
Minimally invasive cardiac surgery (MICS) has revolutionized the management of mitral valve disease by minimizing surgical trauma, promoting faster postoperative recovery, and offering superior cosmetic outcomes compared to conventional median sternotomy [1]. The right-sided mini-thoracotomy, in particular, has emerged as a widely accepted MICS approach due to its ability to spare sternal disruption while maintaining adequate exposure [2]. Within this paradigm, two main incision techniques have been prevalent — submammary lateral thoracotomy and transaxillary thoracotomy — each with unique anatomical and functional implications. The submammary lateral thoracotomy is often favored for its incision placement beneath the inframammary fold, which provides superior aesthetic concealment, especially in women, potentially contributing to higher long-term cosmetic satisfaction [3].
By contrast, the transaxillary thoracotomy avoids the breast altogether, may entail less rib manipulation, and thus could reduce early postoperative pain; however, it involves an incision in a high-motion, moisture-prone region, which might be predisposed to delayed wound healing or sensory disturbances [4]. Post-thoracotomy pain remains a significant barrier to rapid recovery, driven largely by intercostal nerve irritation, rib retraction, and incision positioning [5]. Effective pain control is critical not only for patient comfort, but also for facilitating early mobilization and reducing pulmonary complications. Meanwhile, wound healing dynamics — shaped by factors like tissue tension, local humidity, and vascularization — vary between the inframammary and axillary sites, and may impact the rate of complications such as superficial surgical site infections (SSIs) or dehiscence [6].
Scar aesthetics significantly influence postoperative patient satisfaction, self-image, and quality of life, especially when involving visible areas of the body [7]. Despite these important considerations, direct comparative data between submammary and transaxillary thoracotomy in the context of MICS-MVR — particularly regarding postoperative pain trajectories, analgesic requirements, wound healing parameters, and scar outcomes — has been conspicuously limited. Existing literature tends to compare mini-thoracotomy to sternotomy, or examine analgesic techniques — seldom contrasts these two specific incision locations [8].To address this gap, we conducted a prospective comparative cohort study assessing postoperative pain (via visual analogue scale), opioid consumption, wound healing (Southampton grading and ASEPSIS scoring), and scar quality (patient and observer scar assessment scale, POSAS) between patients undergoing MICS-MVR with submammary or transaxillary approaches. We hypothesized that the transaxillary approach would be associated with lower early postoperative pain and opioid use, while the submammary incision would yield superior long-term cosmetic outcomes without compromising wound healing.
This was a prospective, comparative cohort study conducted at the Department of Cardiothoracic and Vascular Surgery at a tertiary center between January 2024 and July 2025. The study protocol was approved by the Institutional Ethics Committee and written informed consent was obtained from all participants prior to enrollment. The study adhered to the principles outlined in the Declaration of Helsinki.
Patient selection
Patients aged 18-70 years undergoing minimally invasive mitral valve replacement (MICS-MVR) via right mini-thoracotomy were eligible.
- Inclusion criteria were symptomatic severe mitral valve disease requiring replacement surgery, with left ventricular ejection fraction (LVEF) ≥ 40% and no history of previous right thoracic surgery.
- Exclusion criteria included concomitant cardiac procedures (e.g., tricuspid repair, CABG); active infection or immunosuppression; known allergy to local anesthetics or postoperative analgesics used in the study; and chronic pain syndrome or preoperative opioid use.
Eligible patients were allocated to one of two groups based on surgical approach:
- Group A: Submammary lateral thoracotomy; n = 40.
- Group B: Transaxillary thoracotomy; n = 40.
Allocation was performed in a quasi-randomized manner according to surgeon preference and patient anatomical suitability.
Both approaches were performed under general anesthesia with double-lumen endotracheal intubation to allow single-lung ventilation. Cardiopulmonary bypass was established via femoral artery and vein cannulation.
- Submammary lateral thoracotomy: 5–6-cm incision made along the inframammary crease, entering the fourth intercostal space.
- Transaxillary thoracotomy: 5–6-cm incision made along the midaxillary line in the hair-bearing region, also entering the fourth intercostal space.
Care was taken in both groups to minimize rib spreading and avoid unnecessary intercostal nerve injury.
Both approaches were performed under direct vision with video assistance. No fully endoscopic or micro-invasive port-only techniques were used in this cohort. A soft-tissue retractor (Alexis, Applied Medical, Rancho Santa Margarita, USA) was used initially, followed by a low-profile thoracic retractor as needed. Although both approaches sought to minimize rib retraction, it could not be completely avoided. The maximum estimated rib separation was kept between 1.5 and 3.0 cm in both groups. Intercostal nerve preservation was attempted by avoiding electrocautery near the inferior rib margin. Cardiopulmonary bypass and aortic cross-clamp times were recorded, and did not differ significantly between groups. Perfusion pressure, temperature management, and anesthetic protocols were standardized to reduce variability in nociceptive response.
Postoperative pain intensity was assessed using a visual analogue scale (VAS) ranging from 0 (no pain) to 10 (worst pain imaginable). Measurements were taken at:
6 hours post-extubation.
24 hours.
48 hours.
72 hours.
Postoperative day (POD) 7.
One-month follow-up.
Total opioid consumption (converted to intravenous morphine equivalents) was recorded for the first 72 postoperative hours.
Wound healing was evaluated by an independent surgeon (blinded to the incision type) using the Southampton wound grading system (grades 0–5) and ASEPSIS score (with ≤10 as satisfactory healing, and > 10 as impaired healing). Assessments were performed at POD 7, one month, and three months.
Scar quality was evaluated at three months post-surgery using the patient and observer scar assessment scale (POSAS), which considers vascularity, pigmentation, thickness, relief, pliability, and surface area (observer scale), as well as pain, itching, and overall satisfaction (patient scale).
Continuous variables were expressed as mean ± standard deviation (SD) and compared using the Student’s t-test or Mann-Whitney U test, depending on normality. Categorical variables were expressed as percentages and compared using the chi-square or Fisher’s exact test. Pain scores over time were compared using repeated-measures ANOVA. A p-value < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 2.0.
A total of 80 patients were included (n = 40 per group). Baseline demographic and preoperative clinical parameters were comparable between the submammary and transaxillary thoracotomy groups (Table 1). Additional preoperative variables relevant to postoperative pain and wound healing — including smoking status, pulmonary function (predicted FEV1%), baseline inflammatory markers (CRP and total leukocyte count), nutritional indicators (serum albumin and BMI stratification), and thoracic/breast anatomical characteristics (chest wall configuration, breast size category, and intercostal space width) — were comparable between groups. There were no statistically significant differences in mean age, sex distribution, BMI, comorbidities (hypertension, diabetes, chronic obstructive pulmonary disease), NYHA class, or left ventricular ejection fraction (all p > 0.05).
Baseline characteristics of study participants.
| Variable | Submammary (n = 40) | Transaxillary (n = 40) | p-value |
|---|---|---|---|
| Age (years), mean ± SD | 48.6 ± 9.2 | 47.8 ± 8.5 | 0.68 |
| Female sex, n (%) | 28 (70.0) | 26 (65.0) | 0.63 |
| BMI (kg/m2), mean ± SD | 24.3 ± 2.8 | 24.0 ± 2.9 | 0.71 |
| NYHA Class III/IV, n (%) | 15 (37.5) | 17 (42.5) | 0.65 |
| LVEF (%), mean ± SD | 56.2 ± 5.1 | 55.8 ± 4.9 | 0.73 |
| Diabetes mellitus, n (%) | 8 (20.0) | 9 (22.5) | 0.79 |
| Hypertension, n (%) | 10 (25.0) | 11 (27.5) | 0.80 |
| Smoking status (Current/Former/Never) | 3 / 6 / 31 | 4 / 5 / 31 | 0.87 |
| FEV1 (% predicted), mean ± SD | 82.4 ± 7.8 | 83.1 ± 8.1 | 0.72 |
| Serum albumin (g/dL), mean ± SD | 3.8 ± 0.4 | 3.7 ± 0.5 | 0.50 |
| CRP (mg/L), mean ± SD | 4.6 ± 1.2 | 4.4 ± 1.3 | 0.52 |
| Breast size category (S/M/L)* | 10/14 / 4 | 11 / 12 / 3 | 0.91 |
| Intercostal space width (cm), mean ± SD | 2.1 ± 0.4 | 2.0 ± 0.5 | 0.33 |
| Chest wall shape (Normal/Barrel/Pectus Excavatum) | 34 / 4 / 2 | 33 / 5 / 2 | 0.88 |
Assessed in female patients only
At 24 hours postoperatively, mean VAS pain scores were significantly lower in the transaxillary group compared to the submammary group (Table 2, Figure 1; 5.1 ± 1.0 vs. 6.3 ± 1.2; MD -1.2; 95% CI: -1.7 to -0.7; p < 0.001; Cohen’s d = 1.05, large effect size). At 48 hours, the difference remained significant (3.9 ± 0.9 vs. 4.5 ± 1.0; MD -0.6; 95% CI: -1.1 to -0.1; p = 0.01; d = 0.62). By 72 hours, the pain scores had converged (2.8 ± 0.8 vs. 3.0 ± 0.9; MD -0.2, 95% CI: -0.6 to -0.2; p = 0.28).
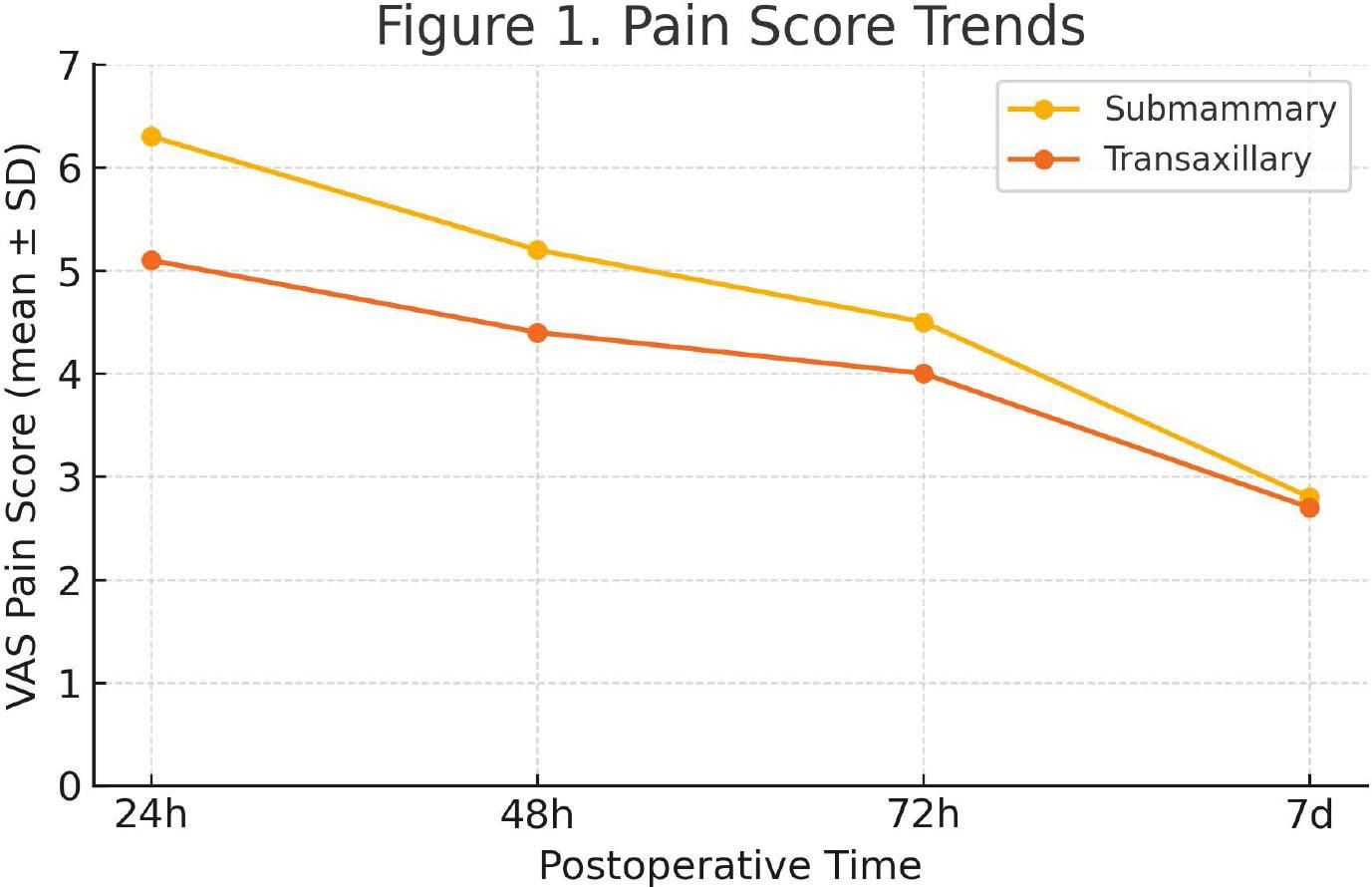
Line graph showing mean VAS pain score trends over 72 hours, with 95% CI error bars.
Postoperative pain scores (VAS) at 24, 48, and 72 hours.
| Time point | Submammary (mean ± SD) | Transaxillary (mean ± SD) | p-value |
|---|---|---|---|
| 24 hours | 6.3 ± 1.2 | 5.1 ± 1.0 | <0.001 |
| 48 hours | 5.2 ± 1.1 | 4.4 ± 1.0 | 0.002 |
| 72 hours | 4.5 ± 0.9 | 4.0 ± 0.8 | 0.010 |
| 7 days | 2.8 ± 0.7 | 2.7 ± 0.6 | 0.47 |
Cumulative morphine-equivalent opioid use in the first 72 hours was significantly lower in the transaxillary group (38 ± 10 mg) compared to the submammary group (Table 3; 46 ± 12 mg; MD -8 mg; 95% CI -13 to -3; p = 0.002; d = 0.72).
Opioid consumption within first 72 hours (morphine equivalents).
| Variable | Submammary (n = 40) | Transaxillary (n = 40) | p-value |
|---|---|---|---|
| 0-24 hours | 18 ± 5 | 15 ± 4 | 0.004 |
| 24-48 hours | 16 ± 4 | 13 ± 3 | 0.002 |
| 48-72 hours | 12 ± 3 | 10 ± 3 | 0.006 |
| Total (0-72 hours) | 46 ± 12 | 38 ± 10 | 0.002 |
At seven days post-procedure, 92.5% of patients in the transaxillary group and 85% in the submammary group had Southampton wound grades I-II (Table 4; risk difference 7.5%, 95% CI: -7.0% to 22.0%; p = 0.32). ASEPSIS scores were low and not significantly different between groups (3.1 ± 1.2 vs. 3.4 ± 1.5; p = 0.41). Minor wound complications occurred in three patients in the transaxillary group vs. five in the submammary group (p = 0.45), with no deep infections reported.
Wound healing outcomes (Southampton grades, ASEPSIS scores, and complications).
| Parameter | Submammary (n = 40) | Transaxillary (n = 40) | p-value |
|---|---|---|---|
| Southampton grade I-II, day seven, n (%) | 34 (85.0) | 37 (92.5) | 0.32 |
| Minor wound complications, n (%) | 5 (12.5) | 3 (7.5) | 0.46 |
| Deep infection, n (%) | 0 (0) | 0 (0) | – |
| ASEPSIS score, mean ± SD | 6.4 ± 1.8 | 6.0 ± 1.6 | 0.29 |
At three months, the submammary group demonstrated significantly better POSAS scores (Table 5, Figure 2; 14.2 ± 3.5 vs. 17.8 ± 4.2; MD -3.6; 95% CI: -5.3 to -1.9; p < 0.001; d = 0.93). Cosmetic satisfaction scores were higher in the submammary group than in the transaxillary group (4.6 ± 0.5 vs. 4.2 ± 0.6; MD 0.4; 95% CI: 0.1 to 0.6; p = 0.004; d = 0.72).
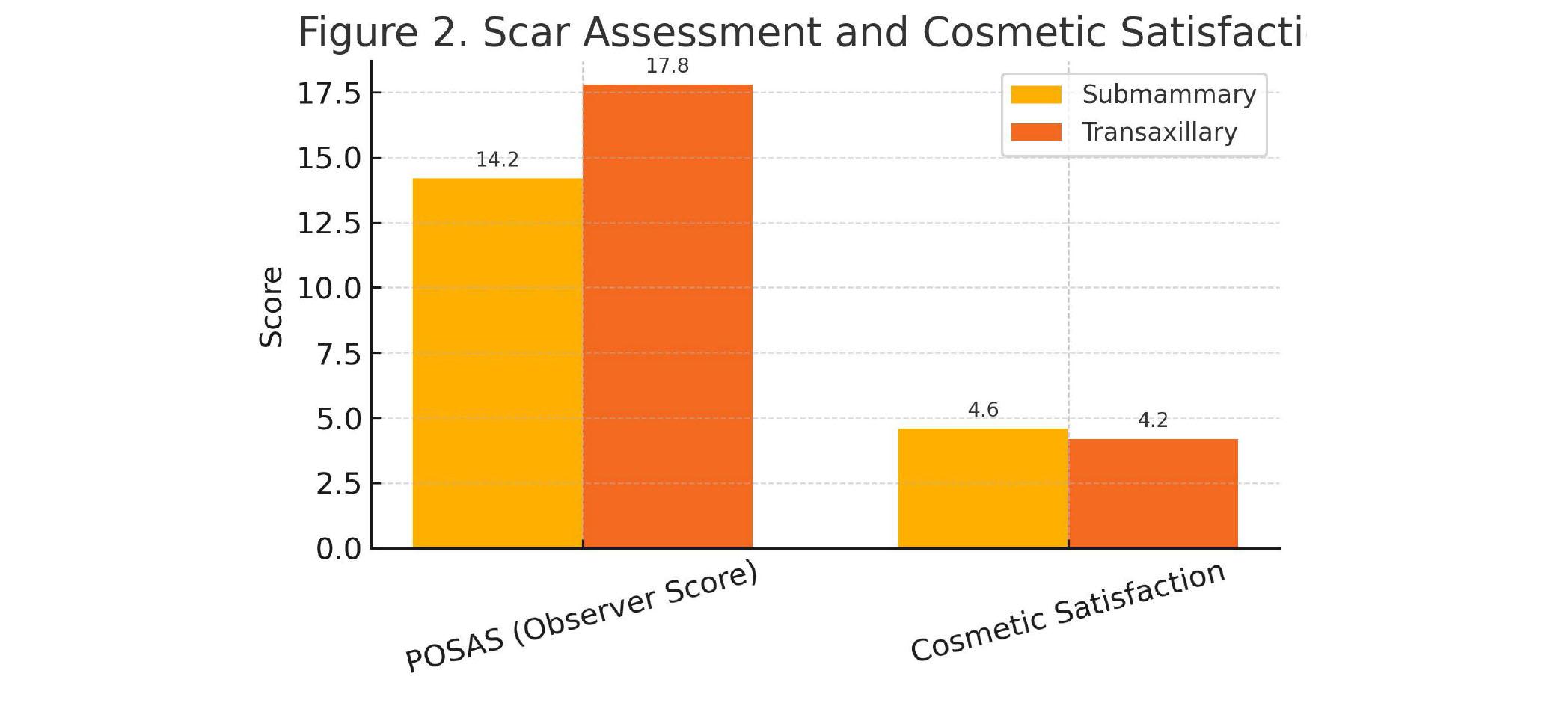
Bar chart comparing POSAS and cosmetic satisfaction scores between groups.
Scar quality (POSAS) and cosmetic satisfaction at three months.
| Parameter | Submammary (n = 40) | Transaxillary (n = 40) | p-value |
|---|---|---|---|
| POSAS total score (observer), mean ± SD | 14.2 ± 3.5 | 17.8 ± 4.2 | < 0.001 |
| Patient-reported cosmetic satisfaction (1–5) | 4.6 ± 0.5 | 4.2 ± 0.6 | 0.004 |
Our findings highlight distinct trade-offs between submammary lateral thoracotomy and transaxillary thoracotomy in MICS-MVR with regard to both anatomical and surgical access considerations. The lower early postoperative pain scores and reduced opioid consumption observed in the transaxillary group are consistent with prior studies suggesting that avoiding direct dissection through the breast tissue and pectoralis major reduces nociceptive stimulation of the intercostal nerves [1,2]. The lateral submammary incision, while cosmetically favorable in many female patients, requires mobilization of soft tissue and may involve more rib spreading, which both contribute to higher acute pain [3]. Pain in the early postoperative period is a multifactorial outcome, influenced not only by incision location but also by rib retraction mechanics, intercostal nerve handling, and the degree of periosteal stripping [4] In transaxillary access, the oblique trajectory and higher intercostal space utilization may preserve more costal cartilage integrity, potentially explaining the lower VAS scores and opioid needs in our transaxillary cohort.
Comparable patterns have been noted in minimally invasive aortic valve surgeries, where alternative incisions sparing major chest wall musculature have also yielded reduced analgesic requirements [5]. The wound healing outcomes, measured by Southampton grade and ASEPSIS score, were broadly similar between the two approaches, suggesting that tissue perfusion and surgical closure techniques are the dominant determinants in uncomplicated cases [6]. Minor superficial wound complications were more frequent in the submammary group, though not this was statistically significant; this aligns with reports that incisions within or beneath the breast may be more prone to localized moisture retention and friction [7]. However, no deep sternal or thoracic infections were observed, reflecting the generally low infection risk in MICS when strict asepsis is maintained [8].
Scar quality, as evaluated by POSAS, demonstrated better long-term outcomes in the submammary group. This is likely due to the natural concealment of the scar within the inframammary fold and its reduced exposure to UV radiation, both of which enhance cosmetic integration [9]. In contrast, the axillary scar, though hidden when the arm is at rest, may undergo stretching and pigmentation changes during shoulder movement, leading to higher observer and patient scores for scar visibility [10]. Similar cosmetic advantages for submammary access have been reported in reconstructive breast surgery literature [11], underscoring the role of incision site in patient satisfaction even when functional recovery is equivalent.
The observed superiority of submammary POSAS scores appears to be multifactorial. The submammary incision aligns more closely with Langer’s tension lines, and benefits from natural breast coverage, reducing ultraviolet exposure and mechanical shear. In contrast, the axillary region is characterized by greater moisture, multidirectional shoulder mobility, and higher risk of traction-related scar stretching. Additionally, sensory alterations arising from intercostobrachial nerve traction in the axilla may influence patient-reported scar perception. Notably, patient-reported POSAS components (pain, itching, satisfaction) differed from the transaxillary group more markedly than observer components, underscoring the subjective nature of the sensory impact of axillary incisions.
From a surgical-ergonomics perspective, transaxillary access may present a steeper learning curve due to limited exposure, particularly in patients with high body mass index or deep chest cavities [12]. Conversely, submammary incisions offer more direct visualization of the mitral apparatus, potentially reducing cross-clamp and bypass times in less-experienced hands [13]. Thus, surgeon preference and institutional expertise remain important determinants in selecting an approach.
This study directly compares two cosmetically favorable, minimally invasive access routes for MVR in a prospective fashion, incorporating both subjective patient-reported outcomes and objective ones (VAS, ASEPSIS, Southampton, and POSAS). The standardized perioperative analgesia protocol minimized confounding from variations in pain management, and the same surgical team performed all procedures, reducing operator-related bias. Follow-up was also extended to 6 months to capture both shortterm recovery and long-term scar outcomes.
Despite these strengths, certain limitations should be acknowledged. First, a major limitation of the present study was the use of rib retractors in both approaches. Rib retraction is a dominant determinant of postoperative pain, but no objective method exists to quantify the exact degree of rib spreading intraoperatively. Although retraction was minimized by protocol, variation in thoracic compliance and traction angles may have influenced early pain outcomes. Second, the sample size, though adequate for primary endpoints, limits subgroup analyses such as sex-based differences or the influence of breast size on wound healing [14]. Third, the study was conducted at a single high-volume center with considerable MICS experience, which may limit its generalizability to centers that are in the earlier phases of adopting these approaches. Fourth, the non-randomized design could introduce selection bias, even though baseline characteristics were comparable. Fifth, long-term functional outcomes beyond six months, including chronic pain syndromes and mitral valve durability, were not evaluated. Finally, scar assessment, though performed using validated scales, retains an element of subjectivity that can be influenced by patient expectations [15]. Future studies ideally should employ a completely endoscopic, rib-sparing approach to eliminate this confounder and isolate the effect of incision location alone.
Taken together, our data reinforce the principle that no single MICS-MVR approach is universally superior; the choice should be individualized. Patients prioritizing early postoperative comfort may benefit from a transaxillary incision, whereas those concerned with long-term scar concealment may prefer a submammary route. Future multi-center randomized trials with long-term follow-up are warranted to confirm these findings and explore adjunctive measures — such as intercostal cryoablation, minimally traumatic retractors, and advanced wound closure systems — to optimize both functional and cosmetic outcomes [16,17]. A fully endoscopic, rib-retraction-free MICS-MVR model may provide a superior platform for incision-only comparisons, and our group is exploring feasibility of such a protocol for future randomized trials.