aortic Dissections, SCTS – Society of Cardiac and Thoracic Surgeons, Sino-RAD – Chinese Registry of Aortic Dissection, STS – Society of Thoracic Surgeons
Preoperative Risk Factors Reported Across Registries
| Study | Malperfusion | Cardiogenic shock | Reduced LVEF | PCS | Surgical Mortality |
|---|---|---|---|---|---|
| 30% | 15% | Not reported | 14.2% | in-hospital 21% |
| 33.6% | 57.8% | Not reported | Not reported | 30-day 16.9% |
|
| 43.6% | Not reported | 3.6% | in-hospital 18.2% |
| 33.9% | 21.4% | Not reported | Not reported | in-hospital 16% |
| Not reported | 30% | Not reported | 5.2% | in-hospital 17% |
| 36.5% | 14.5% | 20.4% | 6% | in-hospital 17.8% |
| Not reported | 15.8% | Not reported | Not included | operative 17.4% |
| Not reported | 15.5% | 28.1% | 1.2% | operative 9.5% |
| Not reported | 19.5% | Not reported | 16.3% | in-hospital 10.8% |
| 13.9% | 3.9% | Not reported | 4.2% | in-hospital 7.6% |
ATAAD – acute type A aortic dissection, ERTAAD – European Registry of Type A Aortic Dissection, GERAADA – German Registry for Acute Aortic Dissection Type A, IRAD – International Registry of Acute Aortic Dissection, JRAD – Japan Registry of Acute Aortic Dissection, NORCAAD – Nordic Consortium for Acute Type A Aortic Dissection, Sino-RAD – Chinese Registry of Aortic Dissection, STS – Society of Thoracic Surgeons
Among the reviewed datasets, GERAADA [7] is the only registry conducted with a fully prospective design, encompassing both data collection and analysis. Most others – such as IRAD [4,6], the European Registry of ATAAD (ERTAAD) [14,15] and NORCAAD [1,8,9] – are structured as retrospective analyses of prospectively collected data, typically gathered through detailed, physician-entered case report forms that include clinical, imaging and surgical variables.
Large national surgical registries like the Society for Thoracic Surgeons National Adult Cardiac Surgery Database (STS ACSD) [16], the Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) [13] and the Japan Cardiovascular Surgery Database (JCVSD) [17], apply these standardized forms across nearly all cardiac surgery centres in their respective countries.
In contrast, registries such as the National Inpatient Sample (NIS) [18], the Danish National Registry (linking four national databases via the unique Central Personal Registration number – Civil Registration, Patient, Prescription, and Cause of Death registries) [11,19], the Japanese Registry of All Cardiac and Vascular Diseases-Diagnostic Procedure Combination (JROAD-DPC) [20] and the German DRG database [21] rely entirely on administrative data derived from ICD-coded discharge records and other billing-related classification systems.
Most registries restrict inclusion to surgically treated ATAAD cases, though some, such as IRAD and the Japan Registry of Aortic Dissection (JRAD), also include patients managed medically [4,6,22].
Figures 2–4 summarize reported mortality outcomes across registries, stratified by inhospital, 30-day and operative mortality. The number of registries and cumulative patient populations contributing to each endpoint varied. In-hospital mortality was reported by 13 registries, encompassing a total of 50,470 patients. Thirty-day mortality was reported by 5 registries, representing 19,521 patients, while operative mortality was reported by 2 registries, including 14,825 patients.
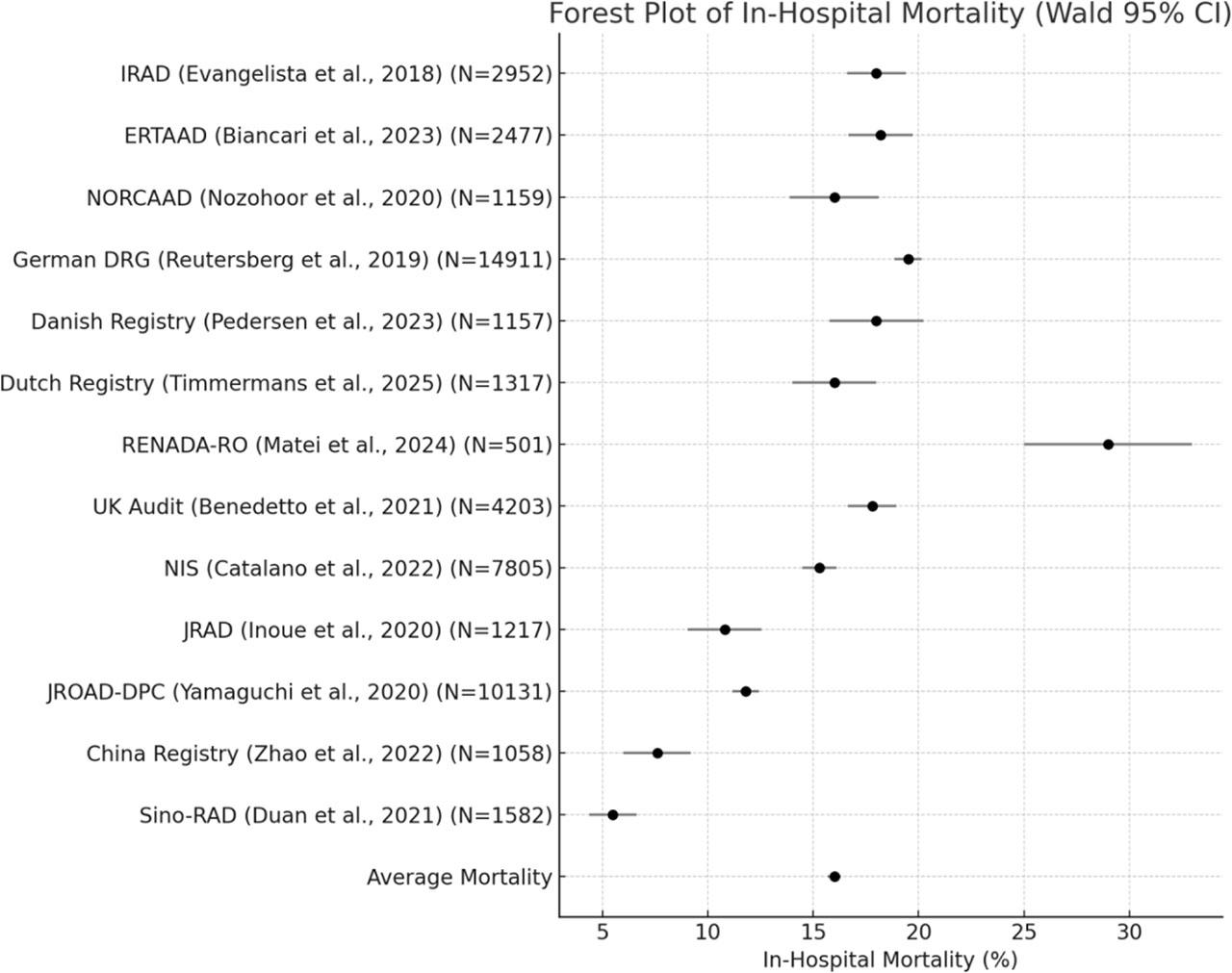
Forest Plot of In-Hospital Mortality in Acute Type A Aortic Dissection: A Synthesis of Multicenter Registry Data.
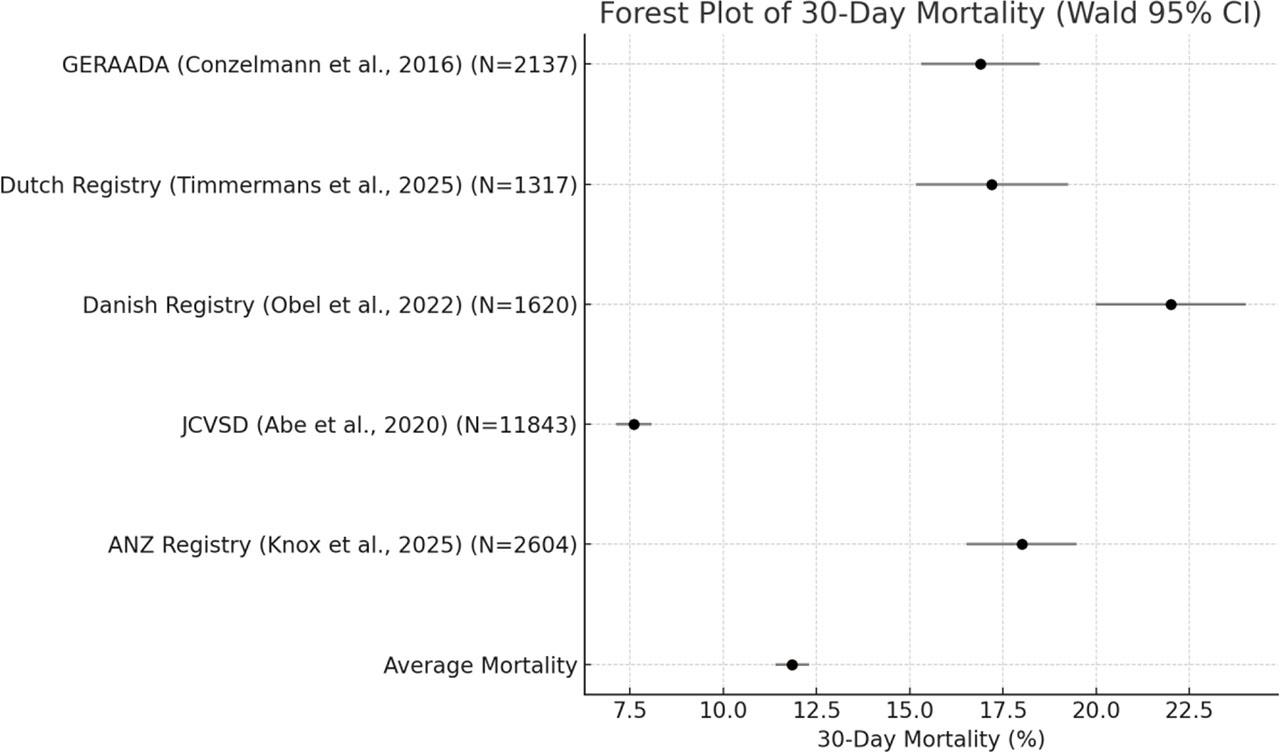
Forest Plot of 30-Day Mortality in Acute Type A Aortic Dissection: A Synthesis of Multicenter Registry Data.
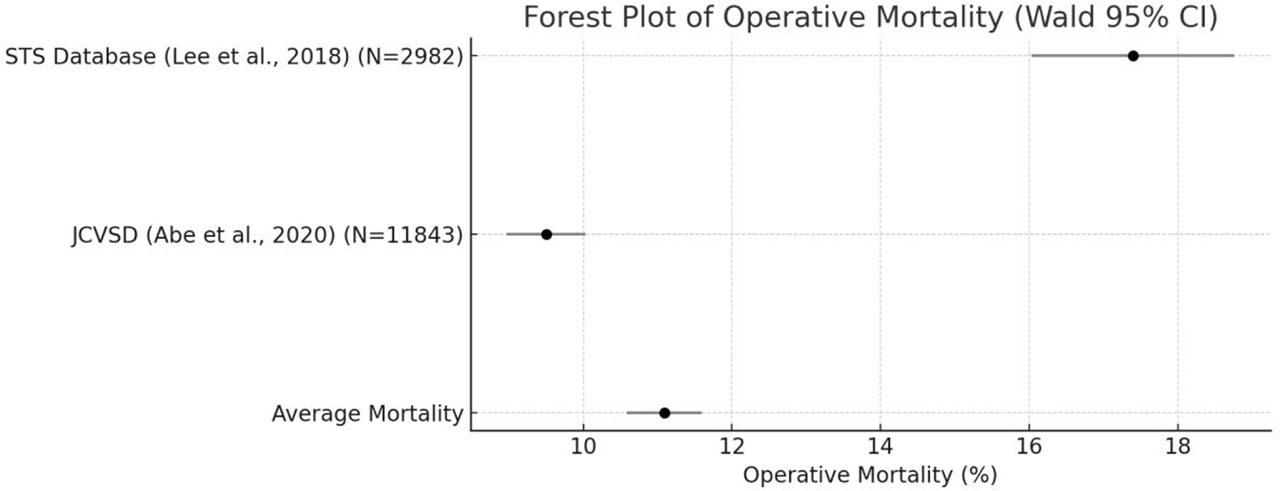
Forest Plot of Operative Mortality in Acute Type A Aortic Dissection: A Synthesis of Multicenter Registry Data.
A subset of the registries includes longitudinal data, allowing assessment of changes in early mortality over successive study periods. IRAD, one of the most comprehensive global registries, reported a significant decrease in in-hospital mortality over time, from 31% in the late 1990s to 22% in the early 2010s [6]. This improvement was accompanied by a reduction in surgical mortality from 25% to 18%, while the mortality among medically managed patients remained unchanged at 57% [6]. The UK Aortic Group also reported a decline in inhospital mortality from 22% in 2009 to 16% in 2018 [12]. A similar improvement was noted in Australia and New Zealand, where data from the ANZSCTS registry demonstrated a steady decline in 30-day mortality over the past two decades, from nearly 30% at the beginning of the study period to 15% in recent years [13]. Similarly, the Dutch nationwide registry reported a steep decline in in-hospital mortality, from 20% in 2018 to 14% in 2021, a trend that persisted after adjustment for age and sex [10]. In contrast, the Danish National Registry found no statistically significant change in 30-day mortality over a 20-year observation period [11]. In the Nationwide German Diagnosis-Related Group Statistics, in-hospital mortality remained relatively stable over time, with a slight increase from 24% in 1996–2000 to 25% in 2006–2010 [21]. The study reported that the slight rise coincided with a higher Elixhauser Comorbidity Score in later years. Nonsurvivors were generally older and had a higher prevalence of cardiovascular and renal comorbidities [21]. A comparable pattern was seen in Japan's JCVSD. Although risk-adjusted operative mortality was stable, annual surgical volume rose by 45% and the proportion of octogenarians increased to nearly one in five [17]. The prevalence of comorbidities such as renal dysfunction also increased [17].
Surgical mortality in ATAAD is a key indicator of healthcare system performance, institutional experience and effectiveness of perioperative management pathways [1,6]. Registries that employ detailed, standardised case-report forms – such as the STS ACSD [16], ANZSCTS [13] and JCVSD [17] – enable consistent perioperative data collection at scale. Conversely, databases built entirely on administrative codes provide broad national coverage and facilitate longitudinal tracking, particularly in unified healthcare systems, yet they generally lack the clinical specificity of dedicated registries. Some datasets originate from tertiary cardiovascular centres, introducing selection bias through referral pathways and transfer times [6,23]; others, especially national administrative registries, capture a broader and more representative patient population [16,20].
Discrepancies in outcome definitions and reporting further limit direct comparability between datasets. Among studies that report in-hospital mortality, rates range from 5–8% in Chinese registries [23,24] to 29% in the Romanian RENADA-RO registry [25]. Most large European datasets (NORCAAD, ERTAAD and the UK National Adult Cardiac Surgical Audit) cluster between 16% and 18% [9,12,14], whereas Japan's JRAD and JROAD-DPC registries report figures just above 10%, reflecting more favourable outcomes in East-Asian cohorts [20,22]. In studies using 30-day mortality as the endpoint, reported rates in Western European populations generally clustered between 17 and 22% [7,10,11]. GERAADA and the Dutch nationwide registry reported similar figures [7,10], while the Danish National Registry recorded a somewhat higher rate, suggesting modest variability across systems with broadly comparable healthcare structures [11].
Operative mortality reported by registries such as STS ACSD and the JCVSD is lower – reaching 9.5% in some cohorts [16,17] – but these figures may underestimate total peri-operative risk because patients who die before or shortly after surgery are often excluded. Finally, the 48-hour mortality rate reported by IRAD (4.4%) stands apart as a distinct early endpoint, capturing only the most immediate postoperative risk [4]. Although not directly comparable to in-hospital or 30-day mortality, it underscores the critical importance of timely surgical intervention in ATAAD.
Evaluating changes in surgical mortality over time offers critical insight into the evolving landscape of ATAAD management. While several registries demonstrate clear improvements, the magnitude and consistency of these gains vary across regions and healthcare systems. These favourable trends coincide with global advances in diagnosis, referral logistics and operative technique, yet they also underscore the persistently limited survival of patients deemed inoperable [26].
IRAD, the UK Aortic Group, ANZSCTS and the Dutch nationwide registry all document substantial reductions in early mortality [6,10,12,13]. However, investigators from the Dutch nationwide registry caution that the sharp four-year decline in mortality may partly reflect selection bias and other confounders, including pandemic-related changes in the types of patients treated and evolving surgical thresholds [10]. In the United Kingdom, this improvement was attributed to surgeon-specific volume–outcome effects, enhanced referral pathways, dedicated aortic services and more standardised peri-operative care [12]. The ANZSCTS series displays a parallel decline, consistent with trends observed in other high-volume surgical networks [13]. By contrast, Danish data show no significant change over twenty years, indicating that progress has not been universal [11]. A similarly muted pattern is seen in the German DRG dataset, where in-hospital mortality remained essentially static; although mean patient age did not rise, the inclusion of patients who would previously have been considered inoperable may explain the modest increase observed [21]. The Japanese data indicate that, in the context of steadily rising operative risk, maintaining a stable mortality rate can itself be considered a favourable outcome [17,20,22].
Overall, mortality appears to be declining in many centres, supported by rising surgical experience, even as more elderly and high-risk patients are being treated – underscoring progress despite increasing clinical complexity [27,28].
Early mortality following ATAAD varies considerably across regions, reflecting differences in healthcare infrastructure, access to specialized care and prehospital logistics.
East Asian registries consistently report the most favourable surgical outcomes [23,24]. In China, low operative mortality must be interpreted in the context of younger surgical populations and long-distance transfers to high-volume urban centres [24]. Authors note a likely survivor bias, as unstable patients may not reach surgery, suggesting that low mortality figures reflect selective inclusion rather than nationwide performance [23,24]. Japanese registries similarly demonstrate better outcomes, supported by centralized care and high surgical volume, despite a rising proportion of elderly and comorbid patients [17,20,22]. Notably, JRAD reported a 17% mortality among medically managed patients, significantly lower than the 58% observed in IRAD, largely because almost half of the non-surgical cohort in JRAD had stable thrombosed false lumen rather than being inoperable [6,22]. This underscores how differences in case definitions and treatment thresholds can influence outcome comparisons.
Western European registries report relatively uniform surgical outcomes, supported by widespread access to emergency intervention and structured referral systems. Nonetheless, within-region disparities remain: outcomes from Romania indicate a substantially higher mortality burden, likely due to delayed transfers and the accumulation of high-risk cases in tertiary centres, often presenting with advanced dissection and malperfusion [6,8,10,11,12,14,25].
In the United States, mortality rates are broadly comparable to European figures, though slight variation exists depending on the data source (Table 2) [16,18].
Age and sex are key demographic variables frequently examined in relation to ATAAD outcomes [29]. Across registries, substantial regional variation exists in the profile of surgically treated patients (Table 2).
Advanced age significantly increases in-hospital mortality in ATAAD – by up to sevenfold – due to frailty and comorbidities [27,30,31]. Nevertheless, surgery remains the preferred approach, as medical management is associated with extremely poor outcomes [32].
East Asian registries show the widest age divergence. In China, the mean age of surgical patients was around 50 [23,24], reflecting a younger cohort, whereas Japanese registries reported mean ages closer to 70, with approximately 1 in 5 patients aged 80 or above [17,20,22].
In Europe and the United States, mean patient age is generally between 60 and 65 years, with consistent figures across GERAADA, ERTAAD, the Danish and UK registries, and the STS ACSD and NIS datasets[ 7,11,12,14].
Sex distribution also varies considerably. Japan reported the highest proportion of women undergoing surgery, with female patients comprising over half of all cases in its three national registries [17,20,22]. In contrast, female representation in China was notably lower, with just over one in five patients in both major registries, possibly reflecting disparities in access to care or symptom recognition [23,24].
In Europe and North America, women remain underrepresented among surgically treated ATAAD patients, typically accounting for one-third or less of cases [6,7,8,15]. This reflects the known male predominance of the disease but may also be influenced by sex-specific differences in clinical presentation, comorbidities, and patterns of care [18,33,34,35]. Female patients often present at an older age, with a higher prevalence of comorbid conditions such as hypertension and chronic lung disease, and tend to exhibit more atypical symptoms [36,37,38,39]. These factors are thought to contribute to delayed diagnosis and surgical referral, and have been associated with worse outcomes in some studies [29,36,39].
Marked differences in the prevalence of critical preoperative complications in ATAAD are evident across registries and appear to correlate with reported mortality outcomes (Table 3).
In European registries, up to 1 in 2 patients presented with malperfusion or cardiogenic shock – two of the strongest predictors of early death [7,14,15,40,41,42,43,44]. For example, in GERAADA, over half of the patients were in cardiogenic shock and about one third had signs of end-organ malperfusion [7]. Similarly, ERTAAD and NORCAAD showed a high frequency of hemodynamic instability and organ ischemia at admission [9,15]. These findings align with the comparatively higher mortality rates observed in these cohorts.
In contrast, East Asian datasets – particularly those from China and Japan – consistently reported lower rates of preoperative instability [17,22,24]. Fewer than 1 in 10 patients in the China Registry arrived in shock or with evidence of malperfusion [24]. While some of these differences may reflect earlier referral or selection bias favouring stable surgical candidates, they likely contribute to the markedly lower operative mortality seen in these populations.
Prior cardiac surgery was most common in IRAD and JRAD, affecting up to 1 in 6 patients – an important consideration given the added technical complexity and risk [6,22,45].
Taken together, these observations suggest that regional differences in early mortality following ATAAD surgery are not solely attributable to surgical approach or hospital capacity, but also reflect the baseline severity of illness at presentation. Standardized definitions and consistent reporting of these risk factors are essential for meaningful international comparison and quality improvement.
Contemporary data from international registries reveal both progress and ongoing challenges in the management of acute type A aortic dissection. While early mortality is declining in many regions, substantial variation remains, partly reflecting differences in patient characteristics and access to specialized care. Interpretation is further limited by heterogeneity in registry design, data quality and outcome definitions. Additionally, most available data come from high-income countries, underscoring the need to expand registry efforts in underrepresented regions. Standardized reporting, long-term follow-up, and integration of real-world data are essential to improve risk stratification, guide clinical decision-making and support evidence-based optimization of care delivery on a global scale.