Atherosclerotic cardiovascular disease is a leading cause of morbidity and mortality in patients with diabetes. Given the increased cardiovascular risk associated with diabetes, early and accurate identification of ASCVD is critical for improving patient outcomes. Diabetes mellitus, particularly type 2 diabetes, is a growing global health concern, affecting approximately 537 million adults worldwide in 2021, with projections suggesting an increase to 783 million by 2045. The rise in prevalence is most significant in economically disadvantaged regions, where undiagnosed diabetes accounts for 24–54% of cases. Diabetes is broadly classified into type 1 diabetes (an autoimmune disorder), type 2 diabetes (the most common form associated with obesity and sedentary lifestyle), gestational diabetes, and other less common types such as monogenic diabetes and diabetes secondary to medications like glucocorticoids. Among these, T2DM is the primary contributor to cardiovascular complications, particularly ASCVD [1].
Prediabetes and diabetes significantly increase the risk of atherosclerotic complications, including coronary artery disease and stroke, both of which contribute to higher mortality rates. Atherosclerosis is a multi-factorial process involving genetic predisposition and environmental risk factors such as aging, male gender, family history, dyslipidemia, hypertension, obesity, physical inactivity, smoking, and elevated uric acid levels. These factors lead to chronic vascular inflammation and arterial wall damage, which accelerate the development of atherosclerosis [2].
Although advances have been made in the molecular understanding of atherosclerosis, as well as in treatments like statins for lowering lipid levels, significant gaps remain in fully addressing ASCVD risk. The role of immune cells in atherosclerotic plaques is critical in influencing plaque stability, and despite optimal management of traditional risk factors, a residual cardiovascular risk remains. The increasing prevalence of metabolic syndrome (MetS), which includes abdominal obesity, insulin resistance, hypertension, and dyslipidemia, further heightens the risk of ASCVD. This syndrome, often referred to as syndrome X, markedly raises the likelihood of developing both ASCVD and diabetes [3].
Insulin resistance, central to T2DM and MetS, exacerbates cardiovascular risk by promoting lipid imbalances and chronic inflammation. These metabolic disturbances accelerate atherosclerosis progression, complicating the search for effective anti-inflammatory treatments. Genomic studies, such as genome-wide association studies (GWAS), have identified hundreds of genetic loci related to ASCVD, enhancing our understanding of the disease's genetic drivers and paving the way for more targeted screening and risk assessment tools [3].
This article focuses on the importance of enhanced screening for ASCVD in diabetic individuals, highlighting the use of advanced risk scoring models and modern detection techniques. By optimizing screening protocols, clinicians can better stratify risk, initiate preventive interventions, and tailor treatment strategies to mitigate cardiovascular complications in this high-risk population.
Diabetes mellitus and atherosclerosis share common pathological pathways that significantly increase the risk and hasten the development of atherosclerosis in individuals with diabetes, as evidenced by early atherosclerotic changes observed in children and adolescents with type 1 diabetes. These include dyslipidemia with high atherogenic low-density lipoprotein (LDL) levels, hyperglycemia, endothelial dysfunction, and increased inflammation (Figure 1) [3].
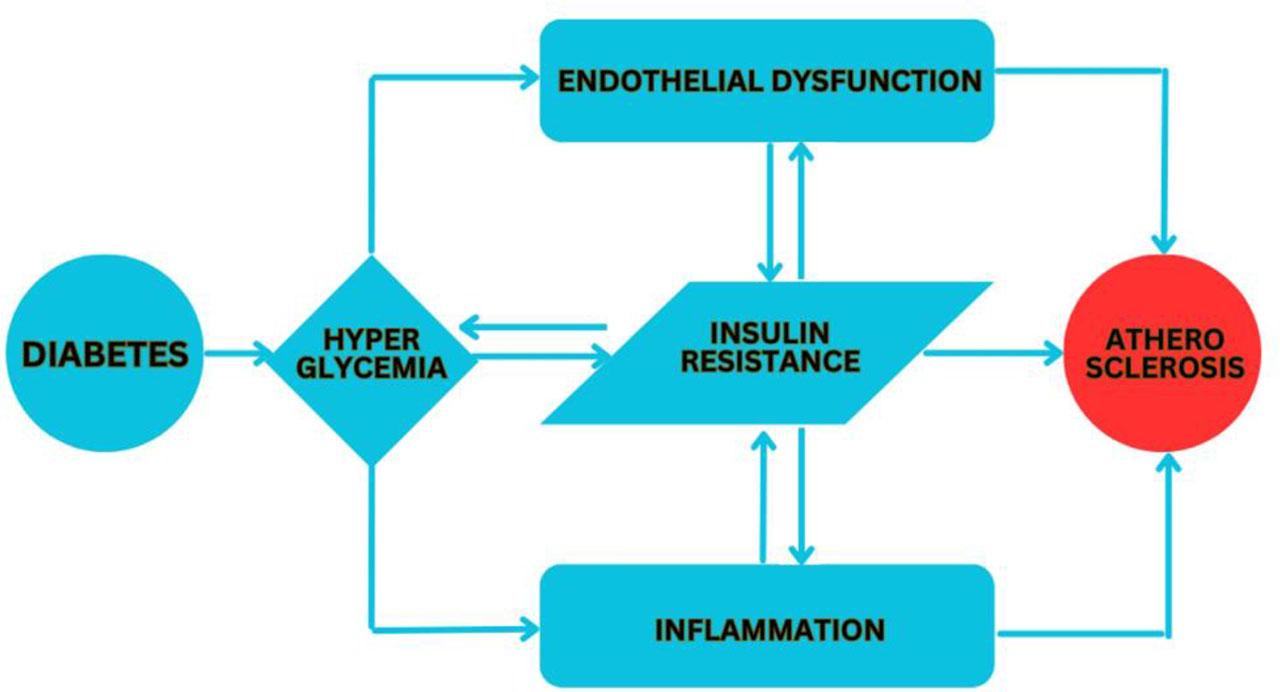
Relationship between diabetes and atherosclerosis.
The process of atherosclerosis begins with endothelial dysfunction, often triggered by mechanical stress at arterial bends or bifurcations, leading to endothelial activation and the recruitment of immune cells. These cells, particularly monocytes, adhere to and penetrate the arterial wall, differentiating into macrophages that consume lipids and transform into foam cells, initiating plaque formation. Early atherosclerotic lesions, or “fatty streaks,” feature these foam cells along with vascular smooth muscle cells (VSMCs) and T lymphocytes, which contribute to the progression of the lesion through ongoing endothelial injury and inflammation. As plaques mature, they may either stabilize or become destabilized through the action of matrix metalloproteinases (MMPs) released by macrophages, leading to potential plaque rupture and thrombosis, which can result in severe ischemic events and metabolic disturbances in the affected tissues [4].
Atherosclerosis in diabetes is driven by key mechanisms such as insulin resistance, hyperglycemia, dyslipidemia, inflammation, and oxidative stress. Insulin resistance, a core feature of type 2 diabetes, impairs glucose metabolism and promotes endothelial dysfunction, a critical factor in atherosclerosis development. Hyperglycemia exacerbates vascular damage through oxidative stress and the formation of advanced glycation end-products (AGEs), which increase inflammation and endothelial injury. Diabetes associated dyslipidemia, with elevated triglycerides and small dense LDL (sdLDL) particles, further accelerates atherosclerosis. Chronic low-grade inflammation and oxidative stress contribute to plaque formation and instability, increasing the risk of cardiovascular events [5].
This section examines these mechanisms and their role in the progression of atherosclerosis in diabetic patients, highlighting the need for targeted therapies to reduce cardiovascular risk.
Insulin resistance, a defining feature of type 2 diabetes mellitus, impairs insulin's ability to facilitate glucose uptake in tissues such as skeletal muscle, adipose tissue, and the heart, and to inhibit hepatic glucose output. This condition often develops long before hyperglycemia and diabetes become evident, with obesity significantly contributing to its prevalence and related vascular complications [6].
Insulin signaling is mediated through two major pathways: the phosphatidylinosi-tol-3-kinase (PI3K)-dependent pathway, which is crucial for metabolic and hemodynamic responses, and the mitogen-activated protein kinase (MAPK)-dependent pathway, which regulates gene expression, differentiation, and cell growth. In insulin resistance, the PI3K pathway is impaired, leading to reduced nitric oxide (NO) production and consequent endothelial dysfunction. Concurrently, the MAPK pathway is upregulated, resulting in increased endothelin-1 (ET-1) production [7].
This dysregulation also promotes the expression of vascular risk factors such as plasminogen activator inhibitor-1 (PAI-1) and adhesion molecules, stimulates vascular smooth muscle cell proliferation, and triggers excessive release of free fatty acids (FFAs), further exacerbating oxidative stress and vascular inflammation. Elevated serum levels of inflammatory markers like tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and CRP in insulin-resistant individuals underline the association with chronic low-grade inflammation and endothelial dysfunction, enhancing the risk for atherosclerotic cardiovascular disease [8].
Recent research has increasingly focused on the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) as a valuable tool for evaluating insulin resistance in patients with type 2 diabetes mellitus. HOMA-IR has also proven effective in assessing insulin resistance in non-diabetic individuals experiencing chest pain but showing no signs of myocardial perfusion defects, revealing its association with endothelial dysfunction and its potential to provide independent prognostic insights [9]. Additionally, studies have identified that insulin resistance adipocyte-derived exosomes (IRADEs) can increase plaque vulnerability and overall plaque burden in diabetic ApoE−/− mice, primarily via the sonic hedgehog (shh) pathway which mediates angiogenesis of the vasa vasorum. Targeting this pathway through gene silencing of shh has been proposed as an innovative therapeutic approach for managing diabetic atherosclerosis [10].
It is well known that diabetes mellitus, with a hypercoagulable state, accelerates atherosclerosis with impaired plaque stability and that, in fact, atherosclerosis represents the major cause of mortality among these patients with a reduced endothelial thrombomodulin (TM) expression. Also, diabetes-associated ASCVD, compared to the simple form of ASCVD, is characterized by a larger necrotic core area with a thin-cap atheroma and a significantly pronounced inflammatory cell infiltrate. Because hyperglycemia exacerbates atherosclerosis progression and at the same time hinders plaque regression, despite intensive lipid lowering, the probability of atherosclerosis and thus of myocardial infarction remains increased in these diabetic patients, suggesting that diabetes-specific mechanisms truly contribute to atherosclerosis, independent of elevated blood lipids. It was also observed that optimal glycemic control provided beneficial effects in preventing microvascular complications of diabetes, such as kidney disease and retinopathy, but had only minor effects in preventing major cardiovascular events, especially in patients with established ASCVD [11].
Endothelial dysfunction, a precursor to both macrovascular and microvascular complications, is associated with prolonged and acute episodes of hyperglycemia in both animal models and human studies. Intensive glycemic control has demonstrated significant efficacy in preventing microvascular complications more so than macrovascular diseases. Hyperglycemia contributes to vascular damage primarily through the disruption of NO bioavailability and the increased accumulation of reactive oxygen species (ROS), leading to endothelial dysfunction [12].
Hyperglycemia further harms the vascular system through several cellular processes: it increases the production of intracellular AGEs, enhances the expression of AGE receptors (RAGE) and their ligands, stimulates the polyol and hexosamine pathways, activates protein kinase C (PKC), and upregulates the hexosamine pathway. Oxidative stress, driven by these processes, is a central pathway in the progression of insulin resistance and T2DM [13].
The oxidative stress induced by hyperglycemia leads to DNA damage and increased ADP-ribose polymer production, activating nuclear polymerase (PARP) and inhibiting glyceraldehyde-3-phosphate dehydrogenase activity. This sequence increases levels of glycolytic intermediates, exacerbating damaging cellular mechanisms, enhancing vascular permeability, oxidative stress, and apoptosis. Hyperglycemia also triggers the activation of nuclear factor-κB (NF-κB), promoting vascular inflammation through increased production of adhesion molecules, cytokines, and chemoattractants, which further recruit inflammatory cells to the vascular wall. Additionally, hyperglycemia enhances the expression of coagulant tissue factors such as PAI-1, contributing to a prothrombotic state. Alongside, dyslipidemia and hyperinsulinemia also disrupt vascular tone by altering the balance of vascular tone regulators, further compounding vascular dysfunction [14].
Diabetes-associated dyslipidemia is characterized by decreased levels of high-density lipoprotein (HDL) cholesterol, increased triglycerides, and minor effects on LDL cholesterol, largely due to excessive hepatic production of very low-density lipoproteins (VLDL). This imbalance elevates serum triglyceride levels, significantly increasing the risk of ASCVD such as coronary heart disease (CHD) in individuals with diabetes. Dyslipidemia is a key modifiable risk factor not only for diabetes but also for atherosclerosis, stroke, and broader cardiovascular diseases. Effective management of dyslipidemia in diabetes typically starts with lifestyle interventions, including weight loss, dietary changes, and regular aerobic exercise, which are crucial for improving lipid profiles and reducing overall cardiovascular risks [5].
The relationship between diabetes and atherosclerosis includes a critical focus on sdLDL particles, known for their increased atherogenic potential. While native LDL particles do not typically cause significant lipid accumulation in cultured cells, modifications to LDL transform its physical-chemical properties, enhancing its ability to accumulate lipids. These modifications include desialylation, increased density, reduced size, and an acquired negative charge, ultimately yielding altered LDL particles with enhanced atherogenic characteristics. Notably, these altered particles, especially the sdLDL subfraction, are more prone to oxidation due to decreased antioxidant levels and changed lipid composition, which usually represents the final stages of LDL modification [15].
Once these modified LDL particles penetrate the subendothelial space at atherosclerotic sites, they are likely to remain longer due to binding with proteoglycans, which increases their chance of being internalized by cells within the lesion. Unlike normal LDL, which is typically cleared via LDL receptors, modified LDL is primarily internalized through nonspecific phagocytic pathways, leading to excessive intracellular cholesterol accumulation and subsequent foam cell formation, a hallmark of atherosclerosis [16].
Research using a murine model of diabetes has demonstrated that LDL particles from type 1 diabetic (T1D) patients have a significantly longer retention time in the subendothelial spaces of atherosclerosis-prone arterial walls compared to those from non-diabetic controls, suggesting a higher atherogenic potential in diabetic conditions. Furthermore, cross-sectional studies indicate that while elevated levels of apolipoprotein B and sdLDL are not common in young individuals with T1D, they are more prevalent in those with type 2 diabetes. This disparity underscores the importance of evaluating specific LDL subfractions in diabetic patients, as total LDL cholesterol levels may not fully reflect the atherosclerotic risk, particularly when sdLDL levels are elevated [17].
Chronic inflammation is a key factor in the pathogenesis of both atherosclerosis and diabetes. In patients with T2DM, there is an upregulation in inflammasome activity, increased levels of the nucleotide-binding oligomerization domain-like receptor 3 (NLRP3), and elevated concentrations of pro-inflammatory cytokines such as interleukin (IL)-1β and IL-18. Additionally, Neutrophil Extracellular Trap (NET) activation, or NET-osis, is intensified in T2DM patients, particularly under hyperglycemic conditions, and is linked to the development of atherosclerosis. Research into anti-inflammatory treatments aimed at reducing cardiovascular risks in diabetic patients has identified promising therapies such as salicylates and canakinumab, a monoclonal antibody targeting IL-1β. These treatments have been effective in lowering inflammation markers in diabetic patients without significantly affecting LDL-cholesterol levels [18].
Oxidative stress, marked by an increase in ROS production and reduced antioxidant capacity, is also prevalent in diabetes. Experimental studies have demonstrated the role of the NADPH oxidase protein in the progression of diabetes-related atherosclerosis. Conversely, a deficiency in the antioxidant enzyme regulator glutathione peroxidase 1 has been shown to aggravate atherosclerosis in diabetic models. While antioxidant therapies could be beneficial in managing diabetes-associated atherosclerosis, more targeted and selective approaches are needed to realize substantial benefits from these antioxidant treatments. It is crucial to recognize that xanthine oxidase, the enzyme responsible for the production of uric acid as a by-product of purine metabolism, generates increased amounts of reactive oxygen species under pathological conditions. Consequently, elevated plasma uric acid levels are linked to a heightened risk of developing atherosclerotic cardiovascular disease. Equally important, the complement system plays a key role in inflammation, contributing to the onset and progression of both diabetes and atherosclerosis [19]. Recent studies have high-lighted the role of cluster of differentiation (CD) 93, also known as complement protein 1 subcomponent receptor (C1qR1 or C1qRp), in influencing the development and progression of atherosclerosis, positioning it as a potential therapeutic target [20].
Endothelial dysfunction has an important role in the pathogenesis of atherosclerosis, significantly impacting vascular smooth muscle cell proliferation. The endothelium, a monolayer of cells lining the inner surface of blood vessels, is integral to maintaining vascular homeostasis. These cells regulate a range of critical vascular functions including cell adhesion, tissue growth, metabolism, angiogenesis, and inflammatory responses. They also maintain vascular integrity, hemostasis, and permeability. Dysfunction of the endothelium disrupts the balance of vasodilators and vasoconstrictors, such as NO, prostacyclin (PGI2), and ET-1, alongside ROS. This dysfunction can trigger abnormal VSMC growth and alter the regulatory mechanisms of platelet activation, fibrinolysis, and thrombogenesis, ultimately impacting vascular health and blood clotting dynamics (Figure 2). Vascular smooth muscle cells play a crucial role in atherosclerosis. Typically, VSMCs help maintain vascular tone, structure, and integrity. However, following endothelial injury or during inflammation, VSMCs can switch from a contractile to a proliferative phenotype. In this proliferative state, VSMCs migrate to the intima, the inner layer of the blood vessel, where they contribute to the development of atherosclerotic plaques by producing extracellular matrix proteins and facilitating lesion growth [21].
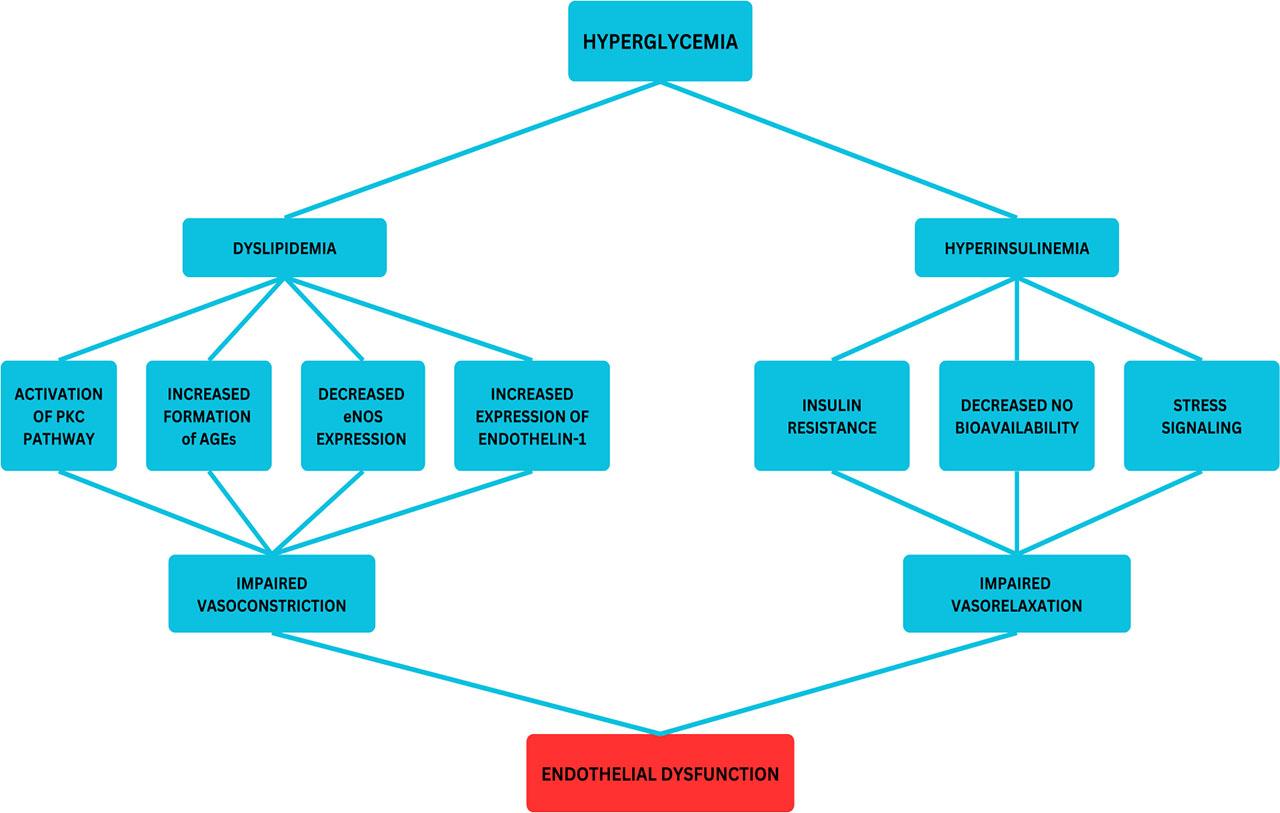
Pathways leading to endothelial dysfunction in diabetes mellitus.
Endothelial dysfunction has an important role in atherosclerosis by promoting the recruitment and retention of inflammatory cells within the vessel wall and influencing vascular smooth muscle cell behavior. Dysfunctional endothelial cells release factors that drive VSMC proliferation and migration, which in turn contribute to the development of neointima and plaque progression. Additionally, VSMCs can secrete factors that exacerbate endothelial dysfunction, creating a cyclical feedback loop that accelerates the progression of atherosclerosis [22].
AGEs further exacerbate vascular damage under hyperglycemic conditions by altering the structural and functional properties of vascular components. AGEs interact with their receptor, which enhances superoxide production and vascular inflammation. AGEs also reduce endothelial nitric oxide synthase (eNOS) activity and NO synthesis while increasing ET-1 expression, contributing to further endothelial dysfunction [23].
Good glycemic control is associated with improved microvascular function in newly diagnosed T2DM patients with cardiovascular disease (CVD), but this benefit diminishes with prolonged disease duration. Additionally, hyperglycemia impairs endothelial cell proliferation and migration by inhibiting pathways like ERK, p38, and Akt, effects which can be partially mitigated by co-incubation with HDL, which also possesses anti-inflammatory properties. However, the anti-inflammatory capabilities of HDL are significantly compromised in T2DM patients due to chronic hyperglycemia and persistent inflammation, diminishing its protective role against atherosclerosis [8].
Furthermore, fluctuations in glucose levels have been linked to chromatin remodeling, potentially explaining persistent vascular dysfunction in poorly controlled diabetes. Research also highlights the role of microRNA miR-29 in maintaining endothelial function by enhancing NO production. Therapeutic delivery of miR-29 mimics has shown potential in restoring endothelial function, underscoring its promise as a treatment for cardiometabolic disorders [24].
The concept of “metabolic memory” or “legacy effect” describes the persistent risk of cardiovascular complications in diabetes, attributed to prolonged high blood glucose exposure. This phenomenon is partly due to the formation of AGEs during periods of elevated glucose, which accumulate in those with historical poor glucose control, potentially accelerating vascular disease progression in diabetic individuals. While the direct link between hyperglycemia and macrovascular complications such as atherosclerosis is less clear, it is hypothesized that high glucose levels may primarily affect organs like the liver and adipose tissue, indirectly influencing atherosclerotic cells through altered organ-specific signaling [25].
Elevated glucose can increase metabolic flux through pathways like the mitochondrial electron transport chain, resulting in excessive reactive oxygen species (ROS) production. Glucose metabolites also trigger pro-inflammatory pathways via PKC-beta and aldose reductase activation. Additionally, extracellular high glucose levels lead to protein glycation and glycoxidation, contributing to AGE accumulation. These AGEs play a critical role in atherosclerosis by promoting endothelial dysfunction, enhancing adhesion molecule expression, increasing monocyte/macrophage adherence, and stimulating cytokine release, thereby fostering a pro-inflammatory state within atherosclerotic plaques [26].
Furthermore, AGEs alter LDL particles, disrupt cholesterol transport, augment vasoconstriction through ET-1, and decrease vasodilation by reducing NO availability. They also modify extracellular matrix components, exacerbating atherosclerotic lesion formation. In atherosclerotic mouse models, the absence of RAGE reduces lesion development, suggesting it as a potential therapeutic target. Recent studies also indicate a direct role of AGEs in enhancing macrophage phagocytosis via scavenger receptor stimulation, highlighting their influence on inflammation and lesion progression. These insights underscore the complex interplay between glucose levels, AGE formation, and vascular damage, revealing potential therapeutic targets for managing diabetic complications [27].
Global CVD risk assessment analyzes key risk factors to predict the likelihood of developing cardiovascular diseases. The Framingham Heart Study, launched in 1948, was a groundbreaking initiative that systematically identified major risk factors for CVD, including high blood pressure, cholesterol levels, smoking, diabetes, and obesity. Based on decades of data from thousands of participants, researchers developed the Framingham Risk Score (FRS) — one of the first comprehensive models to estimate an individual's 10-year risk of developing coronary heart disease. While the Framingham model was widely adopted, it was primarily based on a predominantly white population from a single geographic area, which limited its applicability to diverse racial and ethnic groups. As a result, further refinements were needed to create more inclusive and precise risk assessment models. To address the limitations of the Framingham model, newer tools were developed [28].
One of the most widely used today is the Pooled Cohort Equations (PCE), introduced in 2013 by the American College of Cardiology (ACC) and American Heart Association (AHA). The PCE model provides a more comprehensive risk assessment for ASCVD by incorporating factors such as age, sex, cholesterol levels, blood pressure, smoking status, diabetes, and race. This model is particularly valuable in guiding clinicians in making treatment decisions: low risk (<5%): patients are advised to focus primarily on lifestyle modifications; borderline risk (5–7.5%): additional risk-enhancing factors (e.g., family history, inflammatory markers) are considered to refine risk assessment; intermediate risk (7.5–20%): further testing, such as imaging, may be recommended to guide decisions on pharmacologic interventions; high risk (>20%): patients require intensive management, including statin therapy and other preventive measures [29].
Despite its improvements, the PCE model still has limitations, especially in accurately assessing risk in younger adults and individuals with diabetes.
For individuals at borderline or intermediate risk, additional diagnostic tools can help refine risk prediction. One such tool is coronary artery calcium (CAC) scoring, which uses CT imaging to detect calcified plaques in coronary arteries. A high CAC score suggests significant subclinical atherosclerosis, indicating a higher likelihood of future cardiovascular events, even if traditional risk factors seem controlled. The use of CAC scoring is particularly beneficial for identifying asymptomatic individuals who might benefit from early intervention, reclassifying intermediate-risk patients to determine whether they need aggressive treatment and providing objective evidence of atherosclerosis, helping patients better understand their personal risk [30].
While traditional risk assessment models rely heavily on clinical parameters and lifestyle factors, emerging research suggests that integrating biomarkers and advanced imaging techniques can further improve risk prediction.
Polygenic Risk Scores (PRS): By analyzing multiple genetic variants associated with ASCVD, PRS may offer early risk assessment from birth, helping to identify high-risk individuals before clinical symptoms appear.
Advanced Imaging Modalities: Techniques such as coronary CT angiography (CCTA) and vascular MRI provide detailed insights into plaque characteristics and vessel health, allowing for more precise predictions of CVD events.
Inflammatory and Lipid Biomarkers: Markers such as C-reactive protein (CRP), lipoprotein(a) and apolipoprotein B (ApoB) offer additional layers of risk assessment, particularly for individuals who appear to have normal cholesterol levels but may still be at elevated risk The Framingham Heart Study was instrumental in developing the first risk models, which have since been adopted globally [31].
Risk prediction algorithms, such as the Framingham Risk Score, SCORE2 (Systematic Coronary Risk Estimation 2), and SMART2, depend on conventional risk factors but are limited in their ability to predict future cardiovascular events, as they do not fully capture the pathophysiological complexities of atherosclerosis and plaque instability. This limitation underscores the need for innovative approaches to identify and manage subclinical atherosclerosis in asymptomatic individuals. Biomarkers of inflammation, such as CRP, apo B, lipoprotein(a), and genetic markers, have been identified as additional risk factors for atherosclerotic cardiovascular disease. Recent advances have highlighted the potential of polygenic risk scores (PRS), which aggregate numerous genetic variants associated with ASCVD into a single measure. Unlike traditional risk factors, PRS are present from birth, enabling earlier risk assessment and potentially better predictions of ASCVD risk, especially in younger individuals. This early identification could facilitate personalized prevention strategies before atherosclerotic plaque formation begins. However, challenges remain in applying PRS across diverse genetic populations and determining optimal therapeutic strategies [29].
Polygenic Risk Scores (PRS) have emerged as a significant tool in the assessment of CVD risk, offering insights beyond traditional risk factors. Recent studies have explored the integration of PRS into clinical practice to enhance the prediction and prevention of CVD events. A study involving nearly 80,000 veterans investigated the predictive utility of PRS for coronary heart disease (CHD) and acute ischemic stroke. The findings demonstrated that higher PRS were significantly associated with an increased incidence of myocardial infarction, acute ischemic stroke, and cardiovascular death. Notably, the predictive value of PRS was more pronounced among women and younger individuals. However, while PRS provided additional information, the overall improvement in risk prediction over traditional factors was modest [30]. The American Heart Association (AHA) has addressed the role of PRS in CVD risk assessment. In their scientific statement, they reviewed contemporary science, clinical considerations, and future challenges associated with PRS. The AHA emphasized the potential of PRS to enhance risk stratification but also highlighted the need for further research to fully understand their clinical utility and integration into existing risk assessment frameworks [29].
Cardiovascular risk prediction remains a critical challenge in the management of type 2 diabetes mellitus, given the increased burden of atherosclerotic cardiovascular disease in this population. Numerous risk models have been developed to estimate cardiovascular event risk, yet their predictive accuracy and applicability to diabetic patients vary significantly. A recent analysis conducted by Dziopa et al. compared the performance of 22 commonly used cardiovascular risk models, including those designed specifically for individuals with diabetes and others originally intended for the general population but applied to diabetic cohorts. The study found notable variability in the predictive performance of these models. Of the 22 models assessed, 13 were developed for the general population, while nine were specifically tailored to individuals with T2DM. Surprisingly, the results indicated that general population-based models did not necessarily perform worse than diabetes specific models. The SCORE CVD rule, initially created for the general population, demonstrated the highest predictive performance for cardiovascular disease outcomes in diabetic patients. When evaluating discrimination, measured by the C statistic (where a value of 1.0 represents perfect prediction and 0.5 reflects a model performing no better than chance), the models varied between 0.62 and 0.67 for predicting cardiovascular disease and between 0.64 and 0.69 when expanded to include heart failure and atrial fibrillation. A particularly striking finding was the limited predictive advantage of models developed exclusively for diabetes patients. The UK Prospective Diabetes Study (UKPDS) risk engine, widely regarded as a gold standard for diabetes-related cardiovascular risk estimation, performed worse than the general SCORE CVD rule. This unexpected result highlights that diabetes-specific models do not necessarily outperform general models in predicting cardiovascular events in this high-risk group. The findings challenge the assumption that models incorporating diabetes-related variables such as glycated hemoglobin (HbA1c) and diabetes duration always enhance risk prediction [32].
Another key observation was that the complexity of a model, in terms of the number of variables included, did not necessarily translate into better predictive performance. For example, QRISK3, which integrates 19 different variables, achieved a C statistic of 0.68, while SCORE CVD, which incorporates only six variables, demonstrated a superior C statistic of 0.69. This suggests that a well-calibrated and validated model with fewer, but highly predictive variables, may perform just as effectively as a more intricate model with multiple risk factors. The study also examined whether recalibration could improve the predictive accuracy of these models. By adjusting for differences in population characteristics and baseline risk, recalibration significantly improved the performance of many models, bringing calibration slopes closer to 1.0, a value indicative of strong agreement between predicted and observed risk. This underscores the importance of local adaptations of widely used models, as risk estimation tools derived from one population may require fine-tuning before application to another [32].
Further analysis was conducted on the models' ability to predict specific cardiovascular events, such as coronary heart disease, stroke, and heart failure. The predictive accuracy varied depending on the event, with coronary heart disease being the best-predicted outcome, while models were less effective in forecasting stroke and heart failure. Certain models, such as RECODE, performed slightly better in predicting a broader range of cardiovascular conditions, including heart failure and atrial fibrillation. In contrast, the Framingham 1998 model showed strong performance in estimating both cardiovascular disease and cardiovascular-related complications [28].
These findings have important clinical implications. First, they emphasize the need for improved risk prediction models that are specifically optimized for patients with T2DM. While existing models provide a reasonable approximation of cardiovascular risk, there remains substantial room for refinement. Given that general population-based models such as SCORE CVD performed well in this study, clinicians should consider model selection carefully and avoid assuming that diabetes-specific tools are inherently superior. Furthermore, recalibration appears to be an effective method for improving accuracy, reinforcing the necessity of adjusting risk models based on local epidemiological data.
Looking ahead, the integration of novel biomarkers, imaging modalities, and genetic data may enhance the predictive accuracy of cardiovascular risk models. Emerging tools such as coronary artery calcium (CAC) scoring and polygenic risk scores offer promising avenues for refining risk stratification. Machine learning and artificial intelligence may also play a role in developing more personalized risk assessment tools by analyzing large datasets and identifying complex interactions between risk factors [30].
Traditional risk models, while useful, are constrained in their ability to predict future events and fail to capture the full spectrum of atherosclerotic progression. Emerging tools such as PRS and advanced imaging techniques, including coronary artery calcium (CAC) scoring and coronary computed tomography angiography (CCTA), offer promise in enhancing primary risk assessment and tailoring interventions. Coronary artery calcium, detectable via computed tomography (CT) scans, serves as a reliable marker of subclinical atherosclerosis. The Agatston score, introduced in 1990, quantifies CAC by assessing both the area and density of calcified plaques, providing a standardized measure of coronary atherosclerotic burden. Extensive research indicates that higher CAC scores are independently associated with an increased risk of atherosclerotic cardiovascular disease events, such as myocardial infarction and stroke. Importantly, incorporating CAC scoring into risk assessment models enhances the predictive accuracy beyond traditional risk factors alone. This improvement facilitates more precise stratification of individuals into appropriate risk categories, thereby informing targeted primary prevention strategies. Despite robust evidence supporting the utility of CAC scoring in Western populations, data from other regions, including Japan, remain limited. Notably, studies have reported lower prevalence and severity of CAC among Japanese individuals compared to Western counterparts, even after adjusting for conventional risk factors. This observation underscores the need for region-specific research to validate the applicability of CAC scoring across diverse populations [33]. CAC scoring, in particular, has proven to be a highly reliable marker for subclinical atherosclerosis and an accurate predictor of future coronary heart disease or ASCVD events. It surpasses traditional risk factors and other early markers in predicting ASCVD. CAC testing is especially useful in individuals with borderline or intermediate risk, as it provides a more precise estimation of their cardiovascular risk, guiding decisions about preventive interventions such as statin therapy The most widely used risk score for predicting future cardiovascular events is the ASCVD risk score (2013), developed by the American Heart Association (AHA). This score is based on diverse racial data and considers factors such as age, gender, ethnicity, cholesterol levels, blood pressure, diabetes and hypertension history, smoking, and the use of medications like aspirin and statins. Patients are categorized into high (>20%), intermediate (7.5–20%), borderline (5–7.5%), or low risk (<5%) groups. However, the score's validity has not been extensively tested in populations receiving ongoing medical care, and its predictive power in treated patients remains uncertain, highlighting the need for better risk identification [34].
Both intrinsic and extrinsic infections are notable complications frequently encountered in individuals with type 2 diabetes (T2D). The heightened vulnerability to community-acquired infections in these patients is closely linked to poor glycemic control and is widely recognized in the literature. Contributing factors, including persistent hyperglycemia and hyperlipidemia, increase the likelihood of infections such as urinary tract infections, respiratory illnesses, periodontal conditions, and soft tissue infections among diabetic populations. Research has consistently highlighted impairments in both innate and adaptive immune responses in those with T2D. The innate immune system, serving as the body’s frontline defense, plays a vital role in pathogen clearance, tissue repair, and maintaining homeostasis following various forms of injury. Neutrophils, as key players within this system, are essential for pathogen eradication. Experimental and clinical findings suggest that chronic hyperglycemia leads to disruptions in neutrophil functions, including chemotaxis, phagocytosis, and microbial killing capacity, thereby contributing to the higher infection risk and severity observed in T2D [35].
Evidence has also shown significant associations between various metabolites, such as C4DC, C8:1, C16OH, citrulline, and others, with the 10-year ASCVD risk score, suggesting that metabolomics could contribute to refining risk predictions [36].
In Europe, the SCORE model has recently been updated to SCORE2-Diabetes to better predict cardiovascular events in individuals with type 2 diabetes who have not yet developed ASCVD or severe organ damage. This updated model integrates both traditional and diabetes-specific risk factors, improving its accuracy in estimating 10-year CVD risk. By incorporating sex-specific, risk-adjusted models recalibrated to reflect current CVD incidence in different European regions, SCORE2-Diabetes provides more individualized risk assessments. Factors such as age at diabetes diagnosis, HbA1c, and estimated glomerular filtration rate (eGFR) are included to refine predictions. While SCORE2-Diabetes has shown modest improvement over the ADVANCE risk score, the inclusion of the cardio-ankle vascular index (CAVI) in the model did not significantly enhance individual risk categorization for T2DM patients [37]. In Table 1 we included a summary of the most used prognostic scoring models for patients with diabetes (Table 1).
Overview of prognostic scoring models: populations, variables, and clinical utility
| Scoring Model | Population | Variables included | Endpoint | Advantages | Limitations |
|---|---|---|---|---|---|
| Framingham Risk Score (FRS) [28] | General Population | Age, sex, smoking, systolic BP, total cholesterol, HDL cholesterol, diabetes | 10-year risk of coronary heart disease (CHD) | Simple, widely used, easy to calculate | Limited applicability to non-caucasian populations |
| Pooled Cohort Equations (PCE) [28] | General Population (Including African Americans) | Age, sex, total cholesterol, HDL cholesterol, systolic BP, smoking, diabetes, race | 10-year ASCVD risk (MI, Stroke, CHD death) | More inclusive, accounts for racial differences | Underestimates risk in younger and diabetic individuals |
| UKPDS Risk Engine [32] | Type 2 Diabetes Mellitus | Age, sex, diabetes duration, HbA1c, total cholesterol, systolic BP, smoking | Risk of CHD and stroke in diabetic patients | Specific for diabetics, includes glycemic control | Lacks imaging and novel biomarkers |
| ADVANCE Risk Score [32] | Type 2 Diabetes Mellitus | Age, sex, diabetes duration, smoking, systolic BP, cholesterol, prior CVD, medication use | 5-year risk of major cardiovascular events in diabetics | Incorporates prior CVD and treatment factors | Short-term risk prediction (5 years), lacks imaging integration |
| SCORE2-Diabetes [37] | Type 2 Diabetes Mellitus | Age at diabetes diagnosis, HbA1c, eGFR, total cholesterol, BP | 10-year risk of cardiovascular disease (CVD) in diabetics | Refined model for diabetics, considers renal function | Limited validation outside European populations |
| Polygenic Risk Scores (PRS) [29] | General Population (Genetic-based Risk) | Polygenic risk factors (genetic variants linked to ASCVD) | Lifetime genetic risk for ASCVD | Early risk detection, independent of traditional risk factors | Limited clinical integration, performance varies across ethnic groups |
ASCVD, atherosclerotic cardiovascular disease; BP, blood pressure; CHD, coronary heart disease; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; FRS, Framingham Risk Score; HbA1c, glycated hemoglobin; MI, myocardial infarction; PCE, Pooled Cohort Equations; PRS, Polygenic Risk Scores.
Cardiovascular complications in diabetes, particularly type 2 diabetes, include increased risks of coronary heart disease, stroke, heart failure, and microvascular conditions such as diabetic retinopathy. These complications are driven by hyperglycemia, hyperinsulinemia, dyslipidemia, and endothelial dysfunction, which accelerate atherosclerosis. Clinically, this underscores the importance of early and comprehensive risk assessment, aggressive management of glucose levels, lipids, and blood pressure, and lifestyle interventions to reduce cardiovascular events and improve patient outcomes (Figure 3).
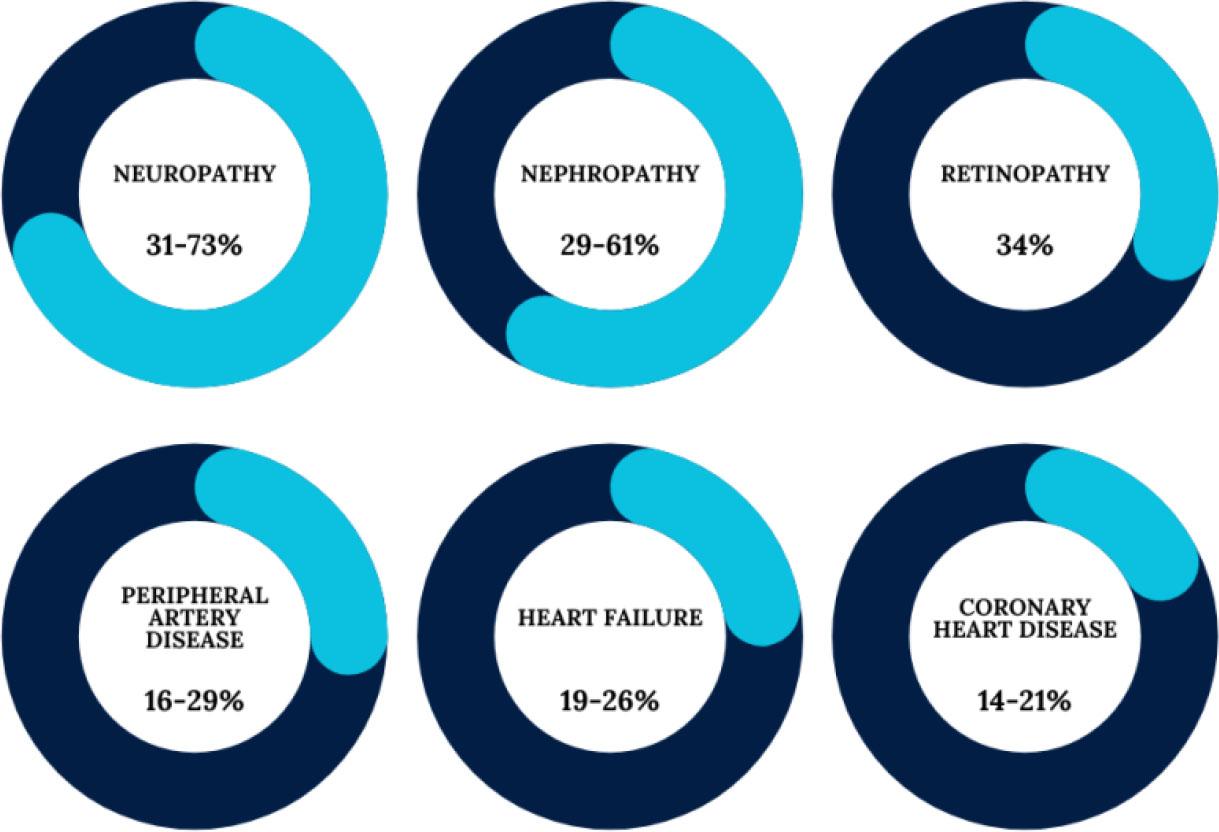
Prevalence of macrovascular and microvascular complications of diabetes.
Non-invasive imaging modalities present a compelling alternative approach for evaluating the susceptibility of atherosclerotic plaques and predicting the risk of future cardiovascular events. These advanced technologies enable the visualization and quantification of various pathological characteristics associated with atherosclerosis. Moreover, the integration of functional vascular assessments – such as the ankle-brachial index (ABI), flow-mediated dilation (FMD), carotid-femoral pulse wave velocity (cfPWV), and the arterial resistive index – can yield valuable insights into vascular function and arterial stiffness. Such assessments are instrumental in estimating the likelihood of cardiovascular events and in stratifying patient risk levels. However, current guidelines, including those from the European Society of Cardiology (ESC), do not endorse the routine use of tests like carotid intima-media thickness (cIMT) or functional testing for general cardiovascular risk evaluation, with the exception of identifying carotid plaque [38].
Having clinical manifestations in the carotid arteries and lower extremity arteries as much as in the coronary arteries, examining the walls of peripheral arteries and the measurement of the intima-media thickness could give us relevant information for estimating a risk profile and to promote early detection of the atherosclerotic burden [39].
Since its introduction in 1995, Computed Tomographic Coronary Angiography has undergone significant technological advancements, evolving into a sophisticated imaging modality. CCTA excels at detecting obstructive coronary artery disease (CAD), generating precise and detailed images of the coronary arteries. Furthermore, it is equipped to discern various characteristics of atherosclerotic plaques, including those indicative of high-risk plaques (HRP). Specifically, CCTA allows for the classification of high-risk plaques into three categories: calcified, non-calcified, and partially calcified, which consists of both calcified and non-calcified plaque tissues. Despite its capabilities, research indicates that CCTA's efficacy in distinguishing between lipid and fibrotic tissue components is some-what limited, primarily due to inadequate imaging resolution. Studies suggest that CCTA demonstrates good specificity but lacks sensitivity in accurately characterizing plaque phenotypes and identifying lesions that are susceptible to histological changes [40].
The adoption of CCTA has markedly increased in recent years. Initially utilized solely for assessing the anatomical features of the coronary tree, CCTA has expanded its applications to include the non-invasive measurement of coronary inflammation. Antonopoulos et al. proposed a hypothesis suggesting that inflamed arteries hinder the formation of lipid within the perivascular space. Computed tomography attenuation serves as a measurable imaging biomarker for indicating pericoronary inflammation, attributable to alterations in the lipid content of the surrounding adipose tissue. It is widely accepted that plaques situated at bifurcation points of the coronary arteries are subjected to endothelial shear stress, a mechanical force that may contribute to plaque rupture [41].
To comprehensively evaluate the relationship between plaque composition, endothelial shear stress, and the exact locations of plaque rupture within human coronary arteries, CCTA can be effectively combined with intravascular modalities such as intravascular ultrasound (IVUS) and OCT. Despite these advancements, it is critical to recognize that a significant proportion of acute coronary events can occur due to lesions that do not exhibit detectable high-risk features on CCTA. Moreover, notable limitations include exposure to radiation and the requirement for an iodinated contrast agent, which may pose risks for specific patient populations [42].
Research utilizing CCTA has established that lesions demonstrating modest progression over time are less likely to precipitate sudden coronary events, irrespective of their initial characteristics or the degree of vascular narrowing. Furthermore, the total burden of coronary plaque, assessed through CAC scoring or segment involvement score (SIS), has been shown to predict major adverse cardiovascular events (MACE) even among asymptomatic individuals. The integration of artificial intelligence (AI) into the analysis of CCTA images is increasingly prevalent, enhancing diagnostic accuracy, efficiency, and reducing human error – all without incurring additional costs or labor. Machine learning techniques, particularly those utilizing deep learning, can accurately quantify the extent of plaque and the degree of stenosis in CCTA images. These metrics have been externally validated and demonstrate robust agreement with evaluations conducted by skilled human readers as well as with findings from IVUS. Machine learning algorithms that amalgamate both clinical and CCTA data exhibit superior predictive capability for 5-year all-cause mortality compared to either dataset used independently. Additionally, algorithms focused on quantitative plaque features derived from CCTA have proven effective in forecasting ischemia, as indicated by functional fractional reserve (FFR) and compromised myocardial blood flow (MBF), as evaluated by positron emission tomography (PET). These scores have surpassed traditional CCTA assessments focused solely on stenosis [43]. CCTA enhances cardiovascular risk assessment in diabetic patients by identifying noncalcified and high-risk plaques that may be missed by coronary artery calcium (CAC) scoring. Patel et al. demonstrated a progressive increase in coronary atherosclerosis with worsening glycemic status, with 69% of diabetic patients exhibiting plaque compared to 43% in normoglycemic individuals. Notably, CCTA detected coronary plaques in 30% of diabetic patients with a CAC score of zero, underscoring the limitations of CAC in fully capturing cardiovascular risk. Furthermore, diabetes was associated with a threefold increase in severe coronary stenosis (≥50%), highlighting the need for advanced imaging to improve early detection of high-risk individuals. These findings support the use of CCTA for more accurate risk stratification, enabling earlier preventive interventions and improved cardiovascular outcomes in diabetic patients [44].
Magnetic Resonance Imaging presents an optimal method for conducting repeated and longitudinal assessments, primarily due to its absence of radiation exposure. This capability facilitates the monitoring of the progression of atherosclerotic plaques over time. Renowned for its exceptional ability to differentiate soft tissues, MRI produces high-resolution images that allow for precise evaluation of plaque dimensions and thickness. Moreover, MRI can effectively distinguish between the vessel's lumen and its outer wall. By employing various image weightings, including T1, T2, and proton density (PD), MRI enables the precise identification and analysis of vulnerable plaque components, such as intraplaque hemorrhage, lipid-rich necrotic cores, and thin fibrous caps. However, achieving high spatial resolution within the arterial wall poses a considerable challenge, particularly in small blood vessels, such as those found in the intracranial circulation. While three-dimensional (3D) imaging techniques are often regarded as superior, they can be time-consuming, lasting several minutes, which may be uncomfortable for patients and susceptible to motion artifacts caused by bodily movements or pulsatile flow. This can complicate assessments when a broader range of imaging sequences is necessary for distinguishing plaque characteristics. Utilizing high-resolution MRI to analyze plaque morphology may be constrained to a single plaque or vascular segment, creating challenges in assessing plaque characteristics across larger sections of the arterial tree. Furthermore, patients exhibiting claustrophobia or those with metallic implants, such as pacemakers, defibrillators, and certain aneurysm clips, must be excluded from MRI scanning due to safety concerns. An alternative approach for characterizing plaques involves the use of MRI contrast agents, such as gadolinium-based agents or iron oxides, to evaluate plaque permeability or the presence of inflammatory cells. However, it is crucial to recognize that these agents can accumulate in tissues over extended periods, raising safety concerns that may limit their future applications in clinical settings [45].
PET is a nuclear imaging modality that utilizes a radio-labeled molecular ligand (or tracer) injected into the body to assess cellular activity. This non-invasive technique is particularly valuable for evaluating biological processes associated with atherosclerosis, including arterial inflammation, hypoxia, neoangiogenesis and microcalcification. The most commonly employed tracer in PET imaging is 18F-fluorodeoxyglucose (18F-FDG), a glucose analogue that is radio-labeled and preferentially taken up by metabolically active cells, especially macrophages. Numerous studies investigating atherosclerosis in both humans and animal models have established a direct correlation between the amount of 18F-FDG accumulation in arterial walls and cellular glycolysis, which reflects the density of plaque macrophages and the level of inflammation. PET imaging holds promise for application in individuals with subclinical atherosclerosis. Recent investigations, including those by Fernández-Friera et al. and van der Valk et al., aimed to delineate thresholds for arterial inflammation associated with 18F-FDG uptake, revealing that over 52% of individuals exhibiting atherogenic risk factors demonstrated elevated tracer uptake. Notably, this research indicated that individuals classified as healthy, characterized by a calcium score of zero, exhibited significantly lower levels of arterial 18F-FDG uptake compared to those diagnosed with cardiovascular disease. The advantages of PET are largely attributed to its exceptional sensitivity and quantitative capabilities, allowing for the detection of tracer concentrations as low as picomolar levels. However, several limitations exist within the FDG-PET imaging technique. The spatial resolution, approximately 6 mm, poses challenges in directly assessing vulnerable plaques in smaller blood vessels, such as coronary arteries. Additionally, substantial cardiac and respiratory motion during coronary imaging can further degrade the PET signal, complicating evaluations of the middle to distal portions of coronary arteries. PET images are often combined with CT or MRI to enhance anatomical localization of the detected signals. Other limitations of PET include potential radiation exposure, the use of large and short-lived tracers, elevated costs, and limited availability compared to other imaging modalities [46].
Employing advanced imaging technology, IVUS allows for real-time visualization of vessel wall dimensions, phenotypic characteristics, distribution, and severity of atherosclerotic plaques. Additionally, grayscale IVUS can classify plaques based on their visual appearance and echogenicity relative to the surrounding adventitia. The classifications include soft plaque, fibrous plaque, calcified plaque, and mixed plaques. Recent advancements in IVUS technology, specifically in analyzing the intravascular ultrasound radiofrequency (IVUS-RF) backscatter signal, also referred to as virtual histology intra-vascular ultrasound (VH-IVUS), have facilitated the real-time visualization of vessels in three dimensions, enhancing the understanding of the composition and mechanical properties of unstable plaques. The PROSPECT study, the largest of its kind, utilized conventional angiography, grayscale IVUS, and VH-IVUS to evaluate the coronary vessels of 697 patients with acute coronary syndrome (ACS) following successful percutaneous coronary intervention (PCI) and during a subsequent follow-up period. This research revealed that IVUS was unable to visualize the entire coronary tree effectively, assessing only 53% of lesions responsible for severe cardiovascular events over a median follow-up of 3.4 years. Furthermore, multivariate analysis demonstrated a poor positive predictive value of merely 18.2% for identifying lesions that resulted in MACE throughout the follow-up period. Factors considered in this analysis included plaque load greater than 70%, a minimum luminal area of less than 4 mm2, and the presence of the thin-cap fibroatheroma (TCFA) phenotype [47].
Optical Coherence Tomography (OCT) is regarded as a more advanced in vivo imaging technology compared to IVUS for identifying vulnerable plaques associated with acute coronary syndrome. OCT offers enhanced specificity in analyzing plaque composition, particularly in distinguishing lipid-rich fibroatheromas and visualizing TCFA, both of which are critical markers of plaque vulnerability. This technology enables a precise assessment of cap disruption and erosion. Another study further validated the efficacy of OCT by demonstrating a strong correlation between OCT measurements and histological data, particularly regarding fibrous cap thickness, lipid core size, and the proportion of lipid content. Additionally, OCT has proven useful in quantifying macrophage presence within fibrous caps, which provides important insights into the inflammatory status of plaques — another key characteristic of plaque instability. Technologically, OCT surpasses IVUS with superior resolution (10–20 μm compared to IVUS’s 150–200 μm), a faster data acquisition rate, compact and cost-effective designs, and the capacity to image adjacent tissues without the interference of shadowing artifacts, especially beneficial when examining calcified deposits. Innovations in OCT have also led to improved imaging frame rates and resolution, as well as new contrast mechanisms to better define the collagen structure within fibrous caps. OCT’s advantage over IVUS lies in its ability to accurately assess the thickness, area, and volume of plaque calcification, categorizing calcifications into macrocalcifications, patchy calcifications, and microcalcifications. However, OCT's limitations include its shallow tissue penetration (2–3 mm), which can hinder accurate plaque burden estimation, and the attenuation of the optical signal by intraluminal blood, complicating clear visualization of the arterial wall. These challenges can be addressed through techniques such as index matching, saline flushes and balloon occlusion [48].
In contrast, Near-Infrared Spectroscopy (NIRS) has emerged over the past decade as a novel intravascular imaging method. NIRS analyzes the interaction between electromagnetic radiation and tissues based on wavelength, allowing rapid and simultaneous assessment of the arterial wall in both circumferential and longitudinal directions. Although NIRS reliably identifies lipid-core plaques, its widespread clinical application has been limited due to several constraints. NIRS focuses solely on lipid content without providing comprehensive morphological evaluation of the plaque. It cannot visualize the brightness of light, assess the external structure of the vessel, or measure plaque mass. Additionally, it struggles to accurately determine the depth of the plaque or distinguish between thin- and thick-cap fibroatheromas. Nevertheless, incorporating lipid-core burden assessment with NIRS may enhance the structural data provided by coronary angiography or IVUS, offering better identification of patients at risk and guiding the management of ACS [49].
Despite significant advancements in understanding the pathophysiology of atherosclerotic cardiovascular disease in diabetes, several limitations persist in the current approaches to risk assessment and management. Traditional risk scoring models, while useful, often fail to capture the complex pathophysiological mechanisms involved in plaque vulnerability and progression, particularly in diabetic populations. Non-invasive imaging techniques, such as cIMT and functional vascular assessments, while promising, are not yet widely recommended for routine clinical use due to limitations in sensitivity, specificity, and accessibility.
Current guidelines also highlight the need for more accurate tools to predict ASCVD risk in diabetic patients, especially younger individuals and those without established cardiovascular disease. Moreover, emerging technologies such as PRS and advanced imaging modalities (e.g., coronary artery calcium scoring, CCTA) have shown potential but require further validation in diverse populations and clinical settings. Integration of genetic, metabolic, and inflammatory biomarkers into risk models could provide a more personalized approach to risk stratification.
Future research should prioritize refining tools for early detection of subclinical atherosclerosis in high-risk populations, such as those with type 2 diabetes, and explore novel therapeutic strategies targeting insulin resistance, chronic inflammation, and oxidative stress. Additionally, RNA-based therapies, including small interfering RNA (siRNA) and messenger RNA (mRNA), offer potential for targeting specific inflammatory pathways in atherosclerosis, while genetic testing and polygenic risk scores can personalize risk prediction and optimize treatment, particularly for conditions like familial hypercholesterolemia and those requiring lipid-lowering therapies like PCSK9 inhibitors.
Furthermore, Genome-Wide Association Studies (GWAS) have contributed to developing polygenic risk scores, which estimate the overall genetic risk of ASCVD by considering the cumulative effect of multiple genetic variants. This can further personalize risk prediction and guide tailored preventive measures [50].
This review highlights the strong association between type 2 diabetes and accelerated atherosclerosis, driven by insulin resistance, chronic hyperglycemia, dyslipidemia, and systemic inflammation, all of which contribute to endothelial dysfunction, vascular remodeling, and an increased burden of high-risk coronary plaques. Despite advances in risk assessment and treatment, traditional models often fail to fully capture the complexity of diabetic atherosclerosis, leaving patients with significant residual cardiovascular risk.
Emerging imaging techniques and biomarkers offer potential for better detection and prediction of cardiovascular events in diabetic patients, but further research and validation are needed. Comprehensive risk management, integrating advanced screening tools and personalized interventions, is crucial for improving outcomes and reducing cardiovascular complications in this high-risk population.