Coronary artery disease (CAD) is a pathological condition that primarily affects the coronary arteries, often due to atherosclerosis. It is the leading cause of mortality globally, with one out of every six deaths related to CAD. The prevalence of subclinical CAD in middle aged population is more than it thought to be in recent studies[1].
Atherosclerosis is a pathological process which is responsible for coronary, cerebral and peripheral vascular diseases. Several factors are involved in the pathology of atherosclerosis, including: endothelial dysfunction, lipid disorders, inflammation, immunological factors and plaque rupture [2,3,4].
Endothelium plays a crucial role in regulating tone, growth, homeostasis and inflammation. Endothelial disorders are closely associated with several risk factors of atherosclerosis, including high cholesterol levels, diabetes, hypertension, and smoking [5].
Specifically, these factors lead to accumulation and modification of lipoprotein particles in the intima, followed by local cytokine release. This process results in endothelial dysfunction, platelet aggregation and therefore acceleration of atherosclerosis progression [6].
Smoking-related cardiovascular diseases are the leading causes of mortality and morbidity among smokers. A review of 10 cohort studies, covering more than 20 million person-years, revealed a 70% higher incidence of myocardial infarction and cardiovascular diseases in smokers compared to non-smokers [7].
Smoking can induce endothelial dysfunction by increasing adhesive molecules expression and reducing Nitric Oxide bioavailability. Additionally, smoking leads to platelet and macrophage aggregation, which is recognized as a pro-coagulation factor in the atherosclerosis process.
Smoking is responsible for 1 in 10 deaths and leads to the loss of 6 million lives worldwide each year [8].
About half a billion people currently alive face premature death from smoking unless they quit. The impact of smoking on atherosclerosis involves numerous biological and metabolic processes, such as endothelial damage, LDL oxidation, and clot formation [9].
Smoking results in a diverse range of CV diseases phenotypes. While some individuals only experience minor vascular effects from long-term smoking, others develop severe atherosclerotic disease even with minimal tobacco usage.
The connection between smoking and atherosclerosis implies that genetic and epigenetic backgrounds contribute to determining individuals’ susceptibility to the pro-atherogenic effects of smoking [10].
The levels of microRNA in the plasma of smokers serve as biomarkers and potential therapeutic targets [11].
MicroRNAs, small single-stranded non-coding RNAs, function by binding to messenger RNA and inhibiting protein translation, thereby regulating gene expression at the post-transcriptional level [9, 12,13,14]. So far, more than 1880 human microRNAs have been identified. MicroRNAs in endothelial cells, vascular smooth muscle, immune cells and platelets are involved in the initiation and progression of atherosclerosis [13]. Notably, several microRNAs, including 15a, 19a, 23b, 17–92, 21, 24, 92a, 101, 126, 145, 155, 205, 663 and 712, are widely expressed during atherosclerosis progression, while microRNA 29b, 24 and 365 play a key role in inhibiting atherosclerosis [12].
MicroRNAs, particularly 223 and 29b, serve as highly sensitive biomarkers for diagnosing CAD and play a critical role in the pathology of various cardiovascular diseases in smokers [10, 12]. Given the importance of CAD and the range of cardiovascular disease phenotypes in smokers, as well as the potential genetic and epigenetic factors, we were motivated to explore the impact of smoking on microRNAs associated with significant CAD.
This observational study was conducted on 60 individuals diagnosed with unstable angina who were referred to the catheterization laboratory of Rasul Akram Hospital and Rajaie Heart Center, Tehran, Iran. The individuals were categorized in four groups including non-smoker without significant CAD (S-A-), non-smokers with significant CAD (S-A+), smokers without significant CAD (S+A-) and smokers with significant CAD (S+A+).
The significant CAD was diagnosed through angiography with at least 75% stenosis in one of the coronary arteries [15]. Further categorization based on smoking status was smokers and former smokers who were defined as individuals that stopped smoking ≤ 5 years. Those who had never smoked or stopped smoking > 5 years were considered as non-smokers.
Upon selecting group members, they were surveyed using a checklist to collect information on smoking habits, encompassing type, quantity, and timing of their last cigarette. Furthermore, the levels of tar and nicotine in cigarettes were measured and treated as variables.
Under the supervision of a physician, venous blood samples were aseptically collected from each individual using a syringe. Approximately 3–5 ml of peripheral blood (PB) samples were drawn into anticoagulant-containing tubes, and the plasma was then separated, collected in RNase/DNase-free tubes, and stored at −70⁰C until extraction.
In accordance with the miRNA extraction kit protocol from Gene All Company, the extraction of all plasma microRNAs was conducted. To ensure the absence of DNA contamination and Phenolate or Thiol-Cyanates, the OD=A260/A280 and OD=A260/A230 ratios were measured using a spectrophotometer, with an absorbance lower than 1.8 considered acceptable.
The purified RNA underwent reverse transcriptase chain reaction (RT-PCR), with cDNA synthesis facilitated by a commercial cDNA synthesis kit incorporating specific primers for the desired microRNAs and normalization primers.
Subsequently, the Real Time PCR was conducted using Cyber Green SGqPCR Master Mix to measure the expression levels of miR-101, miR-199, miR-124-3p, miR-34, miR-126-5p, miR-223 and miR-223-5p. Ultimately, the acquired statistics and values were meticulously scrutinized and analyzed.
Patients with history of HTN, hypercholesterolemia, diabetes, renal failure, drug and opium usage, less than 45-year-old and those with family history of premature CAD were excluded.
When dealing with missing data in the cyclic threshold (CT) of gene expression, two strategies were employed. If there was no expression detection in any microRNAs or only one, the missing data were not replaced (considering as completely at-random pattern). In cases where detection for at least two microRNAs was present, the missing data were replaced by a maximum CT of 45 cycles. The rationale for the first strategy was attributed to quality or technical problems, while the second strategy was driven by significant down-regulation.
Following the selection of 60 cases for the pilot study, a sensitivity power analysis was conducted based on the observed standard deviation (SD), considering a group sample size of 15, a two-tailed alpha of 0.05, and a power of 0.8 (Table 1).
Sensitivity power analysis for comparison of two means
| MicroRNA | SD (∆CT) | Cohen’s d | Detectable ∆CT | Detectable FC |
|---|---|---|---|---|
| Mir-34a | 2.92 | 1.06 | 3.10 | 8.55 |
| Mir-34c | 3.19 | 1.06 | 3.38 | 10.42 |
| Mir-101 | 3.98 | 1.06 | 4.22 | 18.62 |
| Mir-124 | 2.38 | 1.06 | 2.52 | 5.75 |
| Mir-126-3p | 4.96 | 1.06 | 5.26 | 38.26 |
| Mir-126-5p | 4.04 | 1.06 | 4.28 | 19.46 |
| Mir-199 | 3.20 | 1.06 | 3.39 | 10.50 |
| Mir-223 | 4.03 | 1.06 | 4.27 | 19.32 |
The Cohen’s d 1.06 was obtained from group sample size 15, alpha 0.05 and power 0.8.
The CTs were normalized using mean of all the microRNAs’ CTs, and -∆CTs were then reported. A general linear model with analysis of variance (ANOVA) was employed to compare -∆CTs between the groups, with the group S-A- serving as the reference.
In this context, each beta coefficient was treated as -∆CT, and the fold change (FC) was derived by calculating two times the beta coefficient, along with reporting its 95% confidence interval (CI). It’s important to note that all the statistical analyses were carried out using R 4.0.0 (R foundation, Vienna, Austria).
A total of 60 individuals participated in this study including 18 cases of S-A- (30%), 14 cases of S+A- (23%), 12 cases of S-A+ (20%) and 16 cases of S+A+ (27%). There were 27 female cases (45%) and 33 male cases (55%). Mean age was 54.27±13.30 years. Mean BMI was 26.15±2.59 kg/m2. Among the 30 number of smokers (50%), the range of smoking start age was 16 – 40 years, the range of pack-year was 3.75 – 43, and the range of latest smoking time was 0.5 – 12 hours before. Among the 28 number of cases with significant CAD (47%), five cases (18%) had one-vessel disease (1VD), 12 cases (43%) had two-vessel disease (2VD) and 11 cases (39%) had severe vessel disease (SVD). According to our missing data management strategy, the missing data of four cases were not replaced and the other ones were replaced by 45 cycles.
The effects of study groups on gene expression was studied using general linear model considering S-A- group as the reference. The results of each microRNA are presented as the following (Table 2, Figure 1).
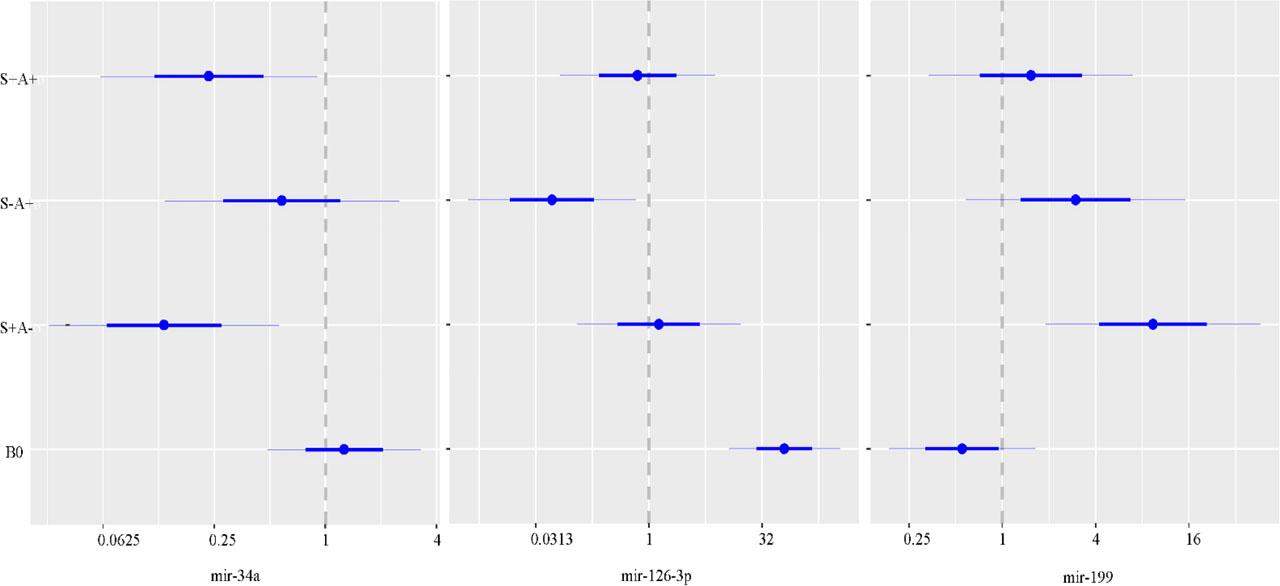
Coefficient plots showing FC and 95% CI (H0: FC =1, reference: S-A-) for the microRNAs having significant FC; B0: intercept of the models.
Gene expression study in among groups using general linear model
| MicroRNA | Group | FC (95% CI) | P value | R-square | ANOVA P value |
|---|---|---|---|---|---|
| Mir-34a | S-A- | Reference | 0.153 | 0.031* | |
| S+A- | 0.13 (0.03–0.56) | 0.007* | |||
| S-A+ | 0.58 (0.13–2.52) | 0.461 | |||
| S+A+ | 0.23 (0.06–0.91) | 0.036* | |||
| Mir-34c | S-A- | Reference | 0.043 | 0.507 | |
| S+A- | 0.95 (0.17–5.17) | 0.952 | |||
| S-A+ | 2.31 (0.41–13.06) | 0.336 | |||
| S+A+ | 2.52 (0.51–12.58) | 0.253 | |||
| Mir-101 | S-A- | Reference | 0.120 | 0.078# | |
| S+A- | 0.2 (0.03–1.44) | 0.107# | |||
| S-A+ | 2.87 (0.37–21.99) | 0.305 | |||
| S+A+ | 0.42 (0.06–2.76) | 0.358 | |||
| Mir-124 | S-A- | Reference | 0.115 | 0.094# | |
| S+A- | 0.79 (0.23–2.64) | 0.694 | |||
| S-A+ | 2.25 (0.65–7.76) | 0.195# | |||
| S+A+ | 0.47 (0.15–1.49) | 0.196# | |||
| Mir-126-3p | S-A- | Reference | 0.129 | 0.064# | |
| S+A- | 1.36 (0.11–16.76) | 0.806 | |||
| S-A+ | 0.05 (<0.01–0.67) | 0.024* | |||
| S+A+ | 0.71 (0.07–7.65) | 0.772 | |||
| Mir-126-5p | S-A- | Reference | 0.105 | 0.122 | |
| S+A- | 3.32 (0.42–26.31) | 0.250 | |||
| S-A+ | 0.27 (0.03–2.27) | 0.224 | |||
| S+A+ | 2.07 (0.29–14.74) | 0.461 | |||
| Mir-199 | S-A- | Reference | 0.146 | 0.040* | |
| S+A- | 9.38 (1.89–46.49) | 0.007* | |||
| S-A+ | 2.97 (0.58–15.26) | 0.187# | |||
| S+A+ | 1.53 (0.34–6.99) | 0.575 | |||
| Mir-223 | S-A- | Reference | 0.029 | 0.666 | |
| S+A- | 0.82 (0.09–7.04) | 0.852 | |||
| S-A+ | 1.88 (0.21–16.98) | 0.567 | |||
| S+A+ | 2.61 (0.34–20.12) | 0.350 |
Significant at P <0.05;
Trend for significance (P <0.1 for ANOVA, P <0.2 for FCs)
Mir-34a: Significant down-regulations were observed for S+A- (FC =0.13, P =0.007) and S+A+ (FC =0.23, P =0.036) groups. This pattern showed that smoking was in favor of down-regulation and significant CAD was in favor of moderation against down-regulation in the interaction with smoking. About 15.3% of the variation of gene expression could be explained by the study groups (ANOVA P =0.031).
Mir-34c: No significant variation was observed between the study groups (ANOVA P =0.507). No significant group comparison was observed (P >0.2).
Mir-101: A trend for significance was observed for the variation of the study groups (ANOVA P =0.078). In group comparisons, a trend for significance was observed for down-regulation in S+A- group (FC =0.20, P =0.107).
Mir-124: A trend for significance was observed for the variation of the study groups (ANOVA P =0.094). In group comparisons, trends for significance were observed for up-regulation in S-A+ (FC =2.25, P =0.195) and down-regulation in S+A+ (FC =0.47, P =0.196) groups.
Mir-126-3p: A trend for significance was observed for the variation of the study groups (ANOVA P =0.064). In group comparisons, a significance down-regulation was observed in S-A+ group (FC =0.05, P =0.024). This pattern showed that significant CAD was in favor of down-regulation and smoking was in favor of removing atherosclerosis effect in the interaction with it.
Mir-126-5p: A trend for significance was observed for the variation of the study groups (ANOVA P =0.122). No significant group comparison was observed (P >0.2).
Mir-199: A significant up-regulation was observed for S+A- group (FC =9.38, P =0.007). A trend for significance was observed for up-regulation in S-A+ group (FC =2.97, P =0.187). This pattern showed that smoking was in favor of up-regulation and significant CAD was in favor of removing smoking effect in the interaction with it. About 14.6% of the variation of gene expression could be explained by the study groups (ANOVA P =0.040).
Mir-223: No significant variation was observed between the study groups (ANOVA P =0.666). No significant group comparison was observed (P >0.2).
To account for potential confounders including age, sex, pack-year, and BMI, multivariable modeling was applied. Stepwise model selection (removal P >0.1) was utilized, with the study groups variable being held constant. As a result, no confounders were found for any of the models, confirming that the associations mentioned previously were not confounded.
The study involved the use of interaction models to examine the interaction between smoking (pack-year) and significant CAD across various scales (healthy, 1VD, 2VD and SVD). Consequently, it was suggested that the expression of mir-34a and mir-199 could be predicted by this interaction model (ANOVA P<0.2).
The only significant interaction was observed for mir-199, aligning with the primary findings. This interaction favored down-regulation, considering with the main effects favoring up-regulation. In essence, while the number of ≥75% stenotic vessels and pack-years led to up-regulation, their interaction resulted in down-regulation (Table 3).
Interaction of atherosclerosis and pack-years of smoking on the expression of microRNA using general linear model
| MicroRNA | Predictor | FC (95% CI) | P value | R-square | ANOVA P value |
|---|---|---|---|---|---|
| Mir-34a | Number vessels | 0.52 (0.36–1.11) | 0.111# | 0.115 | 0.089# |
| Pack-year | 0.90 (0.87–0.99) | 0.018* | |||
| Interaction | 1.05 (0.99–1.08) | 0.131# | |||
| Mir-199 | Number vessels | 2.37 (1.01–3.28) | 0.046* | 0.192 | 0.011* |
| Pack-year | 1.16 (1.04–1.19) | 0.002* | |||
| Interaction | 0.91 (0.90–0.98) | 0.006* |
Number of vessels: 0, 1, 2 and 3;
Significant at P <0.05;
Trend for significance (P <0.2); microRNAs with ANOVA P <0.2 were removed.
Utilizing a heat map, microRNAs and participants were simultaneously clustered. Initially, participants could not be effectively classified according to their group labels when considering all the microRNAs (Figure 2).
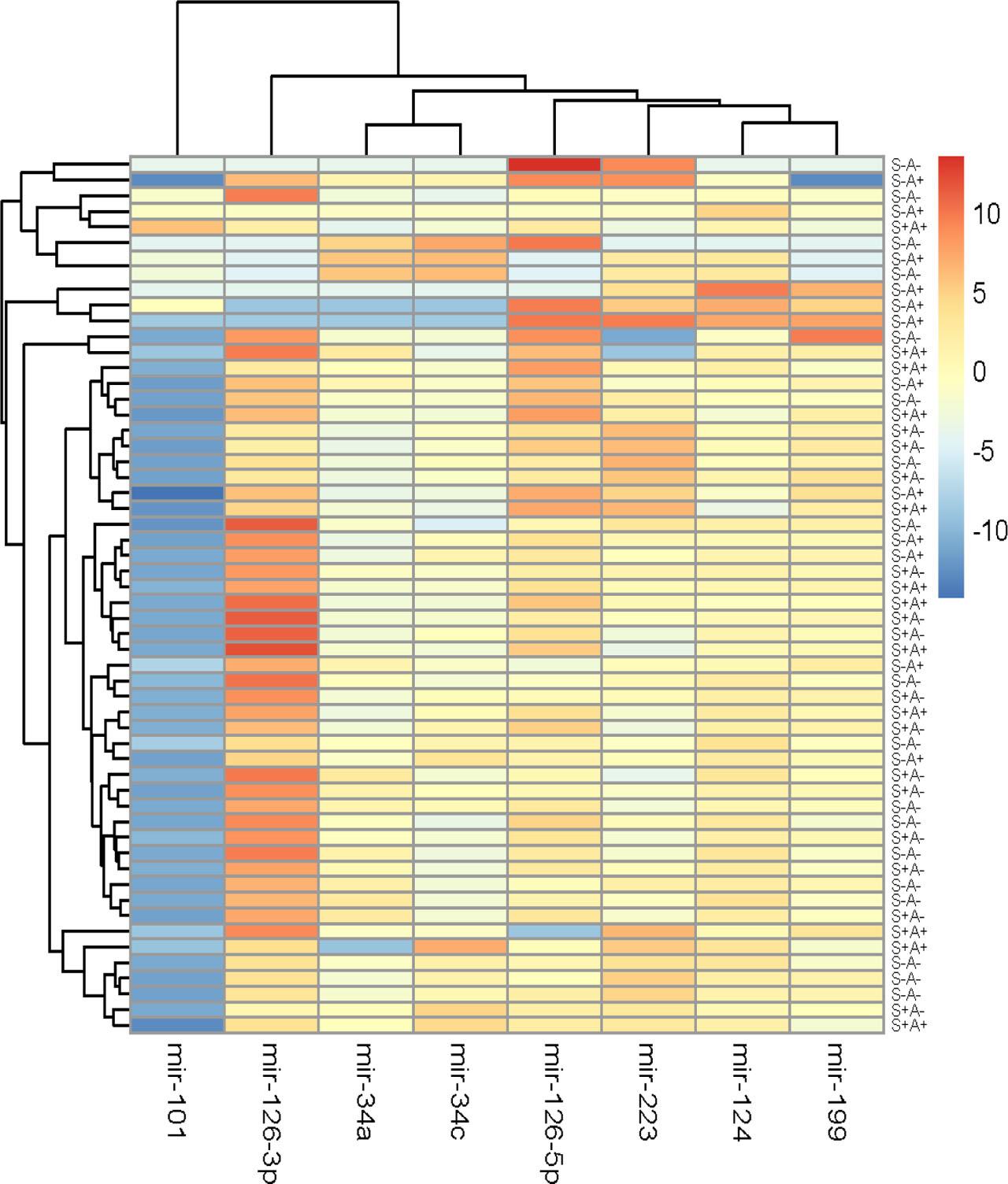
Heat map for simultaneous clustering of microRNAs and participants on the basis of -∆CT (i.e. red color: up-regulation).
However, following the removal of non-significant genes, the clustering of participants became more aligned with their group labels (Figure 3).
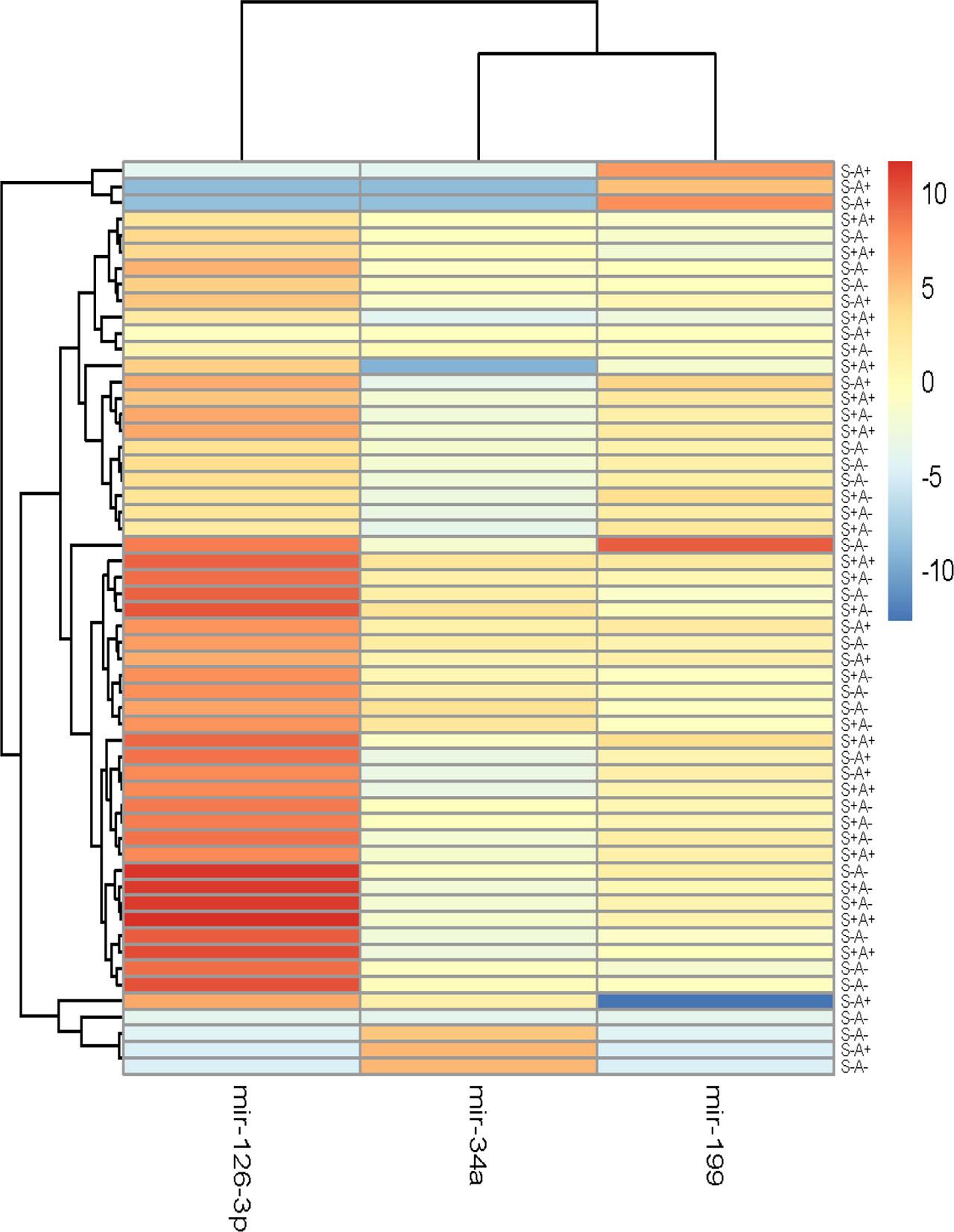
Heat map for simultaneous clustering of microRNAs and participants after removal of microRNAs with non-significant FCs on the basis of -∆CT (i.e. red color: up-regulation).
Smoking decreases anti-oxidants, leading to lipid peroxidation and atherosclerosis. As mentioned before, genetic background influences susceptibility to smoking’s pro-atherogenic effects [11, 16]. MicroRNAs are key players in controlling this process. Meanwhile, smoking triggers a significant rise in plasma microRNAs linked to the progression of atherosclerosis [17, 18]. The present study was conducted to investigate the roles of atherosclerosis, smoking and their interaction on a micro-RNA profile.
Mir-126-3p enhances the endothelial barrier’s strength and decreases vascular permeability via the ERK and AKT signaling pathways. It can also lead to reduction of lesion size and improvement of vascular repair. Notably, a clinical study observed a significant rise in plasma level of mir-126-3p in smokers [19] [20, 21] [22]. Our study found that non-smoking patients with coronary artery disease exhibited a decrease in mir-126-3p expression consistent with previous researches. However, in smoking patients with significant CAD, although there was a decrease in fold change, the results did not reach statistical significance.
The Tampere Vascular Study found that the expression of mir-34a in atherosclerotic arteries was 2.55 times higher than in Left Internal Thoracic Artery (as control vessel), highlighting a statistically significant up-regulation[23] Also in the study by Kalscheuer et al., mice exposed to 4-methylnitrosamino-1-(3-pyridyl)-1 butanone (NNK), a substance found in tobacco, exhibited a decrease in mir-34a expression in the lung tissue after NNK treatment [24]. The data analysis from our study indicated a significant decrease in mir-34a expression in smoking patients, regardless of coronary artery involvement. This reduction, believed to serve as a protective mechanism against the occurrence or progression of atherosclerosis. However, the reduction in mir-34a expression in all smoking patients suggests that mir-34a may not be a suitable biomarker for prediction of atherosclerosis in smokers.
Numerous studies have shown that down-regulation of mir-199 activates NF-kβ pathway and Ox-LDL uptake by vascular smooth muscle cells, leading to atherosclerosis progression. This reduction in mir-199 expression is associated with increased level of atherosclerosis biomarkers like Galectin-3, Neuropilin-1 and Angiogenin, a correlation that has been confirmed through autopsy analysis of coronary atherosclerotic plaques from patients who died because of acute coronary syndrome [25] [26, 27].
No study in the literature examined microRNAs in groups where all atherosclerotic risk factors except smoking were excluded. For instance, in XinXin Sun et al. study, they removed all atherosclerotic risk factors, including smoking. They defined atherosclerosis as carotid intima-media thickness (CIMT) ≥0.9 mm but <1.2 mm and identified reduced mir-199 expression as a predictor of asymptomatic atherosclerosis[28].
Other studies conducted in diabetic patients revealed a significant association between decreased mir-199 level and increased Hemoglobin A1C, endothelial dysfunction and lipid profile disorder. Consequently this led to the identification of mir-199 as predictor of MACE in diabetics [29, 30].
Our study revealed that upon excluding all conventional atherosclerosis risk factors except smoking, a significant increase in mir-199 expression was observed in smoking patients without evidence of ≥75% stenosis in coronary angiography. Conversely, in smoking patients with significant stenosis in CAG, no or minimal up-regulation was observed. Hence, it can be concluded that up-regulated mir-199 in smoking patients may exert protective effects against atherosclerotic coronary artery disease.
Park et al. concluded that Carvedilol usage, through the up-regulation of mir-199, can protect cardiomyocytes from ischemia-reperfusion injury. However, the utilization of mir-199 as a treatment target in smoking patients for prevention of atherosclerosis requires further studies. Nonetheless, this finding represents a positive step towards this goal in smoking patients [31].
In accordance with our expectations, the rise in pack-year of smoking correlates with a decrease in mir-34a expression and an increase in mir-199 levels. This phenomenon can be rationalized as a potential strategy for mitigating the advancement of atherosclerosis, as outlined in Table-3. Regarding mir-199, the up-regulation is significantly associated with the increase in the number of coronary arteries with significant stenosis. However, the interaction of both predictors (the number of involved vessels and pack-year) indicates a decrease in mir-199 expression, signifying the waning protective role of mir-199 upon the onset of advanced atherosclerosis. The findings from Table-2 further validate this issue, as up-regulation of mir-199 is significant in smoking patients without atherosclerosis, while it is minimal in smokers with significant CAD.
In conclusion, for smoking patients, up-regulation of mir-199 suggests a low probability of significant stenosis in the coronary arteries, while decrease in expression indicates a progression towards significant CAD (figure 4).
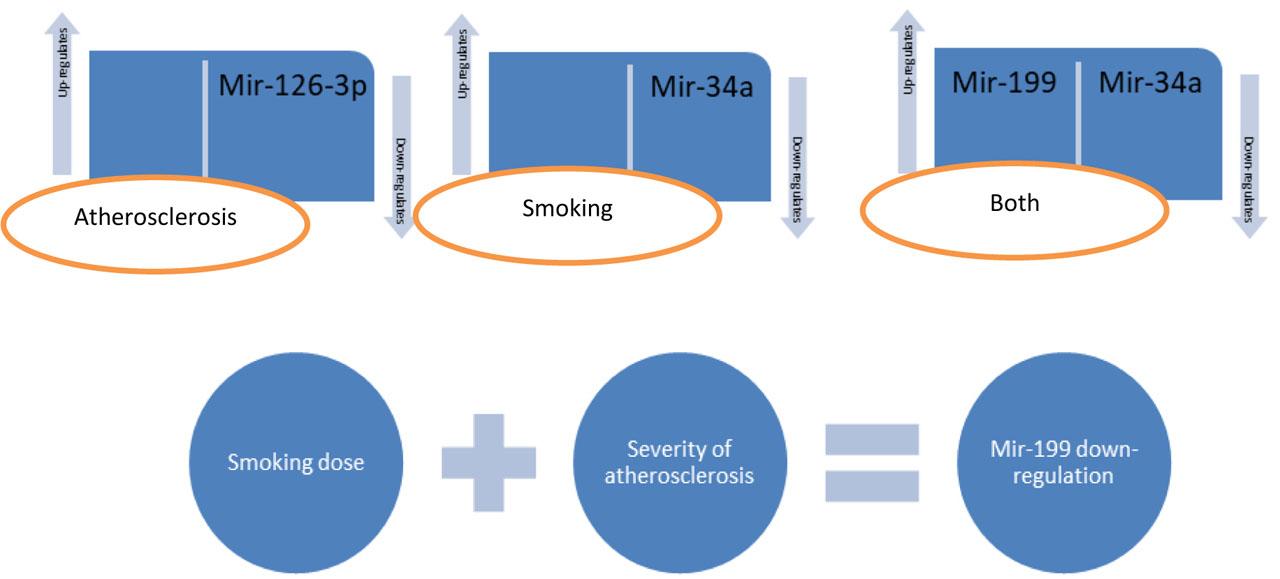
Mir-34a expression may be affected by smoking, whereas mir-126-3p expression may be affected by atherosclerosis. The significant down-regulation of mir-199 for the interaction of smoking dose and severity of atherosclerosis was a notable finding showing the harmful consequence of this interaction. Further studies are needed for this micro-RNA.
The key limitation was the constrained sample size due to financial restrictions, underscoring the critical need to reassess with a larger sample size for more comprehensive and reliable outcomes.